1372
3D Free-Breathing Ungated Spiral bSSFP Functional Cardiac Imaging Using a Deep Image Prior1Radiology, University of Michigan, Ann Arbor, MI, United States, 2Biomedical Engineering, University of Michigan, Ann Arbor, MI, United States
Synopsis
Keywords: Machine Learning/Artificial Intelligence, Cardiovascular, deep learning; spiral; real-time CMR
Motivation: Real-time imaging methods are useful for patients with limited breathhold capacity or arrhythmias, but are typically limited to 2D scans that prevent evaluation of wall motion in 3D over the heart.
Goal(s): The goal of this project is to develop a technique for 3D real-time (free-breathing ungated) cine imaging.
Approach: The proposed method combines a highly undersampled 3D stack-of-spirals trajectory with a deep image prior reconstruction, which does not require ground truth training data.
Results: Real-time 3D imaging is demonstrated in healthy subjects with temporal resolutions of 36ms per volume at 1.5T and 58ms per volume at 0.55T.
Impact: Real-time 3D imaging could enable streamlined cardiac MRI exams, with whole-heart 3D cine images obtained in 10s without breathholds or gating. This technique may also simplify quantification compared to 2D real-time methods, since motion is synchronized over all partitions.
Introduction
Real-time imaging methods are useful for patients with limited breathhold capacity or arrhythmias but are typically limited to 2D scans. Different slices are collected at different points in time, precluding evaluation of wall motion in 3D over the entire heart. Additionally, measuring ventricular volumes and ejection fraction (EF) can be labor-intensive, as images at diastole and systole must be identified for each slice separately. This study develops an approach for 3D real-time bSSFP cine imaging using self-supervised deep learning, with feasibility in healthy subjects demonstrated at <60ms and <40ms temporal resolution per volume at 0.55T and 1.5T, respectively.Methods
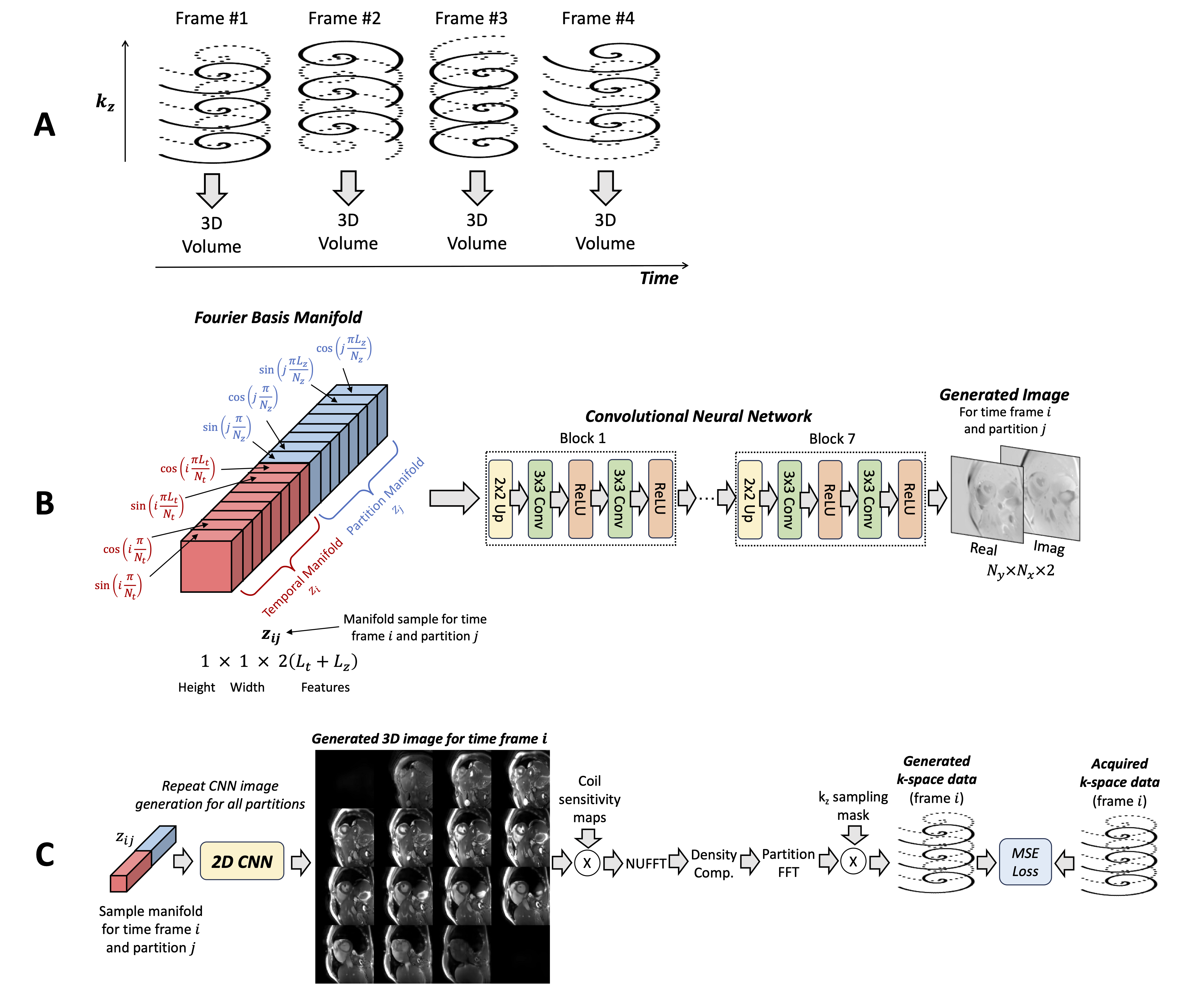
