1385
Assessing the microstructural integrity of the myocardium in hypertrophic cardiomyopathy using diffusion tensor imaging and strain analysis.1Cardiovascular Innovation Research Center, Heart Vascular Thoracic Institute, Cleveland Clinic, Cleveland, OH, United States, 2DZHK (German Centre for Cardiovascular Research), partner site Berlin, Berlin, Germany, 3Berlin Ultrahigh Field Facility (B.U.F.F.), Max Delbrueck Center for Molecular Medicine in the Helmholtz Association, Berlin, Germany, 4Imaging Institute, Cleveland Clinic, Cleveland, OH, United States, 5Department of Biomedical Engineering, Case Western Reserve University & Cleveland Clinic, Cleveland, OH, United States
Synopsis
Keywords: Myocardium, Cardiomyopathy, microstructure, diffusion, strain.
Motivation: Although functional integrity is preserved in most hypertrophic cardiomyopathy (HCM) patients, the microstructure is continuously and silently changing.
Goal(s): To better comprehend the myocardial response, we need to characterize diffusion changes between healthy and disease state.
Approach: We quantitatively investigate the relationship between myocardial strain and diffusion tensor imaging (DTI)-derived metrics in HCM. We assessed diffusion and strain in HCM and healthy patients using a new investigational MR system with ultra-high-performance gradients.
Results: HCM subjects exhibited lower anisotropy values that correlated with strain analysis indicative of early microstructural disarray.
Impact: Our results highlight the contribution of microstructural anisotropy in HCM development. Even in the absence of detectable mechanical deficiencies, diffusion myocardial mapping is an adjunct tool for managing the disease, aiding treatment planning, and bridging clinical outcomes with research findings.
Introduction
