1380
Superior Visualization of Moyamoya Disease Collaterals: A Comparative Analysis of 5.0T vs. 3.0T Time-of-Flight Magnetic Resonance Angiography1Department of Radiology, State Key Laboratory of Complex Severe and Rare Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 2Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Beijing, China, 3China National Clinical Research Center for Neurological Diseases, Beijing, China, 4Department of Neurosurgery, Beijing Hospital, National Center of Gerontology, Beijing, China, 5Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, China, 6MR Collaboration, United Imaging Research Institute of Intelligent Imaging, Beijing, China, 7United Imaging Research Institute of Intelligent Imaging, Beijing, China, 8Department of Neurology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
Synopsis
Keywords: Blood Vessels, Blood vessels, 5.0-T magnetic resonance angiography
Motivation: Limited studies have scrutinized the capability of MRI in evaluating collateral circulation in Moyamoya Disease (MMD), with 3.0T TOF MRA often lacking the necessary precision.
Goal(s): To systematically compare the effectiveness of 5.0T and 3.0T TOF MRA in depicting the complex vascular networks in MMD patients.
Approach: A retrospective study on 21 MMD patients was performed using both 5.0T and 3.0T MRI systems, focusing on the visibility of moyamoya vessels, leptomeningeal anastomoses, and basal ganglia signal intensity.
Results: The study found that 5.0T MRA significantly outperforms 3.0T in visualizing the fine details of MMD's vascular architecture.
Impact: The introduction of 5.0T MRA into clinical practice could revolutionize the imaging landscape for Moyamoya Disease, offering superior diagnostic clarity and aiding in the precise evaluation of cerebrovascular collateral networks, which is critical for surgical planning and patient prognosis.
Introduction