Acquisition: Data were acquired using 3D stack-of-spirals sampling with 48 interleaves.1 The 3D k-space was filled by collecting all partitions before rotating the spiral by the golden angle (Figure 1a).2 Interleaved R=2 undersampling was applied along the partition direction, and each volume was reconstructed using only one interleaf and all acquired partitions, resulting in a net acceleration of R=96.Reconstruction: A Time-and-Partition Dependent Deep Image Prior (DIP) reconstruction was developed that extends the Time-Dependent DIP by Yoo et al. for 2D dynamic imaging.3,4 A convolutional neural network (CNN) was used to generate time-resolved 3D images without ground truth training data. To improve efficiency, 2D (rather than 3D) convolutions were used by parameterizing the time index i and partition index j on a low-dimensional manifold (Figure 1b). A point on the manifold was input to the CNN to generate a 2D image; this was repeated for all time frames and partitions to obtain time-resolved 3D images. The manifold consisted of Fourier basis functions as follows, with lower-frequency sinusoids favoring smooth changes and higher-frequency sinusoids recovering rapid motion, with $$$N_t$$$ time frames and $$$N_z$$$ partitions.
$$z_i = [sin(\pi i/N_t), cos(\pi i/N_t),sin(2\pi i/N_t),cos(2\pi i/N_t),...,sin(L_t\pi i/N_t),cos(L_t\pi i/N_t)]$$ $$z_j=[sin(\pi j/N_z), cos(\pi j/N_z),sin(2\pi j/N_z),cos(2\pi j/N_z),...,sin(L_z\pi j/N_z),cos(L_z\pi j/N_z)]$$
$$$L_t$$$ and $$$L_z$$$ determined the highest frequency sinusoids and were set using $$$L_t=\lfloor log_2(N_t) \rfloor=8$$$ and $$$L_z=\lfloor log_2(N_z) \rfloor=4$$$. The final manifold sample $$$z_{ij}$$$ was obtained by concatenating $$$z_i$$$ and $$$z_j$$$. Training (Figure 1c) was performed in mini-batches of one 3D volume by calculating the forward encoding model, including coil sensitivities and gridding.5 The MSE loss was computed with respect to acquired k-space data to optimize the CNN weights. Training was performed de novo after each scan for 500 epochs and required 26 hours on a GPU.
