1387
Prognostic value of dark right ventricular blood pool sign on myocardial T2 mapping in patients with dilated cardiomyopathy1Radiology, Xiangya Hospital Central South University, Changsha, China, 2Radiology, Xiangya Hospital, Central South University, Changsha, China, 3Radiology, Yiyang Central Hospital, Yiyang, China, 4Scientific Marketing, Siemens Healthineers Ltd, Wuhan, China, 5MR Collabration, Siemens Healthineers, Los Angeles, CA, United States
Synopsis
Keywords: Heart Failure, Cardiovascular
Motivation: The evaluation of surrogate markers of cardiopulmonary status may provide risk stratification and prognostication in patients with dilated cardiomyopathy.
Goal(s): To investigate the prognostic value of the dark right ventricular blood pool (RVBP) sign on T2 mapping by CMR.
Approach: T2 mapping was used to measure T2 values of septum, RV and LV blood pool images in DCM patients and healthy controls.All patients were followed to record major adverse cardiac events (MACEs).
Results: The sign of dark-RVBP on T2 mapping was found in 31.3% (42/134) of DCM patients. The ratio of T2RV/T2LV seemed to be an independent predictor for MACEs in DCM patients.
Impact: The sign of dark-RVBP on T2 mapping by CMR was associated with hard clinical events with prognostic information independent of and incremental to myocardial strain parameters.
INTRODUCTION
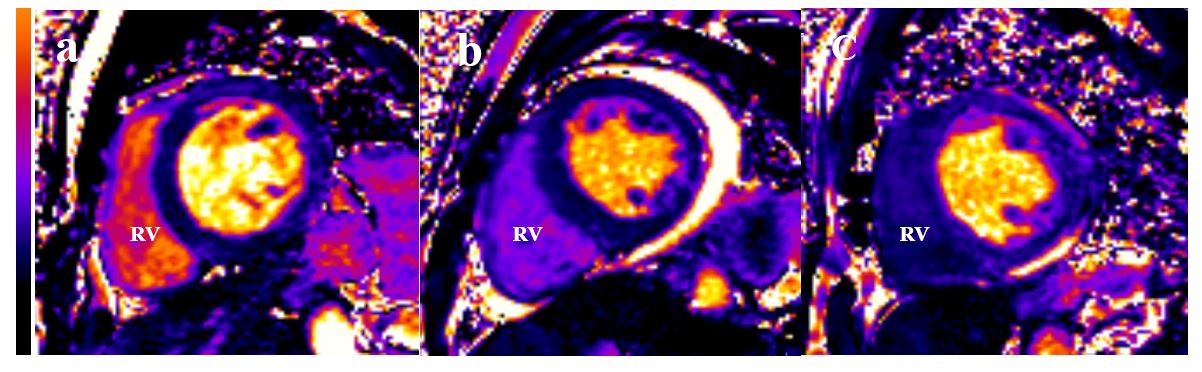
DCM is the most common form of primary cardiomyopathy and represents a significant cause of morbidity and mortality. The T2 mapping can not only be used to quantify myocardial inflammation and edema [1], but it is also sensitive to blood oxygenation levels [2]. In the clinical practice, we noted that the dark right ventricular blood pool (RVBP) on the T2 mapping in some DCM patients. However, T2 mapping data on septum and blood pool of DCM as well as in the follow-up are lacking so far. Moreover, the value of T2 for prediction of MACE of DCM remains unclear.METHODS
Population: DCM patients (n = 134) and healthy controls (HC; n = 28). Field Strength/Sequence: 3.0T MRI balanced steady state free precession (bSSFP) sequence (cine imaging), T2-prepared bSSFP sequence (T2 mapping). Assessment: Ejection fraction (EF) and ventricular strain parameters of LV and RV were derived using cine images. T2 mapping was used to measure T2 values of septum, RV and LV blood pool. All patients were followed to record major adverse cardiac events (MACEs).RESULTS
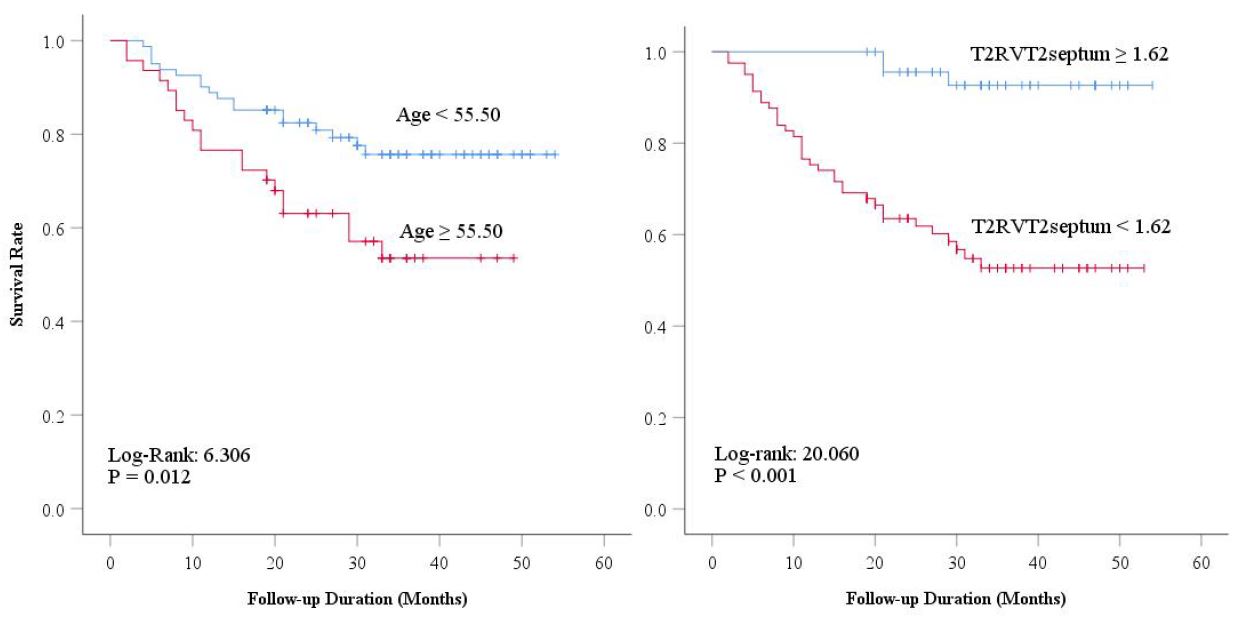
