1377
The value of non- and super-selective 4D-MRA in the assessment of internal carotid artery occlusion: comparison with TOR-MRA and CE-MRA1Radiology, Renji hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China, 2Renji Hospital, School of Medicine, Shanghai Jiaotong University, Shanghai, China, 3Philips Healthcare, Shanghai, China
Synopsis
Keywords: Vessel Wall, Vessels
Motivation: 4D-MR angiography techniques have been developed to visualize both luminal stenosis and collateral circulation.
Goal(s): This study aimed to assess whether 4D-MRA (4D-PACK and 4D-S-PACK) can be used as a noninvasive alternative to intraarterial DSA in internal carotid artery occlusion (ICAO).
Approach: We prospective enrolled patients diagnosed as internal carotid artery occlusion by ultrasound or CTA and scheduled for intra-arterial DSA for this study. All patients underwent carotid multi-contrast MR imaging and DSA.
Results: 4D-PACK and 4D-S-PACK can be used to diagnose ICAO, type of Circle of Willis (CoW), collateral circulation via CoW and blood flow direction of cerebral arteries.
Impact: We offered a noninvasive alternative to intraarterial DSA to diagnose ICAO, type of CoW, collateral circulation via CoW and blood flow direction. By using three durations, we could greatly reduce time cost while ensuring the accuracy of 4D-PACK and 4D-S-PACK.
Introduction
Acute ischemic stroke by internal carotid artery occlusion (ICAO) is known to have relatively high rate of ischemic progression and recurrence. Ipsilateral middle cerebral artery (MCA) flow via primary collateral circulation has been known to protect cerebral tissue from the progression of ischemic insult. The circle of Willis (CoW) plays an important role in the primary collateral circulation. Detailed anatomical and hemodynamic blood flow information in the CoW of ICAO patients is important.Methods
