1389
CMR Imaging-Based Risk Stratification for Patients with Dilated Cardiomyopathy and Severe Left Ventricular Dysfunction1Fuwai Hospital, Peking Union Medical College, Chinese Academy of Medical Sciences, Beijing, China, 2Fuwai Hospital, Beijing, China
Synopsis
Keywords: Myocardium, Cardiomyopathy
Motivation: Dilated cardiomyopathy (DCM) patients with severely reduced left ventricular ejection fraction of≤35% face a high risk of sudden cardiac death and heart failure events.
Goal(s): We aimed to refine a risk stratification model based on cardiac magnetic resonance imaging for DCM patients with LVEF≤35%, and to enhance clinical decision-making and ultimately, patient outcomes.
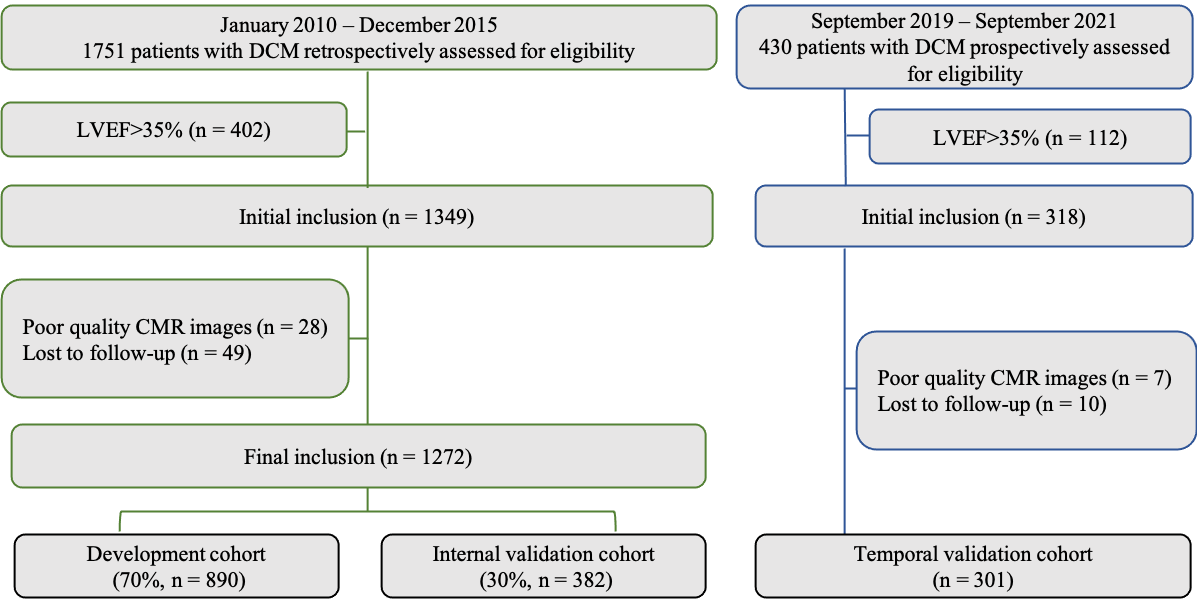
Approach: A retrospective analysis was conducted on 1272 DCM patients divided into a development cohort and an internal validation cohort, as well as a prospective validation cohort (n=301).
Results: Both LGE and LAVi are independently risk factors for predicting survival in a large cohort of patients with DCM and LVEF≤35%.
Impact: Our novel risk stratification may assist in timely interventions such as implantation of implantable cardioverter-defibrillator, heart transplantation, implementation of left ventricular assist devices, or referral for HF specialty care, ultimately leading to improved outcomes for DCM patients with LVEF≤35%.
