1420
Adaptable Twenty-Channel Supine Breast Coil for MRI1GE HealthCare Coils, Aurora, OH, United States
Synopsis
Keywords: RF Arrays & Systems, RF Arrays & Systems
Motivation: Conventional MRI breast screening is performed in the prone position with rigid RF coils. These coils are uncomfortable and imaging area limited by patient size and positioning.
Goal(s): Our goals were to improve patient comfort, accommodate varying breast sizes, and provide faster screening through an adaptable breast coil utilizing stretchable elements.
Approach: A 20-channel breast coil was created with stretchable elements to accommodate varying bust sizes. Bench and phantom scans comparisons were made against an industry-standard flexible coil.
Results: Compared to industry-standard, highly-flexible coils, this coil demonstrated better adaptability to larger breasts, with improved sensitivity along the breast contour, and better acceleration.
Impact: Compared to the use of a traditional flexible coil of similar channel count for supine breast imaging, this coil can adapt to a wider range of breast sizes with easier setup, enhanced patient comfort, and performs better at greater acceleration.
Introduction
While efforts have been made to increase the comfort of prone breast MR scans, conventional coil setups are rigid, uncomfortable, and do not fit larger bust sizes. There is also the challenge of surgical planning due to lesion localization shifts when moving from the prone to supine position1-3. With the newly updated ACR guidelines, and predicted increase in MR surveillance of high-risk women, there is a need for a coil that is adaptable to all patient sizes, easy to setup, and is overall more comfortable. Supine approaches to breast coils have been made, but they do not inherently stretch to adapt to varying patient sizes4,5.Methods
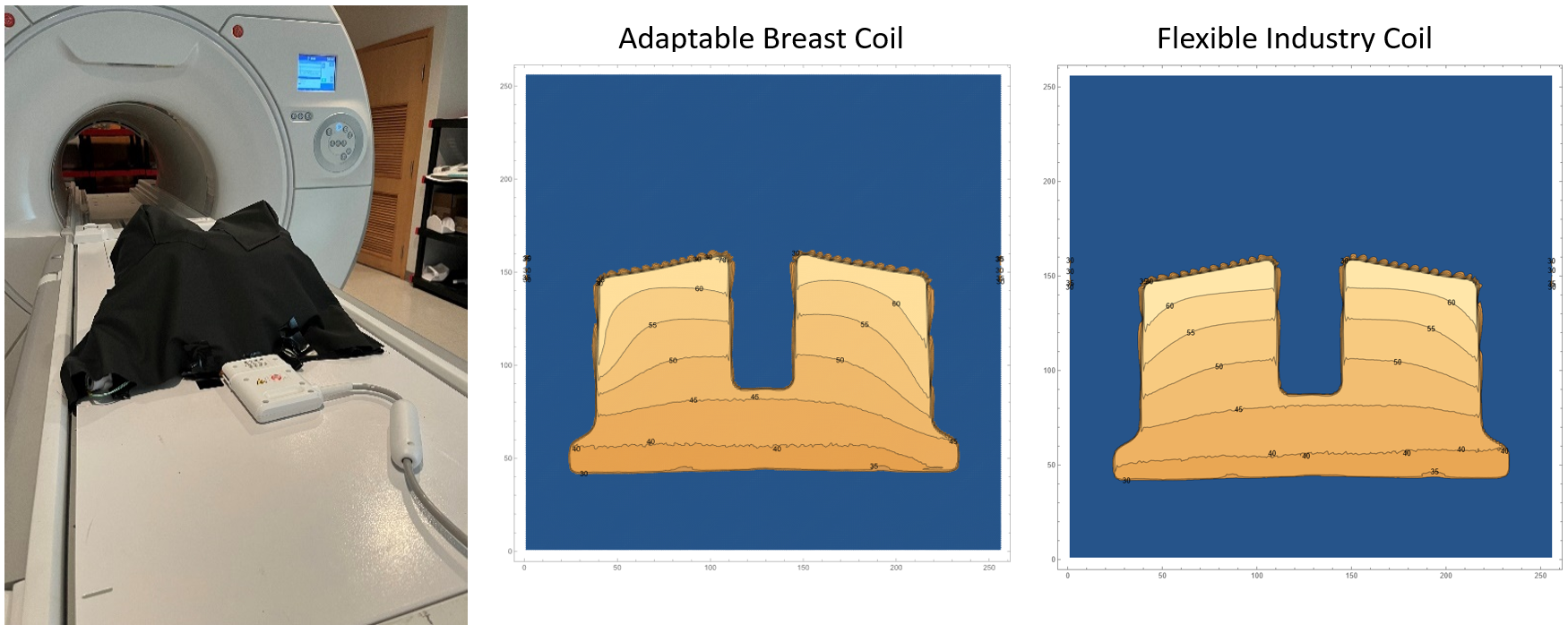
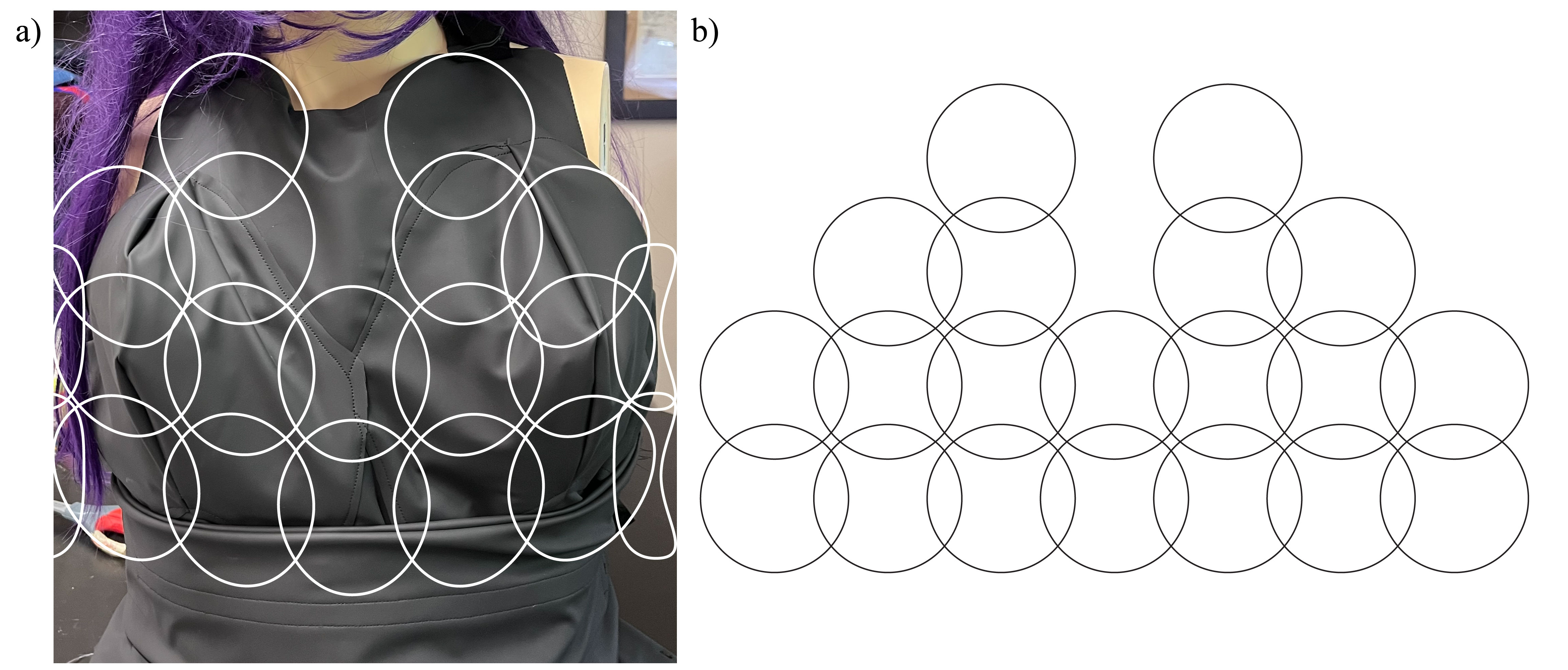
A 20-channel, bilateral, supine breast array was developed using 9-cm diameter elements stitched into fabric allowing for a 30% stretch resulting in a final achievable element diameter of 11.7 cm. The conductor chosen was Lyofil-332 (Syscom Advanced Materials Inc., Columbus, OH, USA). The electronics module includes a preamplifier, active and passive decoupling, matching/tuning circuitry, and baluns. Coil preamplifier decoupling is controlled using custom E-mode preamplifier. The final coil assembly was designed to accommodate a bust size up to 40F with tailored contours to minimize compression of the tissue against the chest while providing coverage of the axilla, breast, and supraclavicular lymph nodes (Fig.1). The coil is comprised of a stretchable coil layer, insulating material, and stretchable