Hypertrophic cardiomyopathy (HCM) is a cardiac disease characterized by extensive myocardial remodeling, often resulting in disorganization of the cellular environment and myofiber disarray 1,2. To investigate these changes, diffusion tensor cardiac imaging (DT-CMR) has been employed to map the diffusion patterns of water molecules and their directional shifts in both diseased and healthy cardiac tissue 3. Mean diffusivity (MD) evaluates the freedom of diffusion within the tissue, helix angle (HA) reflects its orientation and fractional anisotropy (FA) shows the degree of diffusion freedom 4. While previous studies have explored these factors, their precise influence on the mechanical performance of myofibers in clinical contexts remains uncertain 5,6. In this study, we aim to assess myocardial microstructure and its response using DTI and strain analysis, even in the absence of overt dysfunction, by leveraging a new MR system with ultra-high-performance gradient technology. Our goal is to ultimately contribute to the understanding and management of HCM.Methods
After approval from the institutional review board at Cleveland Clinic, we conducted MRI scans on a cohort of 10 patients diagnosed with HCM (4 males, mean age 58.5 years) and 10 healthy controls (4 males, mean age 46.8 years). These scans were performed with an advanced 3T MR system (MAGNETOM Cima.X, Siemens Healthineers AG, Erlangen, Germany), which offers a maximum gradient strength of 200 mT/m. Scans were performed under free-breathing conditions with a DT-CMR protocol consisting of a 2DRF zoomed diffusion prepared spin echo 7, FOV=350 mm, matrix=128 x 48, 5 slices, 8 mm slice thickness, TR=500 ms, 1 b0 acquisition, 12 diffusion directions at b=500 s/mm2, 8 averages. Global MD, HAT and FA values, were calculated over the entire LV. Global LV function and strain were quantified using Segment v3.3 R10187 (Medviso, segment.heiberg.se).Results
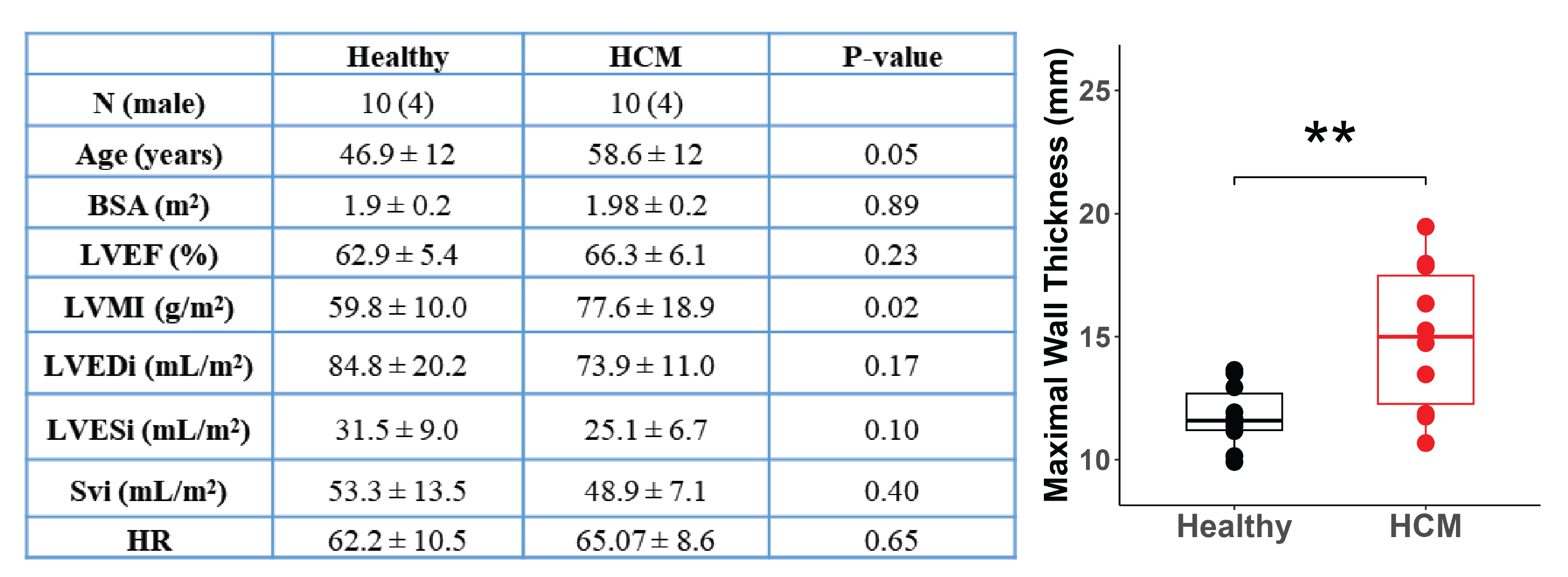
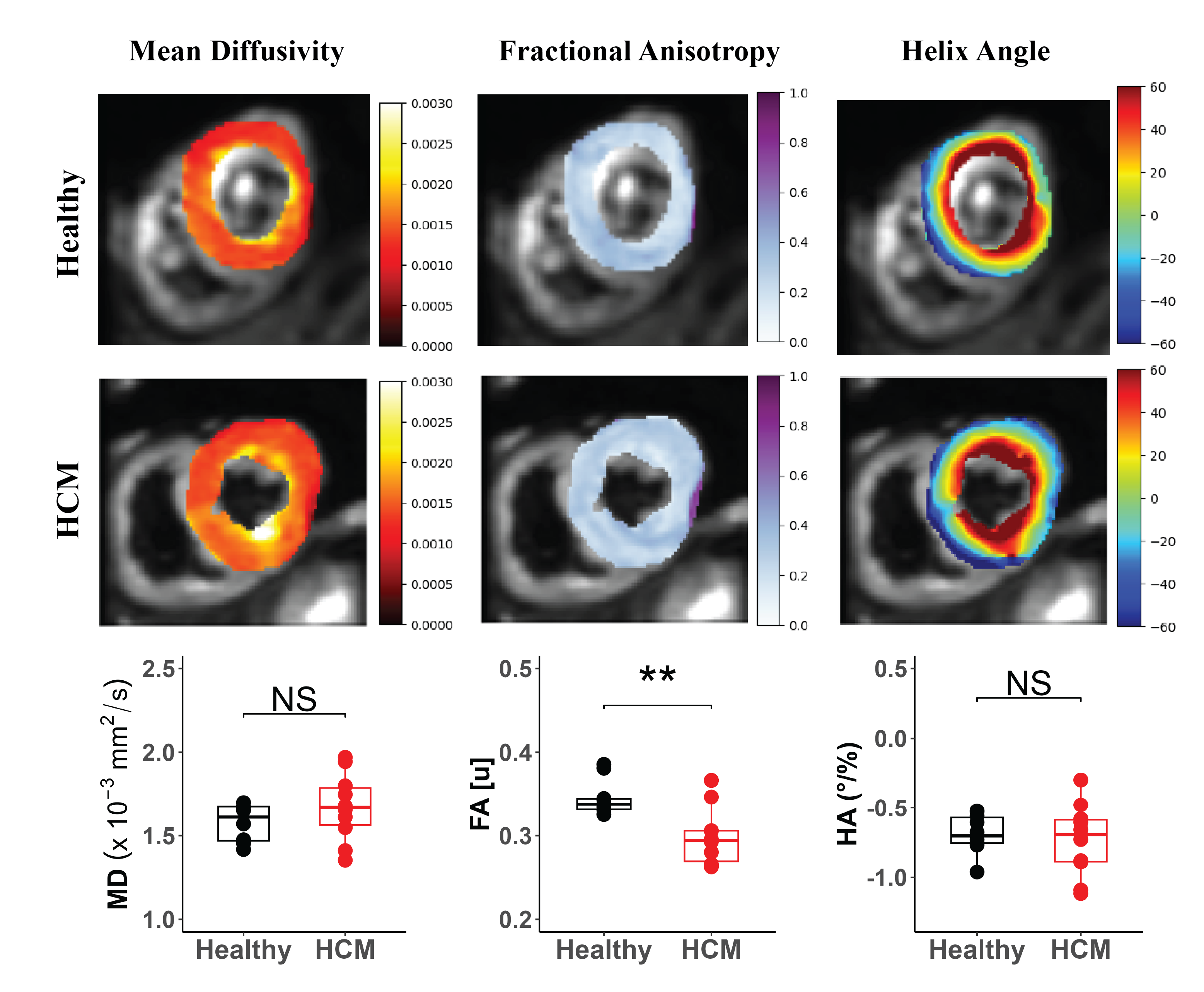
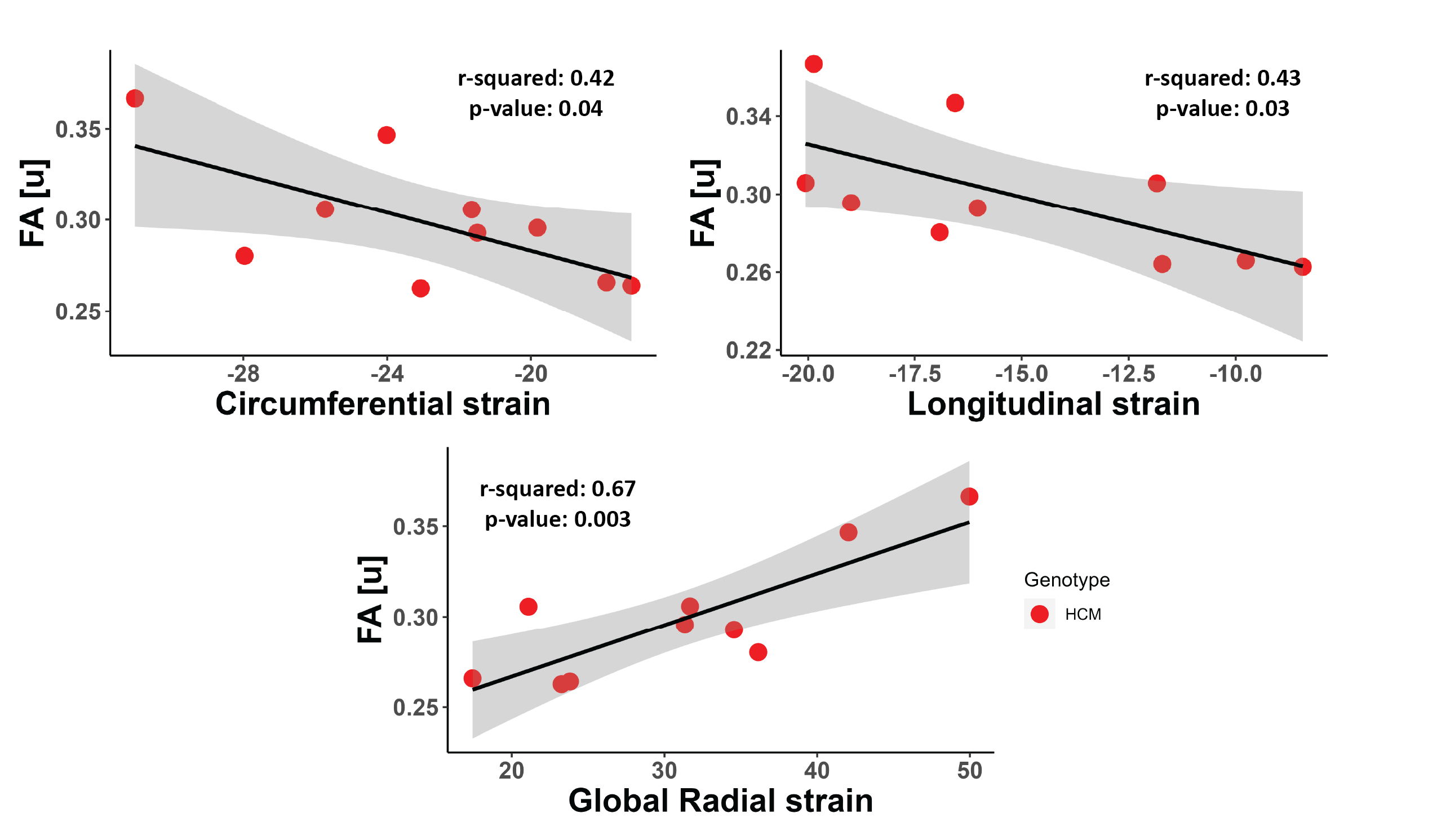
