1405
Evaluation of Metal-Artifact Reduction Techniques at 7T: Hardware adaption, phantom study, and preliminary in vivo results1Erwin L. Hahn Institute for MRI, University Duisburg-Essen, Essen, Germany, 2Westphalian University of Applied Sciences, Gelsenkirchen, Germany, 3High-Field and Hybrid MR Imaging, University Hospital Essen, Essen, Germany, 4General Psychology: Cognition and Center for Behavioral Addiction Research (CeBAR), University Duisburg-Essen, Duisburg, Germany, 5Department of Diagnostic and Interventional Radiology and Neuroradiology, University Hospital Essen, Essen, Germany
Synopsis
Keywords: High-Field MRI, High-Field MRI, artifacts, MSK
Motivation: Advanced metal-artifact reduction sequences (MARS) are currently only available in parallel transmission (pTx) research mode at 7T, while clinically approved RF coils are single-channel transmit (sTx) coils.
Goal(s): Our goal was to build an adapter to connect a sTx knee coil to a pTx system, and to evaluate MARS techniques in phantom and in vivo scans.
Approach: An evaluation of artifact reduction using advanced MARS techniques was performed in a phantom study. Knees of three volunteers with metallic suture plates were imaged.
Results: Optimized bandwidth and view-angle-tilting (VAT) effectively reduced metal artifacts while keeping acquisition time and SAR load acceptable.
Impact: A hardware adaption for connecting a sTx coil to a pTx system was evaluated for safe in vivo usage. The application of MARS was demonstrated for the first time at 7T in volunteers with metallic suture plates after ACL reconstruction.
INTRODUCTION