biocompatible sleeve. Bench S21 measurements were performed to determine the unloaded/loaded Q-ratio for this stretchable loop compared to a standard wire loop from a comparable industry-standard flexible coil. Both coil SNRs were calculated from a silicone oil breast biopsy phantom signal scan using a 3T scanner (SIGNA Premier, GE HealthCare, Waukesha, WI, USA) and by obtaining pure noise scans. The data was analyzed using a custom Wolfram Mathematica script (Wolfram Research, Champaign, IL, USA) to generate G-factor and sensitivity maps.Results
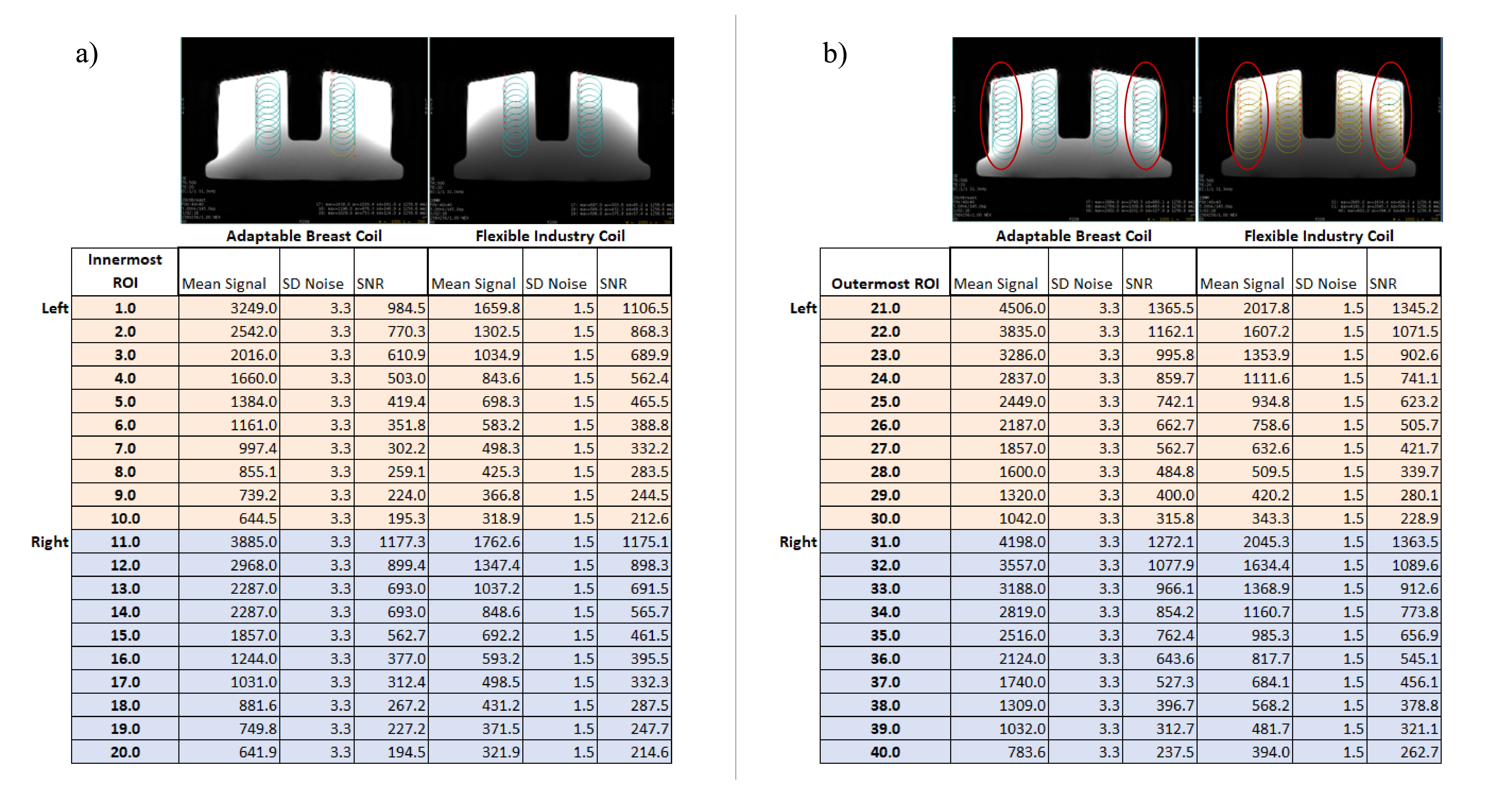
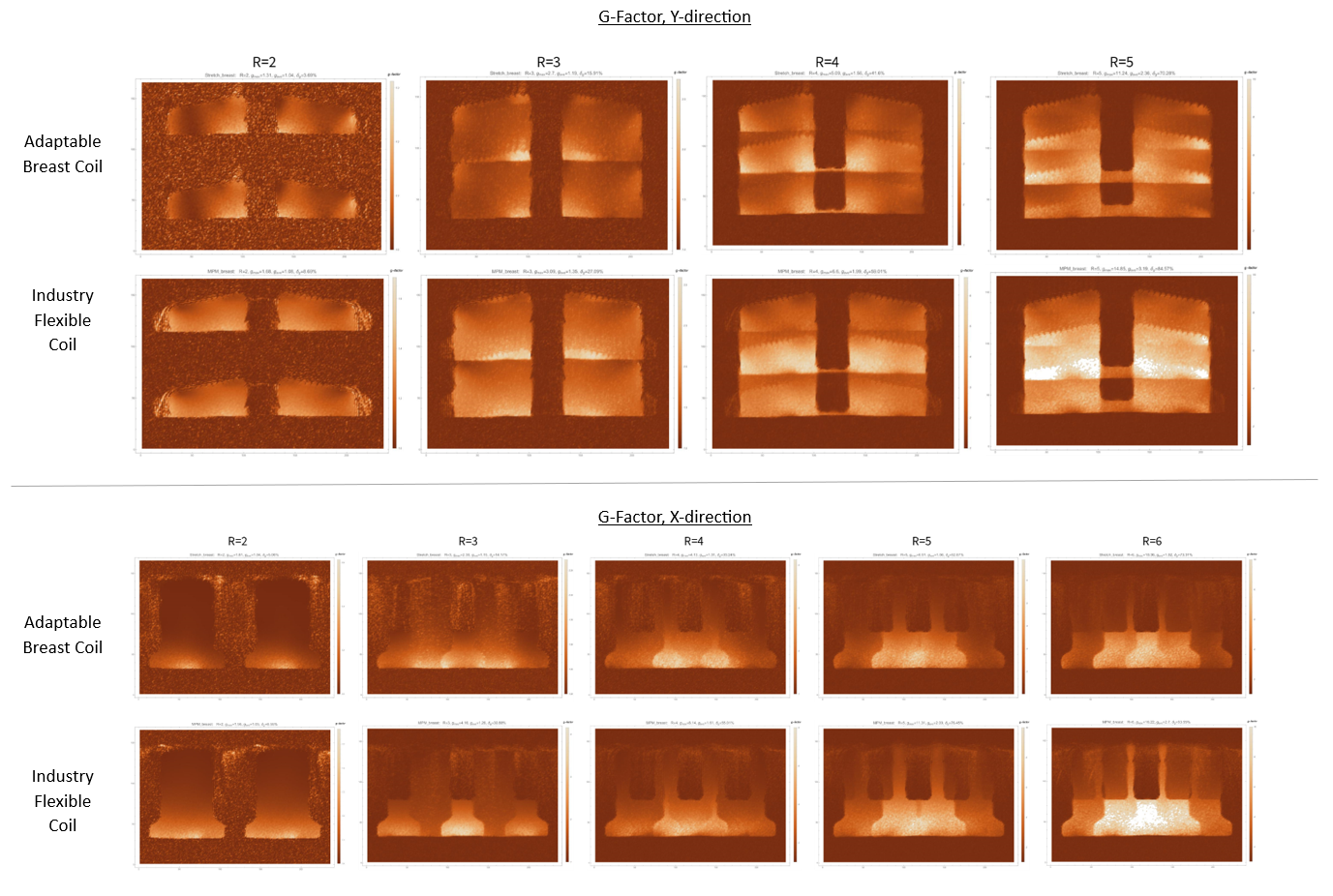
Compared to the flexible industry coil of the same channel count, the adaptable breast coil demonstrated that, despite the lower Qratio of 2.32 (compared to 6.14 for the industry coil loop) and higher conductor resistance, the closer contour of the coil resulted in only an 11% reduction in SNR at the phantom surface on the innermost ROIs along the coil's central line for the left half of a coil and similar performance in SNR on the right half of the coil (Fig. 3). In the outermost ROIs corresponding to the axilla region of the phantom, it was seen that, overall, the adaptable coil exhibited an SNR improvement at greater depths (Fig. 2-3). This improvement ranged from 1% to 43% depending on the area. Sensitivity maps of