Introduction
Dilated cardiomyopathy (DCM) patients with severely reduced left ventricular ejection fraction (LVEF) of ≤ 35% face a high risk of sudden cardiac death (SCD) and heart failure (HF) events. We aimed to refine a risk stratification model based on cardiac magnetic resonance imaging for DCM patients with LVEF ≤ 35%, and to enhance clinical decision-making and ultimately, patient outcomes.Methods
A retrospective analysis was conducted on 1272 DCM patients with LVEF ≤ 35%, divided into a development cohort (70%) and an internal validation cohort (30%). The risk models were validated in a prospective temporal validation cohort (n = 301). The arrhythmic endpoint was defined as a composite of sudden cardiac death (SCD) or aborted SCD, while the HF endpoint was a composite of HF death or heart transplantation.Results
Over a median follow-up of 87.4 months, 104 patients reached the arrhythmic endpoints, and 131 patients reached the HF endpoints. Patients with late gadolinium enhancement (LGE) ≥ 7.5% had a hazard ratio (HR) of 3.6 (p <0.001) for the arrhythmic endpoint, while patients with left atrial volume index (LAVi) ≥ 75.6 ml/m2 had a HR of 2.1 (p <0.001) for the HF endpoint. Finally, we constructed a CMR-based risk stratification model for predicting both SCD/aborted SCD and HF death/HTx risks by combining LVEF, LGE, and LAVi. High-risk SCD patients with LVEF < 20% and LGE ≥ 7.5% had a 9.29-fold higher risk of arrhythmic events compared to low-risk SCD patients with LVEF 20-35% and LGE negative. Patients with LVEF < 20% and LAVi ≥ 75.6ml/m2 had the highest risk of HF endpoint (annual event rate: 4.7%, p <0.001).Discussion
The present study is one of the largest cohorts of patients with severely reduced LVEF in DCM, focusing on survival risk stratification using cardiac magnetic resonance metrics, and employing a long-term follow-up. Our key findings are as follows. First, we found that a 3.6-fold increased risk of SCD composite events in patients with LGE ≥ 7.5% , while patients with LAVi ≥ 75.6 ml/m2 exhibited a 2.1-fold increased risk of HF death or HTx. Second, we established risk categories for predicting the probability of SCD composite events using LVEF and LGE percentage of LV mass, and for forecasting the probability of HF death/HTx events with LAVi and LVEF over years. Based on these risk categories, we described and validated a novel quantitatively prognostic tool for patients with DCM and LVEF ≤ 35%, integrating both clinical and CMR metrics. Third, to the best of our knowledge, our study initially built a “one-stop” risk algorithm encompassing SCD and competing non-SCD events for the DCM population with LVEF ≤ 35%. Specifically, patients with DCM, LVEF < 20% and LGE ≥ 7.5% were at heightened risk of SCD composite events, suggesting a potential benefit from prompt ICD implantation. Conversely, LGE-negative patients with LVEF ranging from 20% to 35% displayed a genuinely low predictive likelihood of SCD/aborted SCD, indicating that ICD implantation for primary prevention might not be necessary. For patients with LVEF < 20%, LGE < 7.5%, and LAVi ≥ 75.6 ml/m2, physicians should prioritize addressing worsening heart failure, as the escalation in the risk of HF death/ HTx surpasses that of SCD or aborted SCD.Conclusion
Both LGE and LAVi are independently risk factors for predicting survival in a large cohort of patients with DCM and LVEF ≤ 35%. Our novel risk stratification may assist in timely interventions such as implantation of implantable cardioverter-defibrillator, heart transplantation, implementation of left ventricular assist devices, or referral for HF specialty care, ultimately leading to improved outcomes for DCM patients with LVEF ≤ 35%.Acknowledgements
None.References
1. Li S, Zhou D, Sirajuddin A, He J, Xu J, Zhuang B, et al. T1 Mapping and Extracellular Volume Fraction in Dilated Cardiomyopathy: A Prognosis Study. JACC Cardiovasc Imaging. 2022;15(4):578-590.
2. Halliday BP, Cleland JGF, Goldberger JJPrasad SK. Personalizing Risk Stratification for Sudden Death in Dilated Cardiomyopathy: The Past, Present, and Future. Circulation. 2017;136(2):215-231.
3. Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022;79(17):e263-e421.
4. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129-2200.
5. Køber L, Thune JJ, Nielsen JC, Haarbo J, Videbæk L, Korup E, et al. Defibrillator Implantation in Patients with Nonischemic Systolic Heart Failure. N Engl J Med. 2016;375(13):1221-30.
6. Pocock SJ, Ariti CA, McMurray JJ, Maggioni A, Køber L, Squire IB, et al. Predicting survival in heart failure: a risk score based on 39 372 patients from 30 studies. Eur Heart J. 2013;34(19):1404-13.
7. Barlera S, Tavazzi L, Franzosi MG, Marchioli R, Raimondi E, Masson S, et al. Predictors of mortality in 6975 patients with chronic heart failure in the Gruppo Italiano per lo Studio della Streptochinasi nell'Infarto Miocardico-Heart Failure trial: proposal for a nomogram. Circ Heart Fail. 2013;6(1):31-9.
8. Pocock SJ, Wang D, Pfeffer MA, Yusuf S, McMurray JJ, Swedberg KB, et al. Predictors of mortality and morbidity in patients with chronic heart failure. Eur Heart J. 2006;27(1):65-75.
9. Levy WC, Mozaffarian D, Linker DT, Sutradhar SC, Anker SD, Cropp AB, et al. The Seattle Heart Failure Model: prediction of survival in heart failure. Circulation. 2006;113(11):1424-33.
10. Arbelo E, Protonotarios A, Gimeno JR, Arbustini E, Barriales-Villa R, Basso C, et al. 2023 ESC Guidelines for the management of cardiomyopathies. Eur Heart J. 2023.
11. Di Marco A, Brown PF, Bradley J, Nucifora G, Claver E, de Frutos F, et al. Improved Risk Stratification for Ventricular Arrhythmias and Sudden Death in Patients With Nonischemic Dilated Cardiomyopathy. J Am Coll Cardiol. 2021;77(23):2890-2905.
12. Li S, Wang Y, Yang W, Zhou D, Zhuang B, Xu J, et al. Cardiac MRI Risk Stratification for Dilated Cardiomyopathy with Left Ventricular Ejection Fraction of 35% or Higher. Radiology. 2022:213059.
13. Gulati A, Ismail TF, Jabbour A, Ismail NA, Morarji K, Ali A, et al. Clinical utility and prognostic value of left atrial volume assessment by cardiovascular magnetic resonance in non-ischaemic dilated cardiomyopathy. Eur J Heart Fail. 2013;15(6):660-70.
14. Pinto YM, Elliott PM, Arbustini E, Adler Y, Anastasakis A, Bohm M, et al. Proposal for a revised definition of dilated cardiomyopathy, hypokinetic non-dilated cardiomyopathy, and its implications for clinical practice: a position statement of the ESC working group on myocardial and pericardial diseases. Eur Heart J. 2016;37(23):1850-8.
15. Zhuang B, Li S, Xu J, Zhou D, Yin G, Zhao S, et al. Age- and Sex-Specific Reference Values for Atrial and Ventricular Structures in the Validated Normal Chinese Population: A Comprehensive Measurement by Cardiac MRI. J Magn Reson Imaging. 2020;52(4):1031-1043.