The presence of small metallic implants within the direct field-of-view in ultrahigh-field (UHF) examinations as well as their impact on image quality have recently been presented for brain 1 and knee 2 scans. The severity of metal-induced artifacts depends on the properties of the implant, choice of pulse sequences and their parameters, but also on the main magnetic field strength. Germann et al. 3 have recently investigated advanced metal-artifact reduction sequences (MARS) at UHF in a phantom study. Advanced MARS techniques like view-angle tilted (VAT) 4 and slice-encoding for metal artifact correction (SEMAC) 5 are well established for musculoskeletal (MSK) MR imaging, but they are only available in parallel transmit (pTx) research mode on a MAGNETOM Terra system (Siemens Healthineers, Germany). Hence, the authors 3 used an eight-channel transmit head coil as a workaround for imaging two MSK implants, i.e., a spinal pedicle screw and an intervertebral cage. In this study, we report on a hardware adaption to connect a single-channel transmit (sTx) knee coil to the pTx system, present a phantom study with a titanium suture button typically used in anterior cruciate ligament reconstructions (ACLR), and finally show preliminary in vivo images.METHODS
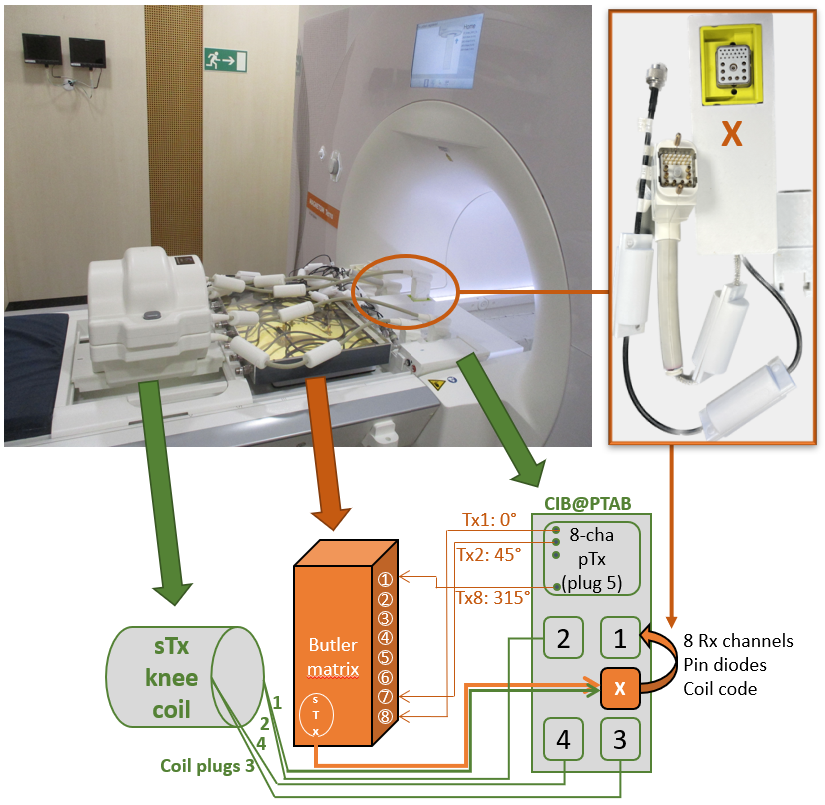
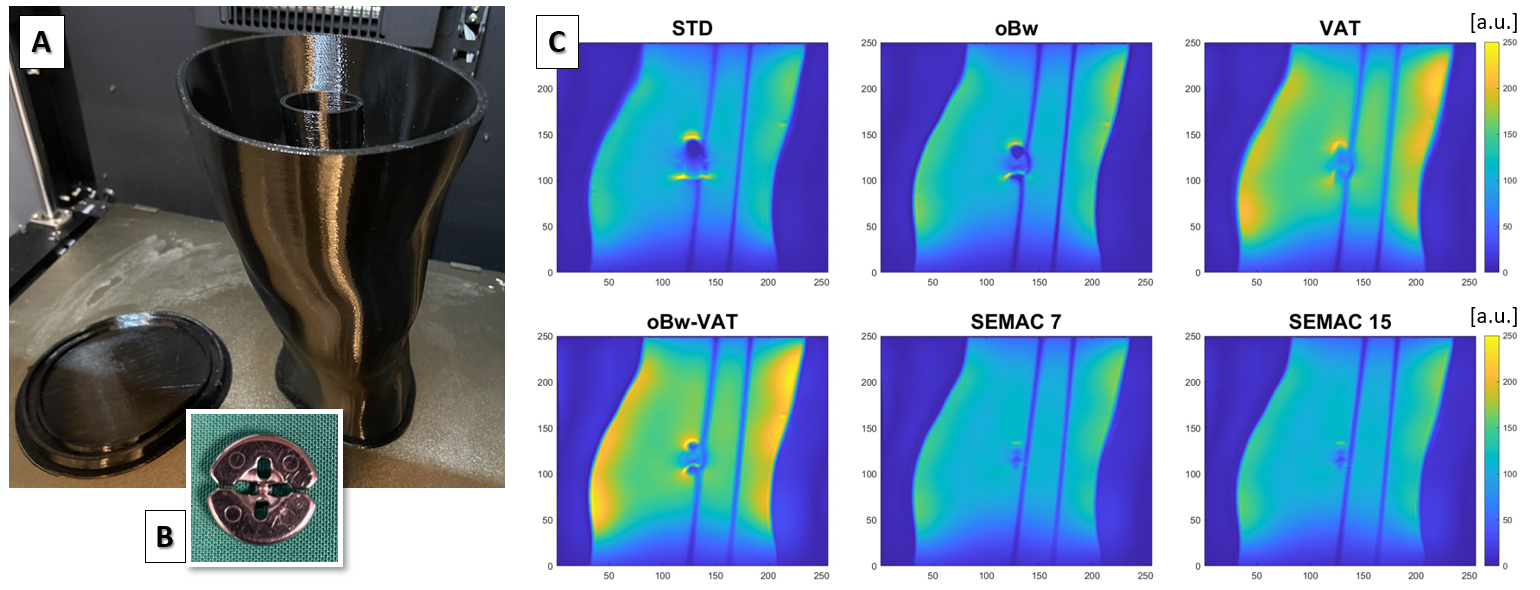
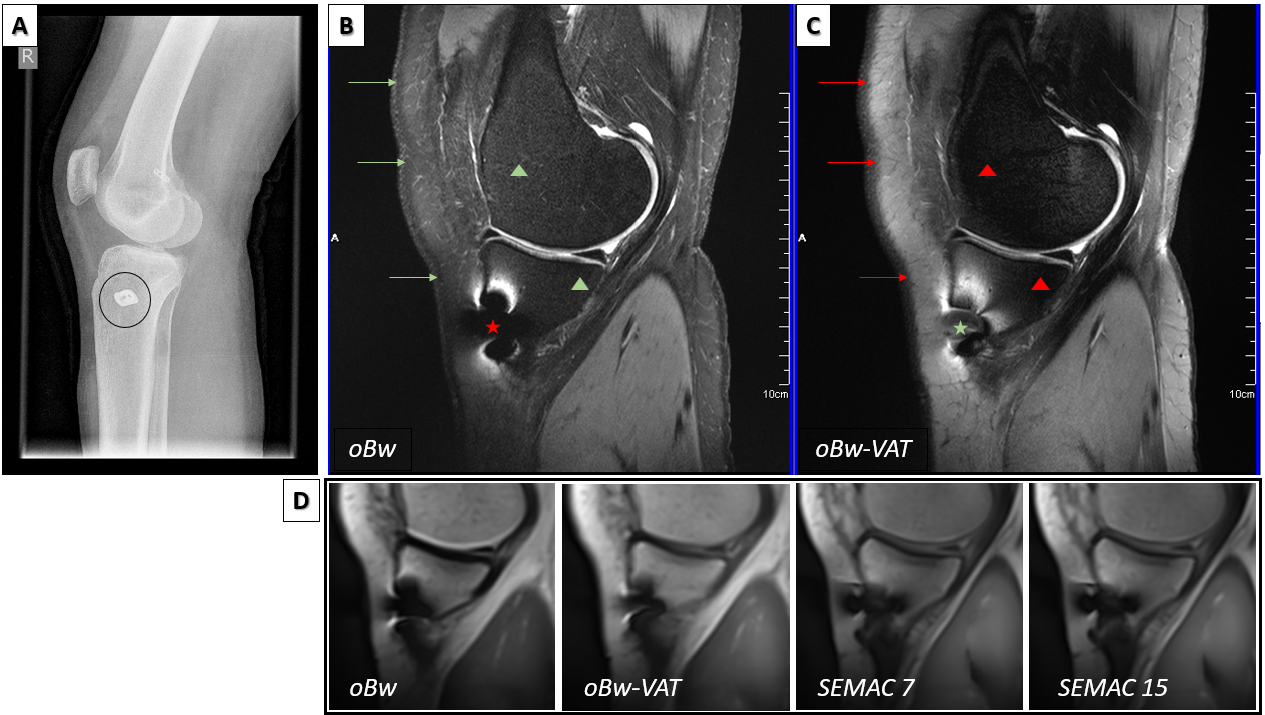
To connect the clinically approved sTx knee coil (Quality Electrodynamics, OH) to the pTx system an adapter was built, which combined the individual eight transmit channels to a sTx port and also fed one of the knee coil’s connectors via an additional plug