HCM patients had a preserved left ventricular ejection fraction (LVEF) (HCM = 66.3 ± 6.1, Healthy = 62.9 ± 5.4, p>0.23) although they showed significant left ventricular hypertrophy (LVH) (HCM = 14.9 ± 2.8 mm, Healthy = 11.7 ± 1.2 mm, p>0.006). All other functional parameters were not significantly different compared to healthy group (Figure 1). On the other hand, DTI analysis revealed significantly decreased fractional anisotropy (FA) values in HCM patients (mean FA = 0.29 ± 0.03) compared to healthy controls (mean FA = 0.34 ± 0.02) (p<0.003) (Figure 2). Mean diffusivity (MD) and helix angle (HA) showed no significant difference between the two groups but were positively correlated (r2 = 0.55, p<0.001). Further, we investigated the relationship between strain and FA in HCM patients, this revealed a negative correlation between FA and longitudinal and circumferential strain (r2 = 0.43, p<0.04 and r2 = 0.42, p<0.05 respectively) and a positive correlation with global radial strain (r2 = 0.67, p<0.004) (Figure 3). This highlights the potential impact of microstructural changes on mechanical integrity of myocardial fibers.Discussion
Preserved LVEF in the presence of hypertrophy is common in HCM and can often hide early signs of diastolic dysfunction 8. Quantitative assessment of FA showing low values in HCM compared to healthy counterparts can support this hypothesis and is consistent with prior studies 3. The correlation found between FA and strain parameters shows the complexity of deformation patterns that can be caused by early microstructural disruption. Our findings further elucidate the importance of quantitative assessment in disease management 6.Conclusion
Our results demonstrate the importance of comprehensive myocardial characterization in the context of HCM. Newly available ultra-high-performance scanners make these measurements accessible for special patients care. Next step would be to assess regional differences in strain and diffusion in a larger sample. Future investigations may delve into the potential impact of sex on the observed patterns, which could help understand the early variabilities in myocardial architecture in HCM patients.Acknowledgements