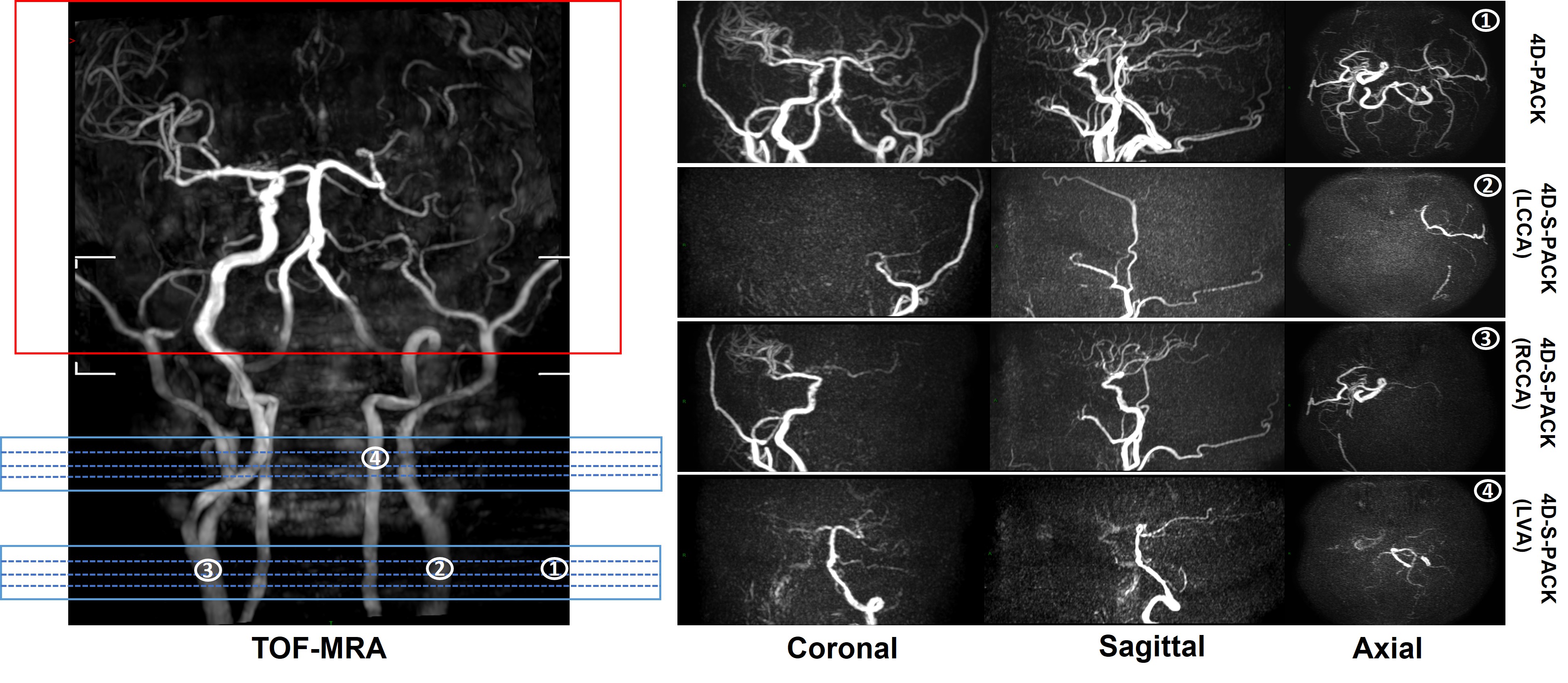
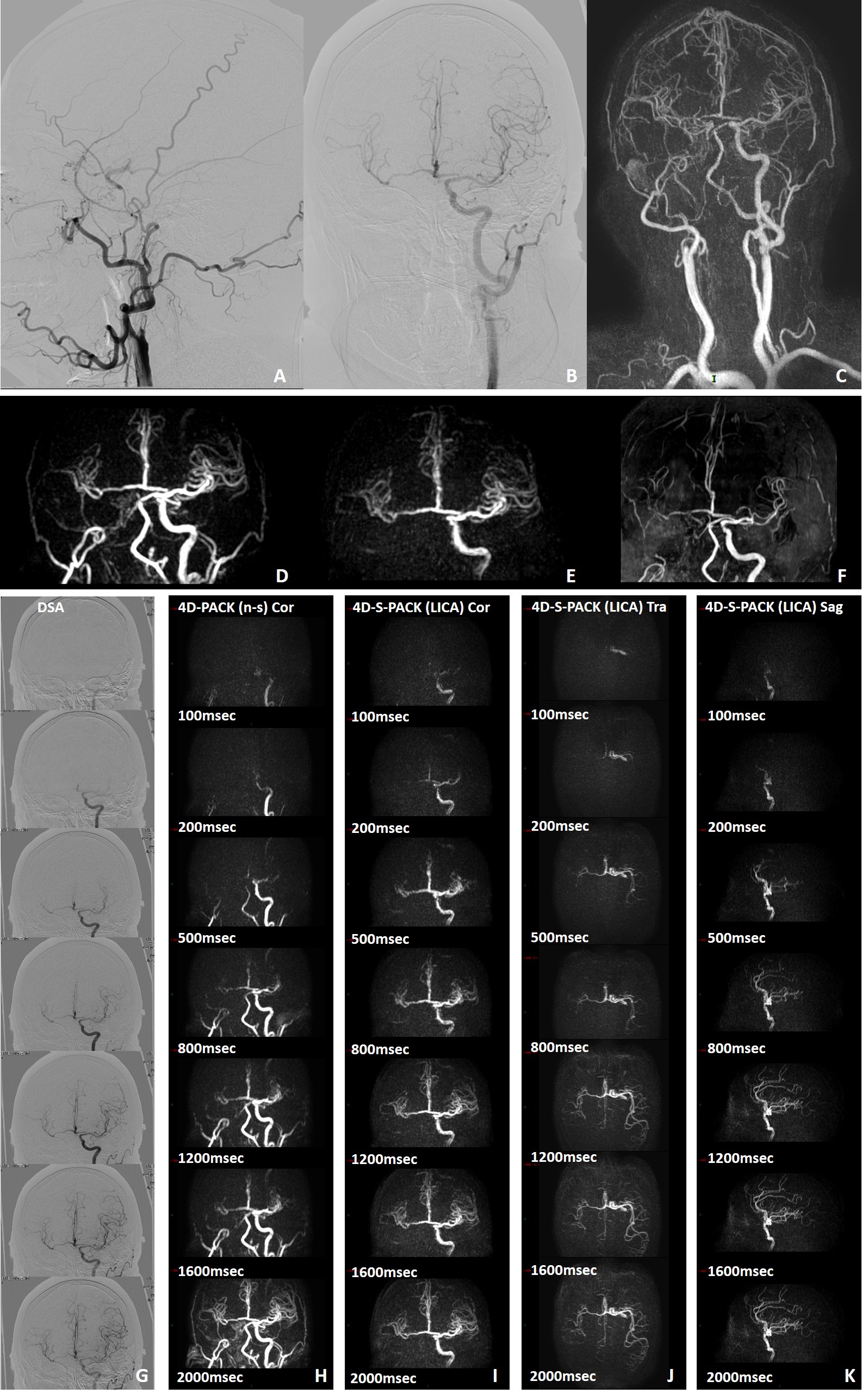
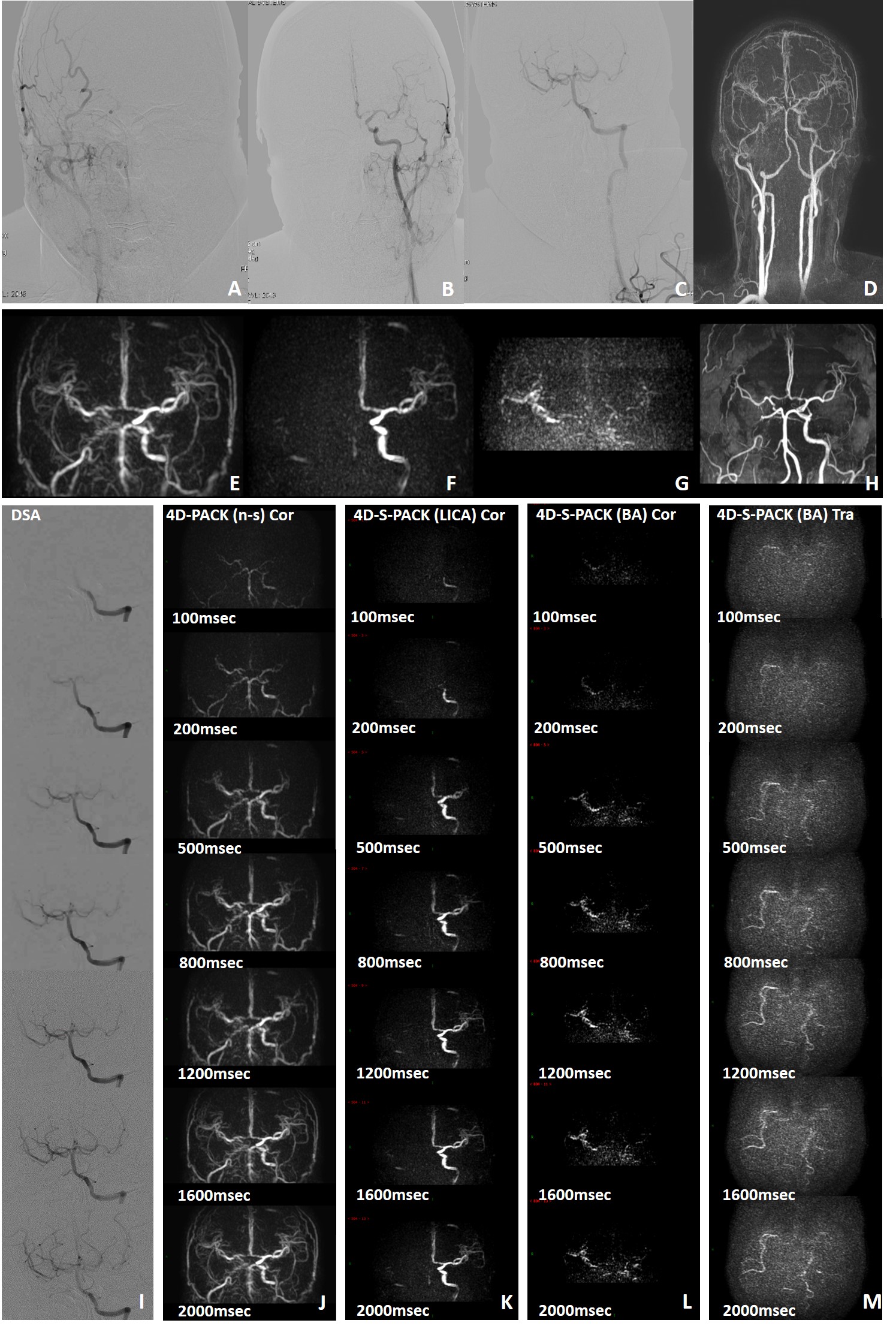
We prospective enrolled patients diagnosed as ICAO scheduled for intra-arterial DSA for this study. All patients underwent carotid multi-contrast MR imaging and DSA within 1 week. Carotid artery MR imaging was performed on a 3.0T whole-body MR scanner (Philips Ingenia, TX). A multi-contrast carotid MR imaging protocol was conducted to acquire 3D-TOF-MRA, 4D-PACK, 4D-S-PACK, and CE-MRA in turn. 4D-MRA images were obtained by changing the label duration between 100, 200, 500, 800, 1200, 1600, and 2000 ms. The following variables were assessed on DSA and corresponding MR images: (A) internal carotid artery occlusion or not; (B) type of CoW; (C) collateral circulation via CoW. Besides, for super-selective 4D-S-PACK, we evaluated its feasibility of evaluating blood flow direction of cerebral arteries from all durations and each duration. We also assessed the accuracy of evaluating blood flow direction of cerebral arteries by 4D-S-PACK with different durations, using DSA as reference.Results
From October 2022 to June 2023, a total of 19 patients with 21 ICAO were enrolled for the final analysis. Both Inter-reader and intra-reader agreement was excellent for determining ICAO, type of CoW, collateral circulation via CoW and symmetry of MCA angiography by 4D-MRA (all Cohen’s κ >0.80; P<0.05). The identification of ICAO on different MR sequences is summarized in Table 2. The sensitivity, specificity, and accuracy for each MRA sequence on the assessment of ICAO was all 100.0%, using DSA as reference. The sensitivity, specificity and accuracy of diagnosing CoW types was 100.0%, 95.8% and 98.2% by 4D-MRA, 100.0%, 88.5% and 94.7% by TOF-MRA, and 97.1%, 100.0% and 98.2% by CE-MRA, respectively. 