Moyamoya disease (MMD) represents a critical cerebrovascular challenge, with its insidious progression marked by the gradual occlusion of the intracranial internal carotid artery (ICA) and an intricate dance of collateral network formation1. This compensatory angiogenesis is pivotal, as it is intimately tied to clinical outcomes and therapeutic trajectories in patients with acute ischemic stroke2-4. Despite its clinical significance, the imaging evaluation of these collateral pathways in MMD via MRI has remained suboptimal, with many nuances of the disease's vascular architecture escaping the resolution of standard 3.0T Time-of-Flight (TOF) Magnetic Resonance Angiography (MRA) 5,6.The technological leap to ultra-high-field MRI systems such as 7.0T has been a game-changer in neuroimaging, offering unprecedented clarity by leveraging heightened signal-to-noise ratios and elongated T1 relaxation times7-9. However, the clinical application of such systems remains in its infancy. In particular, the 5.0T MRI system, a newcomer to the clinical research arena, shows promise in bridging the gap, boasting image quality that not only contends with that of the 7.0T but also significantly outpaces the 3.0T system in visualizing minute vascular structures10. Despite these advancements, comparisons between the leptomeningeal angiographic details captured by 3.0T MRI and those by ultra-high-field systems have been scant. Herein, we endeavor to fill this gap through a systematic comparison of 5.0- and 3.0T TOF MRA in visualizing the collateral circulation of MMD, which may hold the key to unlocking a new frontier in MMD management.Materials and Methods
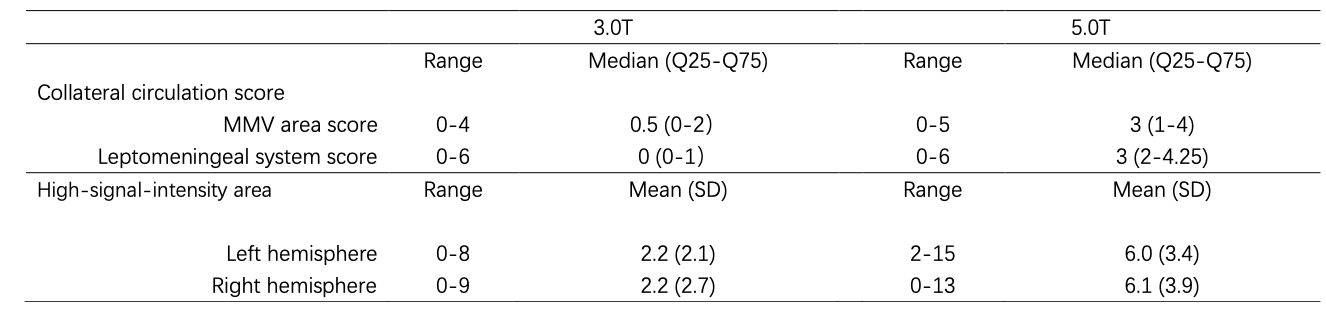
Our retrospective analysis spanned 30 symptomatic hemispheres from 21 patients diagnosed with ischemic-type MMD, featuring a diverse cohort of 10 males and 11 females ranging from 7 to 39 years of age. Each subject was scanned using both 5.0T and 3.0T MRI systems, allowing for a direct comparison of the imaging capabilities of each modality. We employed a 0-5 grading system to quantify the visibility of moyamoya vessels across five cerebrovascular regions 7.Similarly, leptomeningeal anastomoses were scored from 0 to 6, reflecting the complexity of the collateral networks spanning the pPCA to ACA, and the anterior temporal branch of the PCA to the MCA. Manual counts of flow voids in the basal