the adaptable coil show greater areas of sensitivity following the breast shape than the industry coil (Fig. 4). G-factor acceleration maps for both the X- and Y-direction show that less loss is seen in higher acceleration values for the adaptable coil than the industry coil (Fig. 5); With both coils, greater loss is seen at phantom depths that could correspond to the chest wall.Discussion
Due to the closer proximity of placement of this adaptable breast coil compared to an industry-standard flexible coil, the resistance limitation of the conductor and subsequent lower Q-ratio were able to be overcome with, at most, an 11.5% decrease in SNR at certain ROIs, but with improvement in SNR as depths increased along the outermost contoured edges of the phantom. The stretchable nature of the coil elements and sleeve allowed for greater adjustability and ability to position the coil compared to a conventional, rigid prone coil. G-factor maps show that acceleration can be used to reduce scan times and yield less loss in the images when compared to the industry flexible coil.Conclusion
Because of the vest-like wearable nature of the adaptable breast coil, setup time is drastically reduced, as the coil can be placed on the patient prior to entering the scan room. Additionally, supine scanning alleviates the pressure points on the sternum and lower abdomen that are typically seen with prone coil setups. While human scan data was not acquired at the time of this abstract, phantom scanning demonstrated great adaptability to even the largest of bust sizes while maintaining SNR comparable to an industry-standard flexible coil of the same channel count. While biopsy in the supine position poses a challenge, a dedicated, high-channel breast coil could greatly impact routine MR screenings through expediated scan times and patient setup along with increased patient compliance. Continuing research includes expanding the coil to higher channel counts, improving the mechanical stability of elements, and acquisition of human scan data.Acknowledgements
The authors would like to thank Barbara Sammut, Jonielle McDonnough, Adrienne Guyton, Anna Jorgensen, Jihad Elallami, Chaimaa Maghfour, and Brandon Wang for their efforts on this project.References
1. Carbonaro LA, Tannaphai P, Trimboli RM, et al. Contrast enhanced breast MRI: spatial displacement from prone to supine patient’s position. Preliminary results. Eur J Radiol. 2012; 81:e771–e774. doi: 10.1016/j.ejrad.2012.02.013.
2. Satake H, Ishigaki S, Kitano M, et al. Prediction of prone-to-supine tumor displacement in the breast using patient position change: investigation with prone MRI and supine CT. Breast Cancer. 2016;23:149–158. doi: 10.1007/s12282-014-0545-z.
