1431
A contact-free signal and power transfer system.1Bernard and Irene Schwartz Center for Biomedical Imaging, Department of Radiology, New York University Grossman School of Medicine, New York, NY, United States, 2Center for Advanced Imaging Innovation and Research (CAI2R), Department of Radiology, New York University Grossman School of Medicine, New York, NY, United States, 3Siemens Healthcare GmbH, Erlangen, Germany, 4Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, China
Synopsis
Keywords: RF Arrays & Systems, RF Arrays & Systems
Motivation: Wireless MRI signal transfer reduces the need for physical cabling that can complicate patient table design and impede local coil preparation. Proposed techniques to eliminate cabling can involve complex subsystems for clock synchronization, high-fidelity ADC, low EMI, and high-speed data transfer.
Goal(s): Our goal was to implement a short distance contact-free signal and power transfer system without complex circuitry.
Approach: We designed a system to eliminate coil-to-scanner connections by transferring coil signals and preamplifier power over short distances using inductively coupled loops.
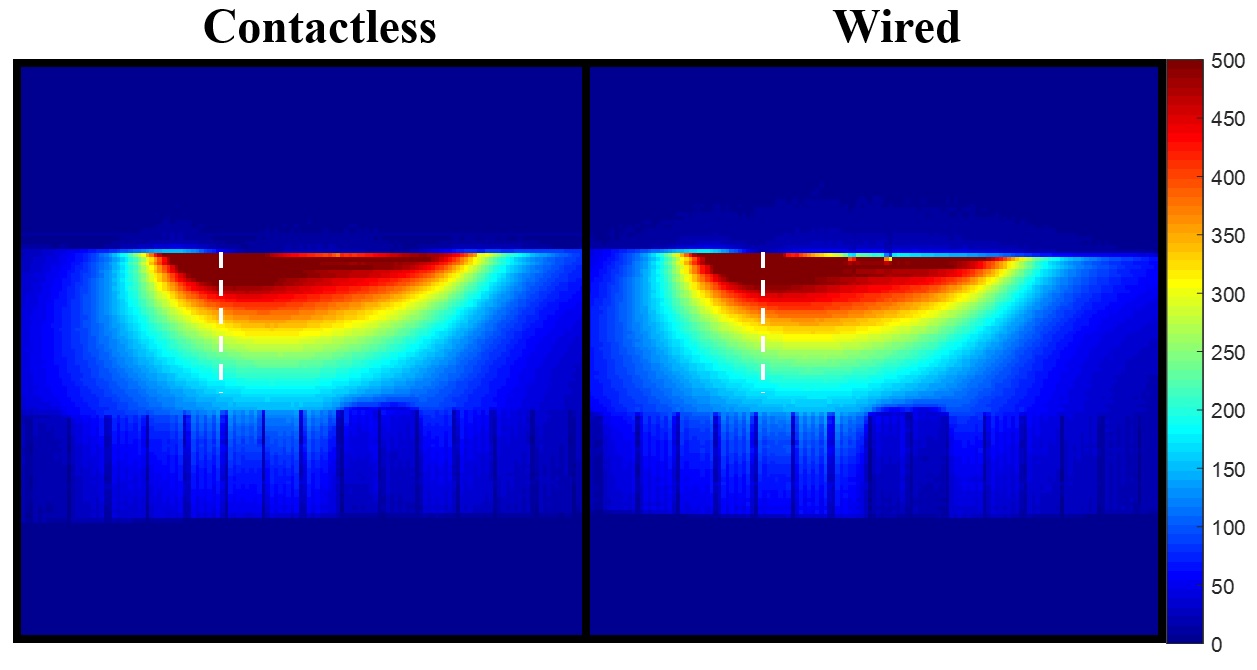
Results: SNR in images acquired with the contact-free and traditional (wired) systems were within 3-5%.