Figures
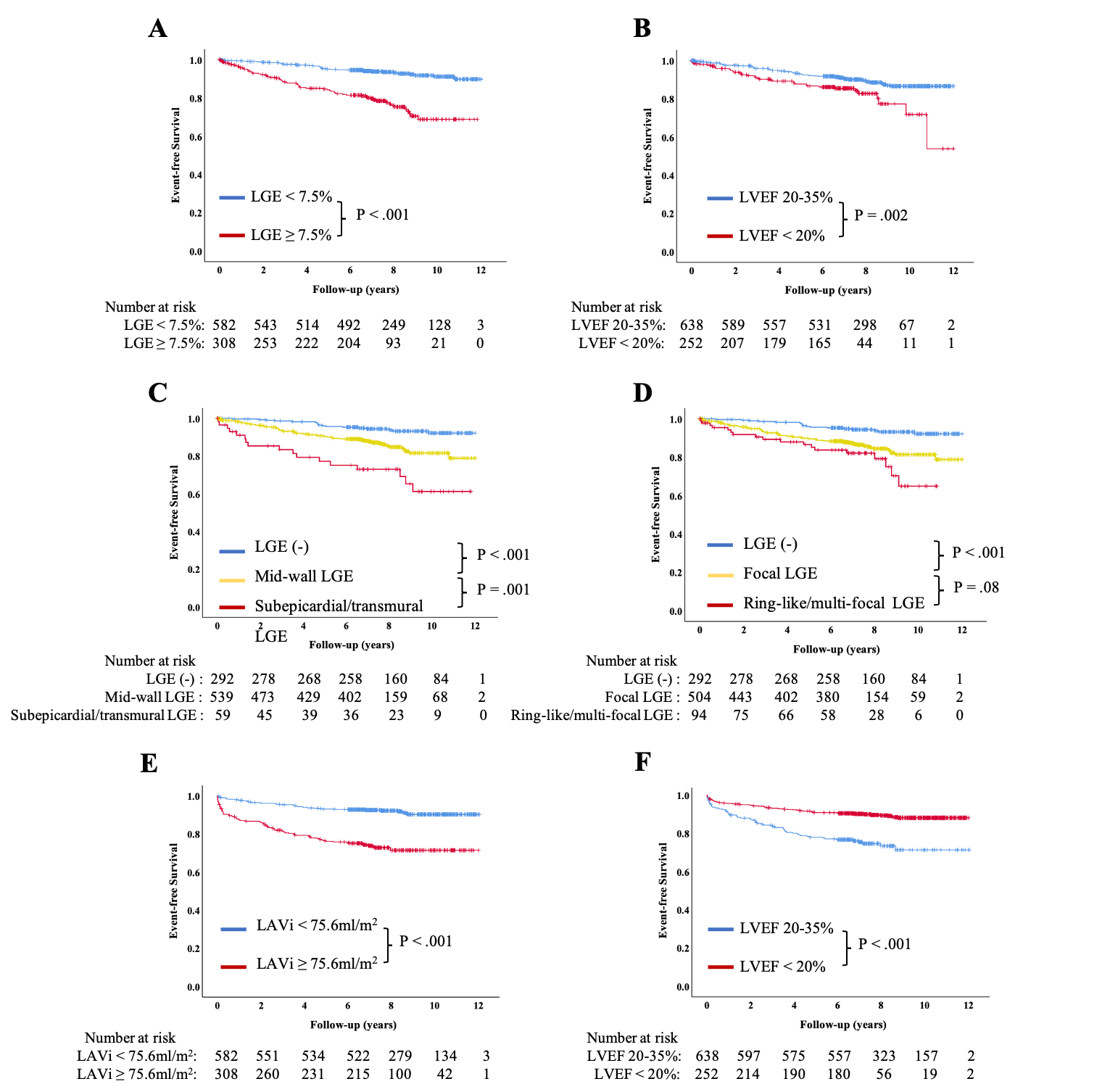
Kaplan-Meier curves for CMR parameters and outcomes in patients with DCM and LVEF≤35%.
Kaplan-Meier curves for LGE (A), LVEF (B), LGE distribution (C), LGE pattern (D) and arrhythmic endpoint, LAVi (E), LVEF (F) and HF endpoint.