to the MR system’s coil interface box (Fig. 1). A Butler matrix 6 was used as an 8:1 RF combiner in inversed direction. The setup was characterized on the bench and in comparative MR measurements in both Tx modes using the 3DREAM flip angle (FA) mapping 7 and the coil_utils service sequence (SNR, g-factor, noise correlation). Two anatomically shaped knee phantoms with simplified inner bone structure were built. One phantom served as reference, while in the other phantom a titanium suture button was placed inside (Fig. 2). Vegetable oil was used as filling material to prevent additional B1+ artifacts. MARS techniques as presented in Ref. 3 (optimized bandwidth (oBw), VAT, SEMAC) were applied to turbo spin echo (TSE) sequences. The setup was cleared by our institutional MR safety board for in vivo usage. Three subjects who underwent ACLR in their past were imaged after obtaining informed consent. Images were qualitatively evaluated by a radiologist with respect to the degree of artifact reduction from the individual MARS techniques, potential diagnostic impairment by remaining artifacts adjacent to the implant, and overall image quality.RESULTS
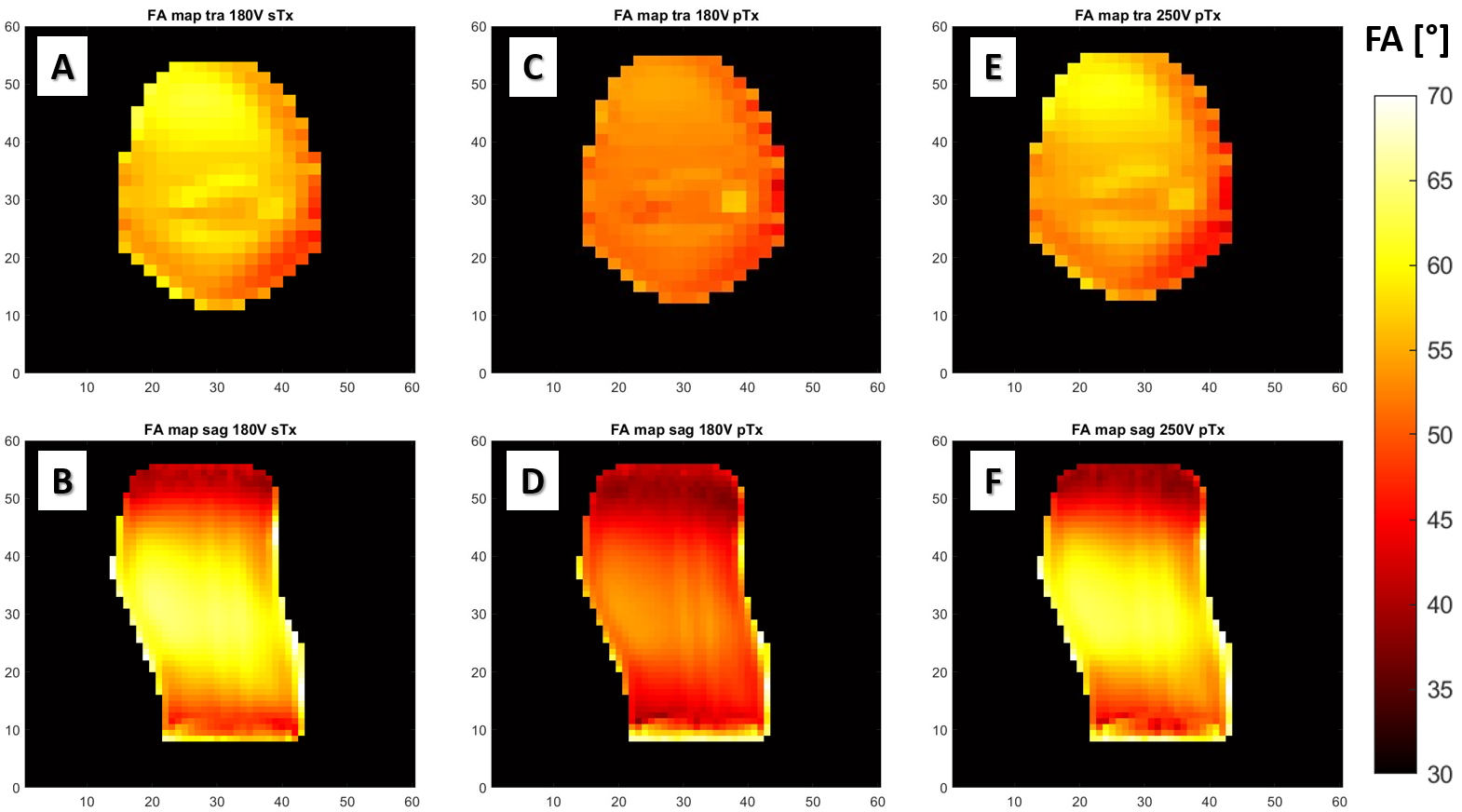
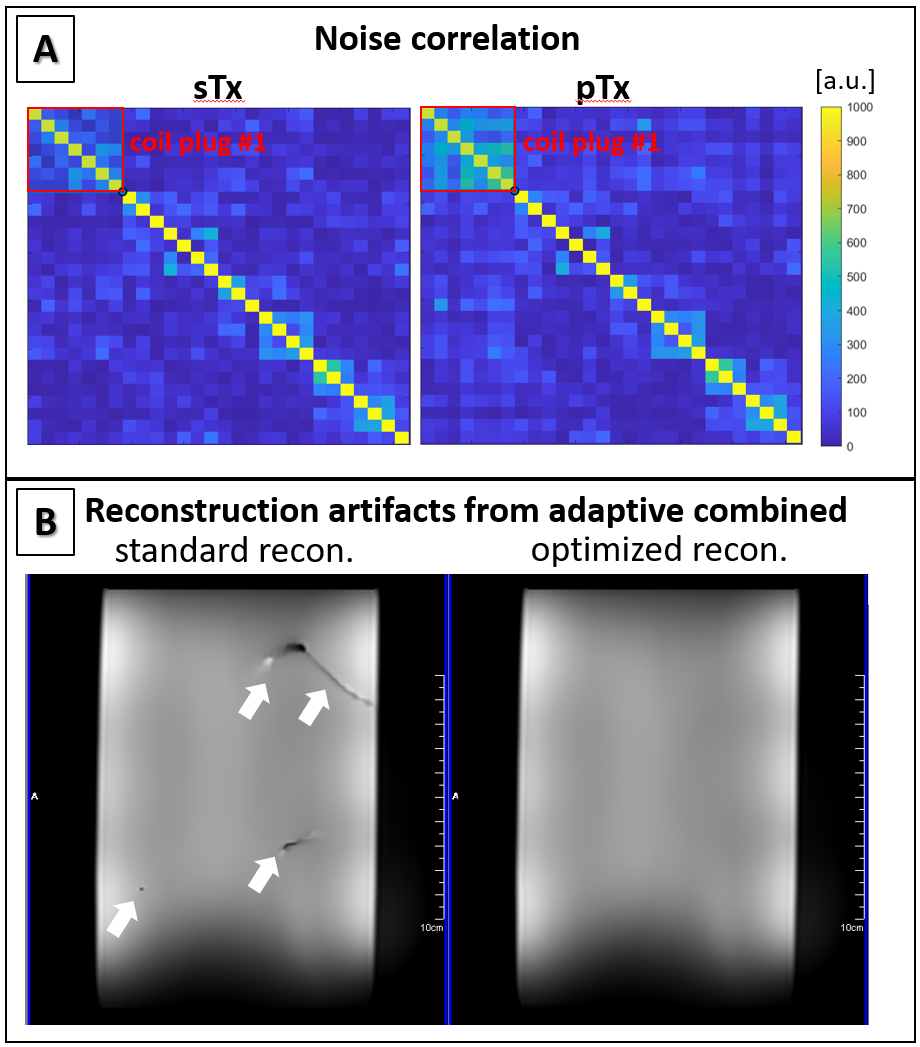
Measurements on the bench showed a mean S11 of -10.6dB at the input ports of the Butler matrix which corresponded well with a detected reflection at the eight Tx ports of 13% at the MR system. Due to additional attenuation losses of the complete Tx chain (25%), the transmitter reference amplitude needed to be increased by 40% from sTx to pTx mode as shown in the comparative FA mapping (Fig. 3). Overall, FA and SNR distribution as well as g-factor analysis remained unchanged. Due to the feed through of eight receive channels from coil plug 1 an increase in noise correlation of 50% between those channels was observed (Fig. 4). Interestingly, this caused severe reconstruction artifacts only in the SEMAC scans which were sensitive to phase errors (Fig. 4) in the adaptive combined reconstruction 8. However, an adaptive combined reconstruction using eigen value decomposition with phase correction prevented these artifacts. A combination of oBw and VAT reduced metal artifacts by 25% compared to standard imaging (Fig. 2). SEMAC yielded best results with respect to minimum peri-implant signal voids (43% reduction) and distortion at cost of nearly 6-fold increased acquisition time and SAR load. An increase of the slice encoding steps in SEMAC from 7 to 15 did not improve geometric distortions further. The subjects were imaged without complications at 7T. Images were only minimally compromised by metal-induced artifacts within the direct vicinity of the implants. The oBw-VAT technique was found best in terms of efficiently reducing artifacts while keeping both scan time and SAR load reasonable. Additionally, high resolution fat suppressed PD-weighted TSE images were obtained to complement the results. Here, VAT was inferior due to insufficient fat suppression (Fig. 5).DISCUSSION & CONCLUSION
A setup for connecting a sTx coil to the pTx system was presented. The use of advanced MARS techniques at UHF was demonstrated for the first time in vivo in subjects after ACL graft reconstruction. Future studies will determine whether 7T MARS MRI offers diagnostic benefit over lower field strengths.Acknowledgements