The sign of dark-RVBP on T2 mapping was found in 31.3% (42/134) of DCM patients. Values of T2RV, T2RV/T2LV and T2RV/T2septum in patients with dark-RVBP were significantly lower than that in patients with bright-RVBP relatively bright RVBP and in HC, all P < 0.001. Global myocardial circular strain (GCS) and global longitudinal strain (GLS) of LV and RV showed significant differences between dark-RVBP, bright RVBP and bright-RVBP groups, all P < 0.001. During a median follow-up of 30 months, 38 patients experienced MACEs. In multivariate Cox regression analysis, age and T2RV/T2septum remained independent predictor of MACEs (hazard ratio = 2.320 and 13.408, respectively; P < 0.05 for both). In Kaplan–Meier analysis, patients with age > 55.50 and the ratio of T2RV/T2septum < 1.62 had signifcantly higher rate of MACEs (log-rank = 6.306, P = 0.012 and log-rank = 20.060, P < 0.001, respectively).DISCUSSION
To our best knowledge, this was the first clinical experience evaluating the prognostic value of the dark right ventricular blood pool sign on T2 mapping by CMR in DCM patients. About 31% of DCM patients had significantly blurred septal myocardium due to dark right ventricular blood pool on the T2 mapping. Some researcher [3] have found that the estimation of venous O2 saturation from the measurements of T2 value of the blood pool was in good agreement with the measurement obtained by invasive catheterization. Higher T2mapping signal indicates higher oxygen saturation of blood. T2 mapping by CMR may non-invasive reflect differential blood oxygenation between the left and right heart (ΔSaO2) to predict adverse prognosis in patients with DCM.CONCLUSION
The sign of dark-RVBP on T2 mapping by CMR was associated with hard clinical events with prognostic information independent of and incremental to myocardial strain parameters.Acknowledgements
noneReferences
[1] Messroghli DR, Moon JC, Ferreira VM, et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI) [published correction appears in J Cardiovasc Magn Reson. 2018 Feb 7;20(1):9]. J Cardiovasc Magn Reson. 2017;19(1):75. Published 2017 Oct 9. doi:10.1186/s12968-017-0389-8[2] Emrich T, Bordonaro V, Schoepf UJ, et al. Right/Left Ventricular Blood Pool T2 Ratio as an Innovative Cardiac MRI Screening Tool for the Identification of Left-to-Right Shunts in Patients With Right Ventricular Disease [published online ahead of print, 2021 Aug 10. J Magn Reson Imaging. 2021;10.1002/jmri.27881. doi:10.1002/jmri.27881[3] Varghese J, Potter LC, LaFountain R, et al. CMR-based blood oximetry via multi-parametric estimation using multiple T2 measurements. J Cardiovasc Magn Reson. 2017;19(1):88. Published 2017 Nov 9. doi:10.1186/s12968-017-0403-1Figures