3. Arıbal E, Buğdaycı O. Supplementary abbreviated supine breast MRI following a standard prone breast MRI with single contrast administration: is it effective in detecting the initial contrast-enhancing lesions?. Diagn Interv Radiol. 2019;25(4):265-269. doi:10.5152/dir.2019.18167
4. Vincent J, Follante CK, Bayram E, et al., “Ultra-Flexible, High-Resolution, 60-Channel RF Coil for Supine Breast Imaging,” in Proc. Intl. Soc. Mag. Reson. Med. 29, 2021, #1591, [Online]. Available: https://cds.ismrm.org/protected/21MProceedings/PDFfiles/1591.html
5. Nohava L, Obermann M, Frass-Kriegl R, et al., “BraCoil – preliminary performance evaluation of a wearable breast coil array for 3 T MR mammography,” in Proc. Intl. Soc. Mag. Reason. Med. 30, 2022, #2253, [Online]. Available: https://cds.ismrm.org/protected/22MProceedings/PDFfiles/2253.html
Figures
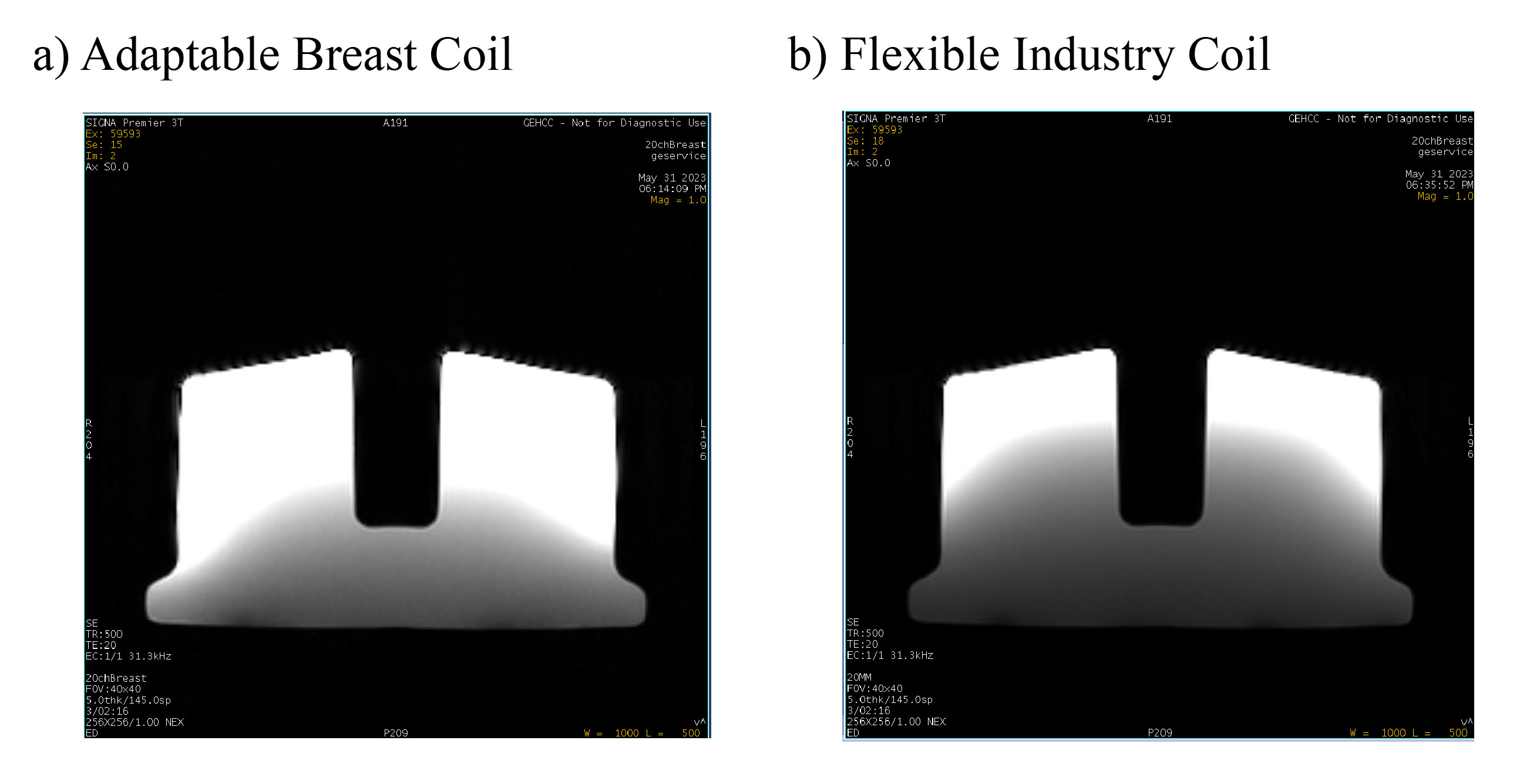
a) Image showing the resulting phantom images from the 20-channel adaptable breast coil, b) Image showing the resulting phantom image from the 20-channel flexible industry coil. Window leveling has been kept consistent for comparison.