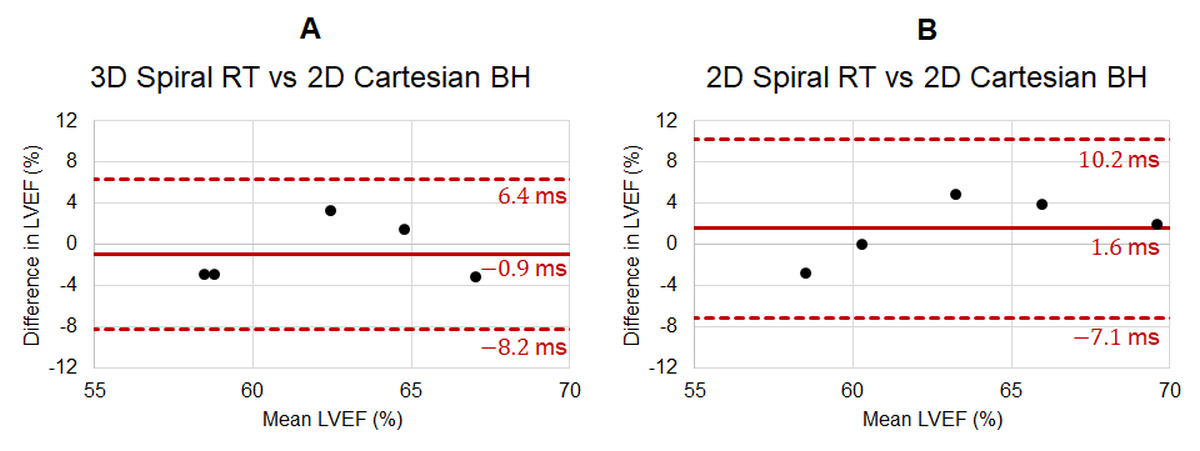
Experiments: Short-axis cardiac data were collected in five healthy subjects at 1.5T (MAGNETOM Sola, Siemens Healthineers, Erlangen, Germany). Real-time 3D spiral data were obtained with 16 partitions, 300x300mm2 FOV, 2.2x2.2x8.0mm3, and TR/TE=4.5/1.4ms. 288 time-resolved 3D images were collected over 10.4s at a temporal resolution of 36ms per volume. Additionally, real-time 2D spiral data were collected using a Time-Dependent DIP4 reconstruction (34ms/frame, R=6). A 2D breathheld ECG-gated Cartesian cine scan with 25 phases was acquired for reference. LVEF values were compared using Bland-Altman6 plots after manual contouring. To demonstrate translatability on a commercial low-field system, two subjects were scanned at 0.55T (MAGNETOM Free.Max), where lower gradient performance resulted in temporal resolutions of 50ms for 2D and 58ms (per volume) for 3D real-time scans.
Results
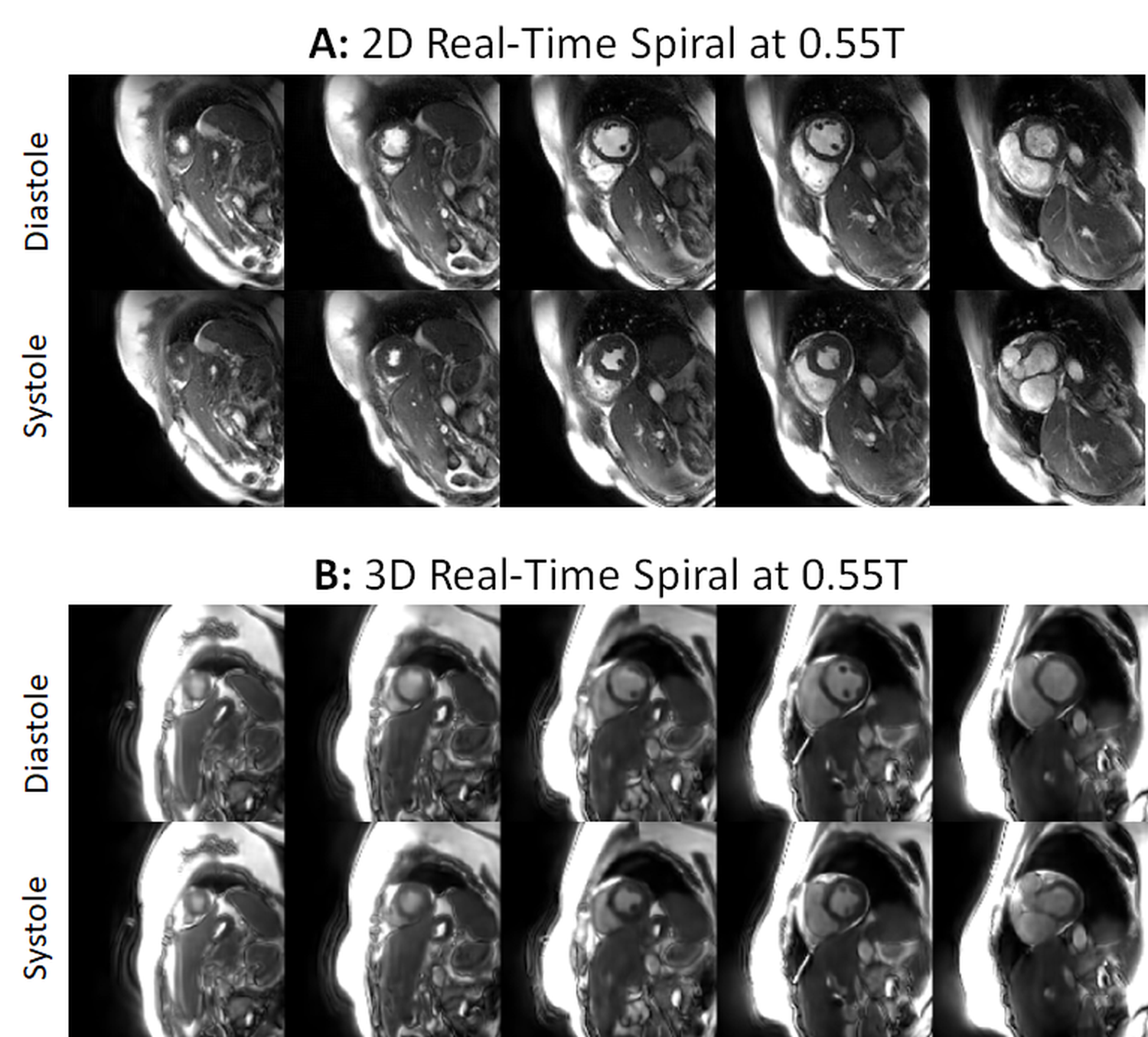
Figures 2 and 3 show 2D and 3D real-time images from the same subject at 1.5T. Respiratory and cardiac motion are synchronized over all partitions for the 3D scan, enabling evaluation of motion over the entire LV, unlike the 2D scan, where each slice is imaged at a different point in time. Bland-Altman plots in Figure 4 compare LVEF from 2D and 3D real-time methods with the 2D reference scan. The mean bias and 95% limits of agreement were -0.9% (-8.2%, 6.4%) for 3D real-time vs the 2D reference. Figure 5 presents 2D and 3D real-time images from one subject acquired at 0.55T.Discussion