The MAGNETOM Terra used in this study was funded by the German Research Foundation (DFG) – project number 432657511.References
1. Chen B, Schoemberg T, Kraff O, et al. Cranial fixation plates in cerebral magnetic resonance imaging: a 3 and 7 Tesla in vivo image quality study. Magma Magn Reson Mater Phy. June 2016;29(3):389-98.
2. Kraff O, Theysohn JM, Theisejans J, Quick HH. 7T MRI of the knee joint after anterior cruciate ligament graft reconstruction: safety discussion and image quality study. Proceedings ISMRM 2023: #611.
3. Germann C, Falkowski AL, von Deuster C, Nanz D, Sutter R. Basic and Advanced Metal-Artifact Reduction Techniques at Ultra-High Field 7-T Magnetic Resonance Imaging-Phantom Study Investigating Feasibility and Efficacy. Invest Radiol. June 2022;57(6):387-398.
4. Cho ZH, Kim DJ, Kim YK. Total inhomogeneity correction including chemical shifts and susceptibility by view angle tilting. Med Phys. Jan-Feb 1988;15(1):7-11.
5. Lu W, Pauly KB, Gold GE, Pauly JM, Hargreaves BA. SEMAC: Slice Encoding for Metal Artifact Correction in MRI. Magn Reson Med. Jul 2009;62(1):66-76.
6. Yazdanbakhsh P, Solbach K. Microstrip Butler matrix design and realization for 7 T MRI. Magn Reson Med. Jul 2011;66(1):270-80.
7. Ehses P, Brenner D, Stirnberg R, Pracht ED, Stocker T. Whole-brain B1 -mapping using three-dimensional DREAM. Magn Reson Med. Sep 2019;82(3):924-934.
8. Walsh DO, Gmitro AF, Marcellin MW. Adaptive reconstruction of phased array MR imagery. Magn Reson Med. May 2000;43(5):682-90.
Figures