Impact: The proposed contact-free signal and power transfer system eliminated the physical connection between the coil and scanner while maintaining SNR, which opens the door to wireless coils and more robust and low-cost, detachable patient tables.
Introduction
Wireless MRI reduces the need for cable connections between the coil and table that can be failure-prone and impede patient setup. Promising systems eliminate cabling altogether by performing “on-coil” sampling, digitizing, and wireless transfer but involve complexities such as clock synchronization, high-speed and high-resolution digitization, EMI shielding, and require relatively large power consumption1,2. We developed an alternative contact-free signal and power system to transfer pre-amplified and frequency down-converted coil signals over short distances via coupled loops3 that did not require complex subsystems and had low power and EMI shielding requirements.Methods
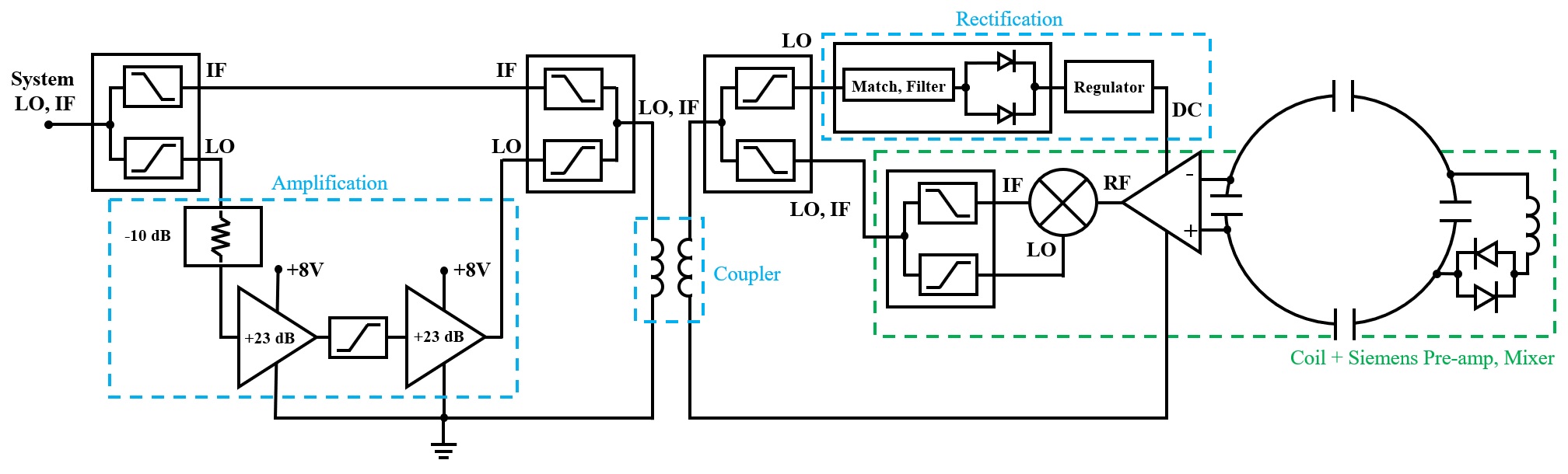
The contact-free system featured a pair of inductively coupled loops (Figure 1). The system was designed to operate on a 1.5T scanner equipped with “Tim 4G” RF architecture (MAGNETOM Sola, Siemens Healthcare, Erlangen, Germany), which is advantageous for short distance transfer because RF coil signals are down converted to intermediate frequencies (IF) via on-coil mixers driven by scanner-provided local oscillators (LO). Therefore, signal transfer can take place via inductive coupling at IF, rather than RF, which reduces the possibility of oscillation and interference with the system body or local coils. At the same time, the mixer LO served as a wirelessly accessible power source for the coil preamplifier. This was arranged by amplifying (PHA-13HLN+) the LO on the scanner-side after isolating it from IF using a home-built diplexer. The amplified LO and IF signals were recombined and inductively transferred to the coil-side using a home-built coupler consisting of two 3-turn loops with 2.5cm outer diameter that were separated by 5mm. The coupler was designed for low-loss LO and IF transfer, while blocking other frequencies including RF. On the coil-side, the amplified LO was again isolated from IF using a diplexer, rectified (PMEG2005CT), and fed to a voltage regulator (LD3985M30R) to power the preamplifier (Siemens Healthcare). The same diplexer was arranged to “leak” attenuated LO to the on-coil mixer. The coil itself was tuned and matched to 63.6MHz using conventional techniques with the exception of detuning, which was achieved using passively triggered diodes (UM9989) to avoid the need for (wired) active detuning. Thus, the coil-side modules were connected to the scanner-side in a completely contact-free manner. S-parameters were measured to evaluate the diplexers and coupler. The contact-free system was tested by comparing SNR in images acquired with the same coil and preamplifier wired directly to the scanner.Results