No acknowledgement found.References
1 Oldfield, C. J., Duhamel, T. A. & Dhalla, N. S. Mechanisms for the transition from physiological to pathological cardiac hypertrophy. Can J Physiol Pharmacol 98, 74-84 (2020). https://doi.org:10.1139/cjpp-2019-0566
2 Musumeci, B. et al. Left Ventricular Remodeling in Hypertrophic Cardiomyopathy: An Overview of Current Knowledge. J Clin Med 10 (2021). https://doi.org:10.3390/jcm10081547
3 Joy, G. et al. Microstructural and Microvascular Phenotype of Sarcomere Mutation Carriers and Overt Hypertrophic Cardiomyopathy. Circulation 148, 808-818 (2023). https://doi.org:10.1161/CIRCULATIONAHA.123.063835
4 Khalique, Z. et al. Diffusion Tensor Cardiovascular Magnetic Resonance Imaging: A Clinical Perspective. JACC Cardiovasc Imaging 13, 1235-1255 (2020). https://doi.org:10.1016/j.jcmg.2019.07.016 5 Lee, H. J. et al. Supplementary role of left ventricular global longitudinal strain for predicting sudden cardiac death in hypertrophic cardiomyopathy. Eur Heart J Cardiovasc Imaging 23, 1108-1116 (2022). https://doi.org:10.1093/ehjci/jeab187
6 Sharrack, N. et al. The relationship between myocardial microstructure and strain in chronic infarction using cardiovascular magnetic resonance diffusion tensor imaging and feature tracking. J Cardiovasc Magn Reson 24, 66 (2022). https://doi.org:10.1186/s12968-022-00892-y
7 Nguyen, C. T. et al. Free-breathing diffusion tensor MRI of the whole left ventricle using second-order motion compensation and multitasking respiratory motion correction. Magn Reson Med 85, 2634-2648 (2021). https://doi.org:10.1002/mrm.28611
8 Chamsi-Pasha, M. A., Zhan, Y., Debs, D. & Shah, D. J. CMR in the Evaluation of Diastolic Dysfunction and Phenotyping of HFpEF: Current Role and Future Perspectives. JACC Cardiovasc Imaging 13, 283-296 (2020). https://doi.org:10.1016/j.jcmg.2019.02.031
Figures