ganglia supplemented our imaging data. A Wilcoxon matched-pair signed-rank test was applied for statistical comparison of moyamoya vessel and leptomeningeal system scores across the two MRI systems. Furthermore, a paired t-test facilitated the comparison of flow void counts between the 5.0T and 3.0T images, providing a quantitative foundation for our evaluation.Results
The 5.0T TOF MRA system exhibited a remarkable improvement in the detection capabilities over its 3.0T counterpart. The moyamoya vessel (MMV) area scores were notably higher on the 5.0T MRA (z=-4.633, p = 0.001), indicating a superior visualization of the intricate moyamoya vessels. The leptomeningeal system scores followed suit, with statistically significant improvements in detail and clarity (p=0.001). High-signal-intensity areas within the basal ganglia were not only more frequently detected with the 5.0T system but also with greater clarity (left hemishpere: t=-6.616, p < 0.001; right hemishpere: t=-4.387, p < 0.001 ), suggesting an enhanced sensitivity to the subtle contrasts in tissue signal that often elude lower-field systems.Discussion
he findings of our study underscore the superior diagnostic prowess of 5.0T TOF MRA, which could potentially revolutionize the imaging approach to MMD. This technology may enable clinicians to discern the fine vascular details crucial for surgical planning, prognostication, and therapeutic decision-making. Furthermore, the improved visualization of collateral pathways could facilitate earlier diagnosis, allowing for timely interventions that may alter the disease course and improve patient outcomes.Conclusion
The 5.0T TOF MRA emerges as a formidable tool in the imaging arsenal against MMD, promising enhanced visualization of the disease's vascular nuances. Its application may herald a new era in the diagnosis, assessment, and management of Moyamoya disease, ultimately contributing to the refinement of therapeutic strategies and the betterment of patient care.Acknowledgements
No acknowledgement found.References
1. Guidelines for diagnosis and treatment of moyamoya disease (spontaneous occlusion of the circle of Willis). Neurol Med Chir (Tokyo). 2012;52(5):245-66. doi:10.2176/nmc.52.245