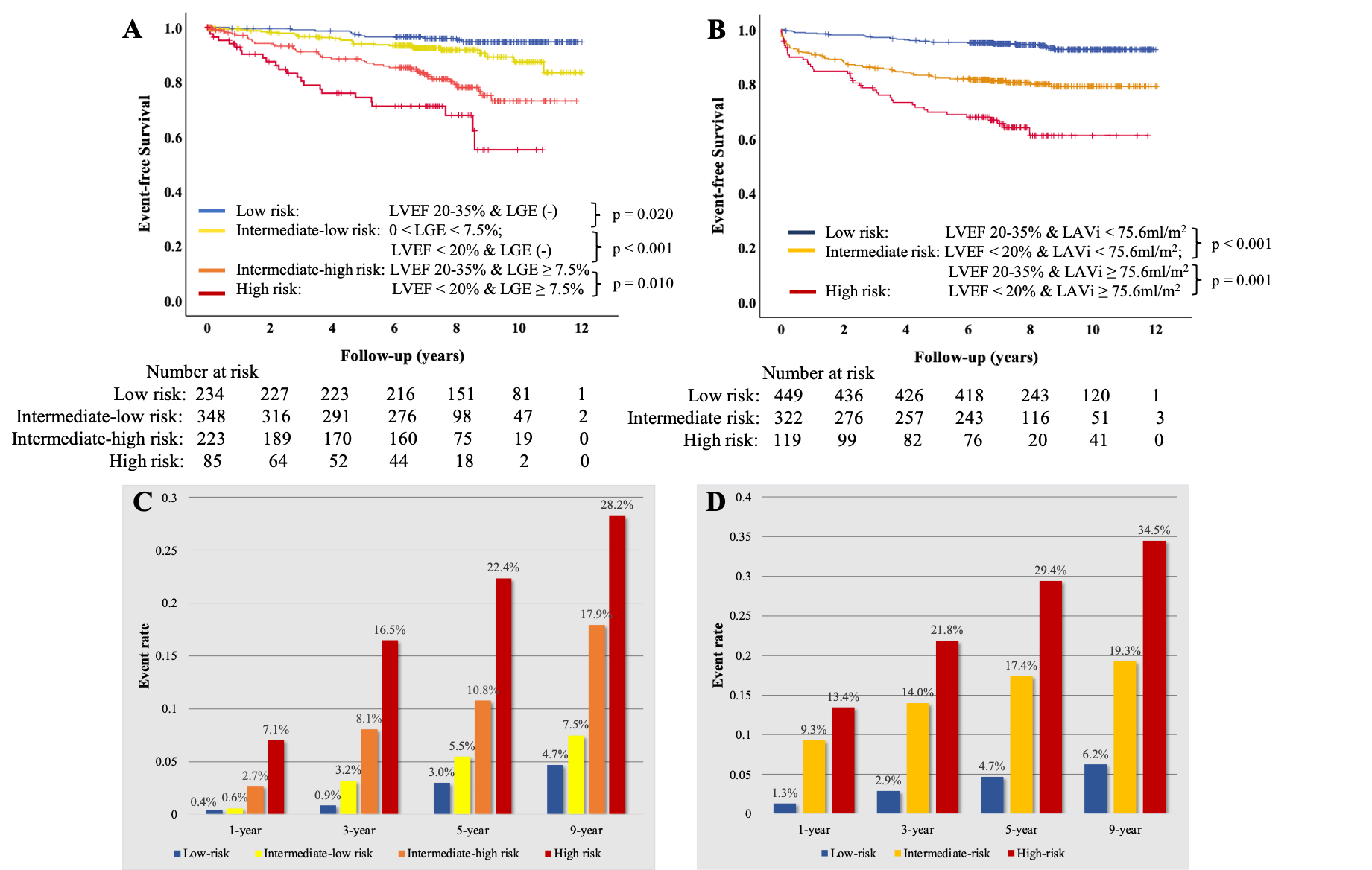
Clinical risk stratifications of the arrhythmic and HF endpoint.
Kaplan-Meier curves illustrated survival free from the arrhythmic (A) and HF (B) endpoint. Bar graphs showed cumulative event rate of arrhythmic endpoint (C) and HF endpoint (D) for all categories risk stratified.