The diplexers provided approximately 25dB isolation between LO and IF with 0.3dB insertion loss through the individual arms. The coupler module had average 2.0dB insertion loss for LO and 2.5dB for IF. Total loss in the IF pathway between the coil-side diplexer and scanner socket was about 5dB. The scanner-side power requirement was approximately 3.2W primarily to drive the LO amplifiers, whose output was ~28dBm. The LO was rectified to DC at about 74% efficiency, resulting in a total system efficiency of 43%, which was sufficient to power the coil-side electronics (~0.26W). The SNR in the image acquired with the contact-free system was within 3-5% to that acquired with the traditional (wired) setup (Figure 2). There were no visible differences in image quality.Discussion
We designed and implemented a system that eliminated physical connections between the coil and scanner with minimal SNR loss (3-5%) compared to a wired setup. The product preamplifier in our system had 25-30dB gain and a 0.50dB noise figure. The addition of the diplexer and coupler chain added about 5dB loss that degraded the cascaded noise figure by a negligible 0.01dB, to a total of 0.51dB. A unique aspect is that the scanner-provided LO was used to power the coil preamplifier, eliminating the requirement for “RF-harnessed” or battery power.The described prototype system was designed for contact-free transfer over millimeter distances. The distance of transmission scales with the coupler loop diameter, which could be customized depending on the application. It could potentially eliminate table cabling by placing coil-side couplers at known locations on the table that align with scanner-side couplers in the bore. It could be envisioned for coils such as the spine, head, and breast that are typically fixed to the patient table. On the other hand, it may be challenging to align couplers in the case of flexible cardiac or abdominal coils.
Conclusion
The contact-free signal and power transfer system represents a cost-effective and robust alternative to the failure-prone coaxial connectors between the table and scanner interface that could reduce local coil setup time and facilitate detachable and robust yet inexpensive tables. Remaining challenges include implementing wireless active coil detuning and expanding the system to support multiple coils.Acknowledgements
This work was performed under the rubric of the Center for Advanced Imaging Innovation and Research (CAI2R, www.cai2r.net), an NIBIB National Center for Biomedical Imaging and Bioengineering (NIH P41 EB017183).References
1. Nohava L, Ginefri JC, Willoquet G, Laistler E, Frass-Kriegl R. Perspectives in Wireless Radio Frequency Coil Development for Magnetic Resonance Imaging. Front Phys. 2020;8. doi:10.3389/fphy.2020.00011
2. Darnell D, Truong TK, Song AW. Recent Advances in Radio-Frequency Coil Technologies: Flexible, Wireless, and Integrated Coil Arrays. J Magn Reson Imaging. 2022;55(4):1026-1042. doi:10.1002/jmri.27865
3. Bulumulla SB, Fiveland E, Park KJ, Foo TK, Hardy CJ. Inductively coupled wireless RF coil arrays. Magn Reson Imaging. 2015;33(3):351-357. doi:10.1016/j.mri.2014.12.004
Figures