4D-MRA performed the best in the assessment of primary collateral circulation pattern, with sensitivity of 95.2%, specificity of 100.0%, and accuracy of 98.2% in the reference of DSA. CE-MRA was not far behind, with sensitivity of 100.0%, specificity of 86.1%, and accuracy of 91.2%. The sensitivity, specificity, and accuracy for TOF-MRA was 85.7%, 86.1%, and 86.0%, respectively, ranking the third place. We evaluated the feasibility of evaluating blood flow direction of cerebral arteries from all durations and each duration of 4D-S-PACK. We divided 4D-S-PACK into four groups: group 1 with 7 durations; group 2 with 5 durations; group 3 with 3 durations; and group 4 with only 1 duration. The accuracy of diagnosing blood flow direction was 98.2%, 98.2%, 98.2%, and 96.5% and the time cost was 5 min 16 s, 4 min 7 s, 2 min 10 s and 2 min 6 s, respectively, from group 1 to group 4. 4D-S-PACK with 3 durations including 100 msec, 800 msec, 2000 msec has greatly reduced the time cost while ensuring the accuracy.Discussion
Few studies have used non-selective ASL-based 4D-MR angiography for visualizing ICAO. The accuracy was excellent for diagnosing ICAO, type of Circle of Willis (CoW), collateral circulation via CoW and blood flow direction of cerebral arteries by 4D-PACK and 4D-S-PACK. Time cost is important in the MR scanning. By using three durations, we could greatly reduce the time cost while ensuring the accuracy of 4D-PACK and 4D-S-PACK. It is of great use to patients with ICAO to evaluate collateral circulation and blood flow direction. Compared with the contralateral ICA and MCA, the CNRs of the patients’ distal MCA beyond ICAO were significantly lower when 4D-PACK and 4D-S-PACK were used. This finding could be due to the smaller amount of blood labeled by the super-selective labeling. From the C3 segment to the C6 segment of ICA, the CNRs of these tortuous vessels were lower than the relatively straight vessels. The