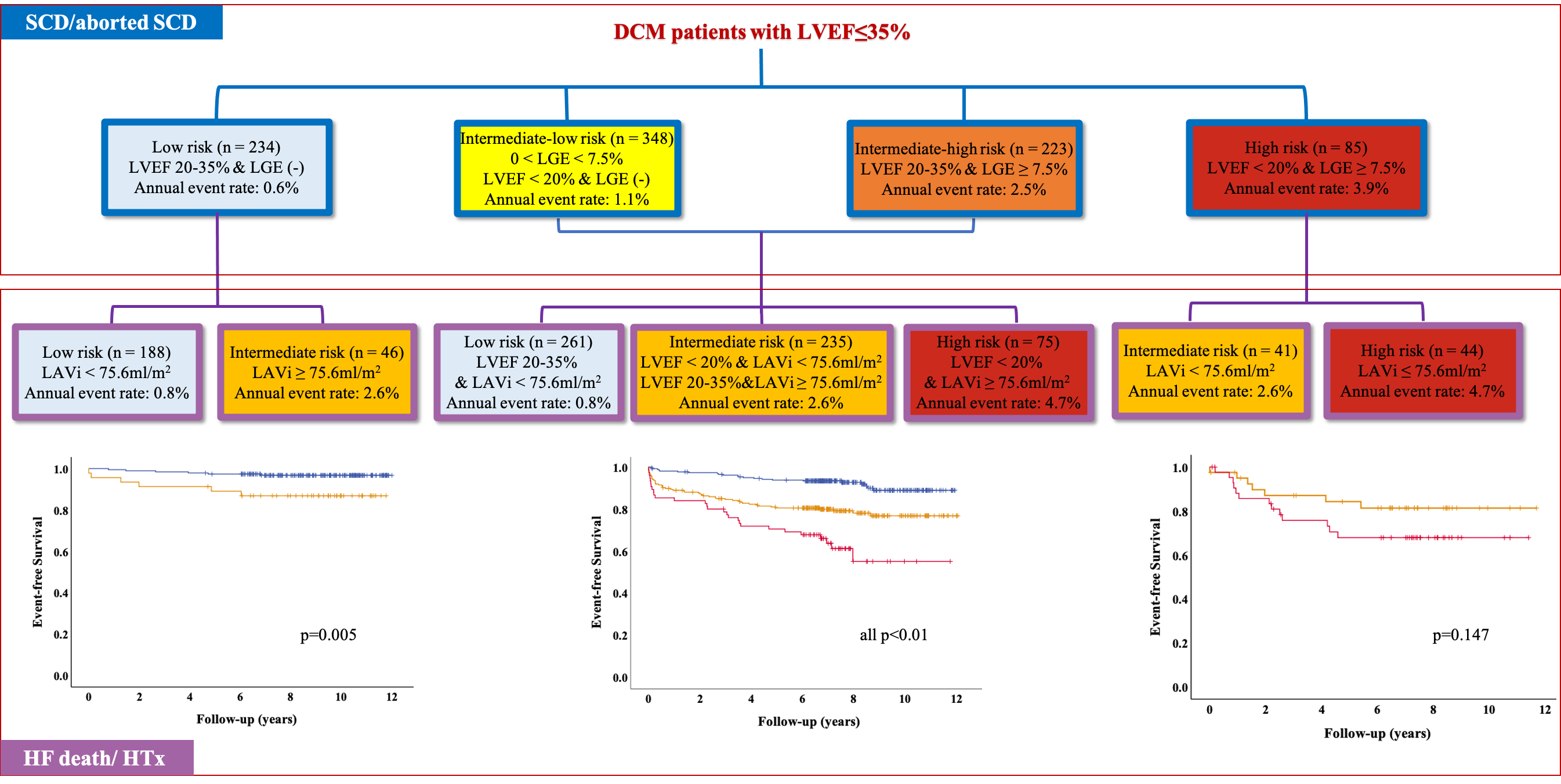
Clinical risk stratification for decision making combined with LVEF, LGE and LAVi.
Flow chart summarized the categories of the SCD compositing events and HT death/HTx risk.