2. Fanou EM, Knight J, Aviv RI, et al. Effect of Collaterals on Clinical Presentation, Baseline Imaging, Complications, and Outcome in Acute Stroke. AJNR Am J Neuroradiol. Dec 2015;36(12):2285-91. doi:10.3174/ajnr.A4453
3. Shuaib A, Butcher K, Mohammad AA, Saqqur M, Liebeskind DS. Collateral blood vessels in acute ischaemic stroke: a potential therapeutic target. Lancet Neurol. Oct 2011;10(10):909-21. doi:10.1016/s1474-4422(11)70195-8
4. Liu ZW, Han C, Zhao F, et al. Collateral Circulation in Moyamoya Disease: A New Grading System. Stroke. Oct 2019;50(10):2708-2715. doi:10.1161/strokeaha.119.024487
5. Jin Q, Noguchi T, Irie H, et al. Assessment of Moyamoya disease with 3.0-T magnetic resonance angiography and magnetic resonance imaging versus conventional angiography. Neurol Med Chir (Tokyo). 2011;51(3):195-200. doi:10.2176/nmc.51.195
6. Filimonova E, Ovsiannikov K, Rzaev J. Neuroimaging in Moyamoya angiopathy: Updated review. Clin Neurol Neurosurg. Nov 2022;222:107471. doi:10.1016/j.clineuro.2022.107471
7. Deng X, Zhang Z, Zhang Y, et al. Comparison of 7.0- and 3.0-T MRI and MRA in ischemic-type moyamoya disease: preliminary experience. J Neurosurg. Jun 2016;124(6):1716-25. doi:10.3171/2015.5.Jns15767
8. Oh BH, Moon HC, Baek HM, et al. Comparison of 7T and 3T MRI in patients with moyamoya disease. Magn Reson Imaging. Apr 2017;37:134-138. doi:10.1016/j.mri.2016.11.019
9. Matsushige T, Kraemer M, Sato T, et al. Visualization and Classification of Deeply Seated Collateral Networks in Moyamoya Angiopathy with 7T MRI. AJNR Am J Neuroradiol. Jul 2018;39(7):1248-1254. doi:10.3174/ajnr.A5700
10. Shi Z, Zhao X, Zhu S, et al. Time-of-Flight Intracranial MRA at 3 T versus 5 T versus 7 T: Visualization of Distal Small Cerebral Arteries. Radiology. Dec 2022;305(3):E72. doi:10.1148/radiol.229027
Figures
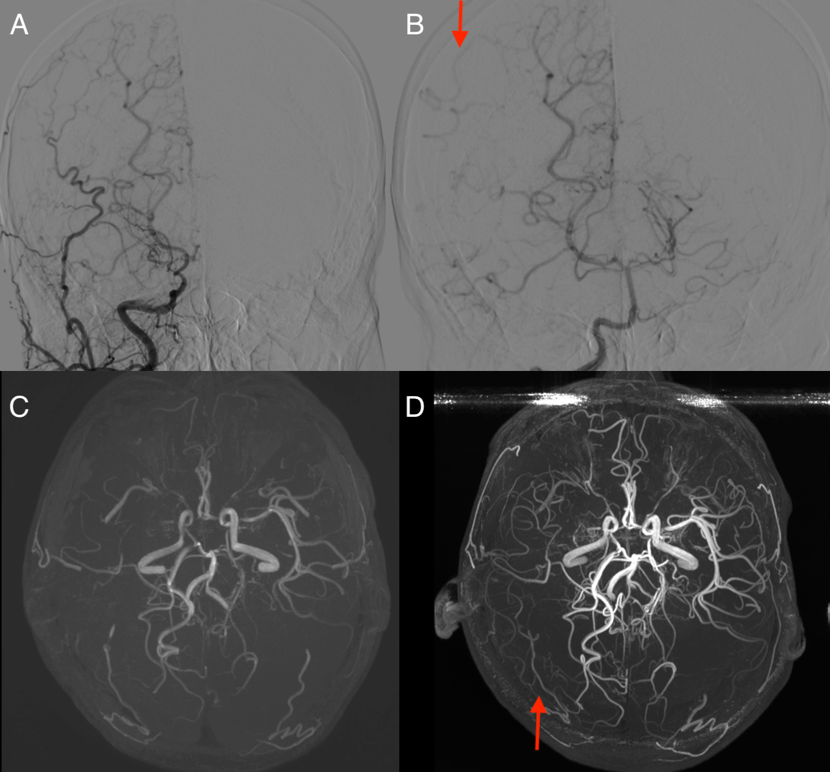
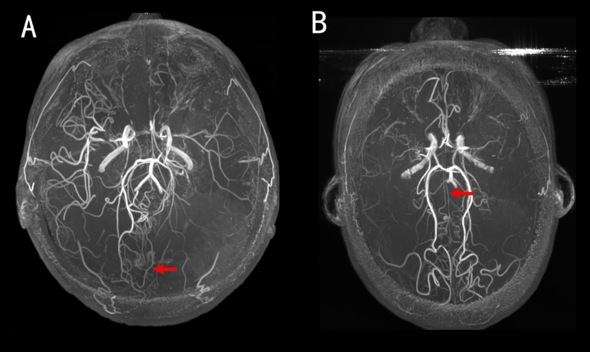
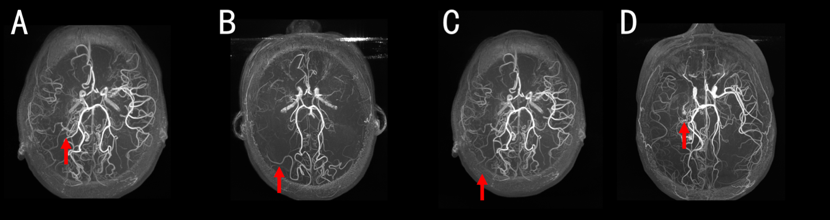
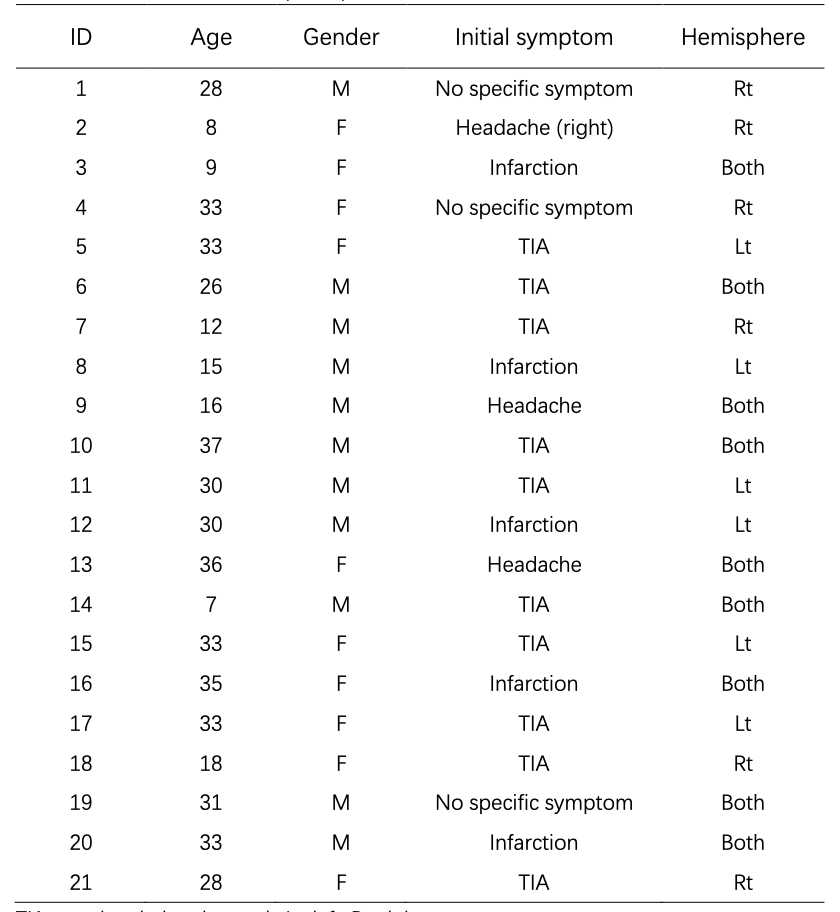
Table 1. Characteristics of the participants
TIA: transient ischemic attack, Lt: left, Rt: right.