The study demonstrates the feasibility of 3D real-time functional cardiac imaging by combining a highly undersampled stack-of-spirals trajectory with a deep image prior. This technique may enable streamlined exams, as whole-heart 3D cine images could be obtained without breathholds or gating in a 10-second scan. This technique may simplify volume and EF measurements since motion can be evaluated synchronously over the entire heart. Future studies will explore whether real-time 3D imaging can improve LVEF reproducibility over 2D real-time techniques, where changes in slice positions during free-breathing may lead to differences in LVEF values. Initial results at 0.55T suggest this technique could be deployed on low-field scanners, potentially improving access to cardiac MRI in lower-resource settings. Future work will include validation in additional subjects, including patients with arrhythmias.Acknowledgements
Siemens Healthineers; NIH/NHLBI R01HL163030, R01HL153034, and R01HL163991References
1. Hargreaves B. Variable-Density Spiral Design Functions. 2005. http://mrsrl.stanford.edu/~brian/vdspiral/.2. Winkelmann S, Schaeffter T, Koehler T, Eggers H, Doessel O. An optimal radial profile order based on the Golden Ratio for time-resolved MRI. IEEE Trans Med Imaging. 2007;26(1):68-76. doi:10.1109/TMI.2006.885337.
3. Ulyanov D, Vedaldi A, Lempitsky V. Deep Image Prior. In: Proceedings of the IEEE Computer Society Conference on Computer Vision and Pattern Recognition. IEEE Computer Society; 2018:9446-9454.
4. Yoo J, Jin KH, Gupta H, Yerly J, Stuber M, Unser M. Time-Dependent Deep Image Prior for Dynamic MRI. IEEE Trans Med Imaging. 2021;40(12):3337-3348. doi:10.1109/TMI.2021.3084288
5. Fessler J, Sutton B. Nonuniform fast Fourier transforms using min-max interpolation. IEEE Trans Signal Process. 2003;51(2):560-574.
6. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet Lond Engl. 1986;1(8476):307-310.
Figures