signal reduction in 4D-PACK and 4D-S-PACK sometimes wrongly showed narrow and stenosis from the actual normal vessel. We found that the super-selective labeling put in the relatively vertical vessel and as close to the imaging area as possible could improve the CNRs in the processing of scanning.Conclusion
Non-contrast and non-invasive 4D-MR angiography has the potential to become an alternative imaging approach in diagnosing ICAO and initially assessing its blood supply pattern. By using three durations, we could greatly reduce the time cost while ensuring the diagnosis accuracy.Acknowledgements
None.References
1. Obara M., O. Togao, G.M. Beck, et al., Non-contrast enhanced 4D intracranial MR angiography based on pseudo-continuous arterial spin labeling with the keyhole and view-sharing technique. Magn Reson Med, 2018. 80(2): p. 719-725.
2. Togao O., A. Hiwatashi, M. Obara, et al., 4D ASL-based MR angiography for visualization of distal arteries and leptomeningeal collateral vessels in moyamoya disease: a comparison of techniques. Eur Radiol, 2018. 28(11): p. 4871-4881.
3. Obara M., O. Togao, M. Helle, et al., Improved selective visualization of internal and external carotid artery in 4D-MR angiography based on super-selective pseudo-continuous arterial spin labeling combined with CENTRA-keyhole and view-sharing (4D-S-PACK). Magn Reson Imaging, 2020. 73: p. 15-22.
4. Togao O., M. Obara, M. Helle, et al., Vessel-selective 4D-MR angiography using super-selective pseudo-continuous arterial spin labeling may be a useful tool for assessing brain AVM hemodynamics. European Radiology, 2020. 30(12): p. 6452-6463.
5. Togao O., M. Obara, K. Kikuchi, et al., Vessel-Selective 4D-MRA Using Superselective Pseudocontinuous Arterial Spin-Labeling with Keyhole and View-Sharing for Visualizing Intracranial Dural AVFs. AJNR Am J Neuroradiol, 2022. 43(3): p. 368-375.
Figures