1364
Time-dependent diffusion MRI-based microstructural mapping for preoperative prediction of intraductal component in invasive breast cancer1Department of Radiology, Sichuan Clinical Research Center for Cancer, Sichuan Cancer Hospital & Institute, Sichuan Cancer Center, Chengdu, China, 2MR Research Collaboration, Siemens Healthineers Ltd, Chengdu, China, 3Siemens Healthineers AG, Erlangen, Germany
Synopsis
Keywords: Microstructure, Quantitative Imaging
Motivation: Conventional MRI falls short in detecting specific imaging markers for an intraductal component(ductal carcinoma in situ) in invasive breast cancer (IBC-IC), thus affecting breast-conserving surgery. Advanced MRI techniques can help in preoperative evaluations.
Goal(s): We evaluated the efficacy of td-dMRI for preoperatively identifying IBC-IC for surgical planning.
Approach: We used td-dMRI to examine microstructural mapping in IBC patients by IMPULSED model, focusing on the parameters Dex, d, and vin to differentiate IBC-IC from IBC.
Results: We revealed that elevated d and Dex and reduced vin are distinct microstructural markers of IBC-IC, which might facilitate surgical planning for IBC-IC patients.
Impact: Parameters derived from td-dMRI have the potential to act as imaging biomarkers for distinguishing IBC-IC, thereby enhancing the precision of breast-conserving surgery planning.
Introduction
Breast cancer is the most commonly diagnosed cancer among women globally. The occurrence of an intraductal component (ductal carcinoma in situ) in invasive breast cancer (IBC-IC) is a common risk factor contributing to positive surgical margins1, re-operation rates2, and local-regional recurrence3 in breast conserving surgery. Traditionally, morphological features of breast tumors on magnetic resonance imaging (MRI) have been the only predictors of IBC-IC and are subject to visual interpretation and highly affected by the radiologist’s experience. Thus, MRI often falls short in accurately identifying specific imaging biomarkers of IBC-IC. More advanced techniques are needed to improve preoperative evaluations. Time-dependent diffusion MRI (td-dMRI) is a promising technology, offering detailed, non-invasive tumor microstructure imaging. Using a suitable model, such as imaging microstructural parameters using limited spectrally edited diffusion (IMPULSED) model, td-dMRI provides deeper insights into the cellular characteristics and composition of tumors4,5. This study was conducted to investigate the feasibility of td-dMRI in preoperatively predicting IBC-IC within IBC cases.Methods
MR imaging: This retrospective study included 34 women with IBC, aged 54.44 ± 13.01 years, who underwent td-dMRI on a 3T scanner (MAGNETOM Skyra, Siemens Healthineers, Erlangen, Germany) with a 16-channel breast array coil. The MRI protocol integrated oscillating gradient spin-echo (OGSE) and pulsed gradient spin-echo (PGSE) sequences from research sequence. OGSE operated at 40 Hz and 25 Hz, with effective diffusion times of 5.9 msec (b-values: 0, 150, 315 sec/mm2) and 9.7 msec (b-values: 0, 350, 710 sec/mm2), respectively. The PGSE sequence was applied with an effective diffusion time of 33.6 msec, with b-values of 0, 350, and 710 sec/mm2. Both sequences were harmonized to the following parameters: three diffusion directions, repetition time/echo time = 5000/132 ms, field of view = 220 × 220 mm2, in-plane resolution = 2.75 × 2.75 mm2, slices = 10, and section thickness = 5 mm. The total scanning time for this td-dMRI protocol was approximately 4.5 minutes. Post-contrast T1-weighted images were acquired for anatomical reference.Reconstruction & Segmentation: The estimation of IMPULSED parameters included extracellular diffusivity (Dex), volume-weighted mean cell size (d), intracellular volume fraction (vin), and cellularity. Intracellular diffusivity (Din) was set at 1.5 µm2/ms for stability6. Constraints were applied based on physiological plausibility: 0.2< d <25 μm, 0< vin <1, and 0< Dex <3.1 μm2/ms. Fitting was performed using the least square curve fitting toolbox in MATLAB (MathWorks, Inc.). In patients with IBC, the regions of interest in the tumor tissue were manually delineated on each slice based on td-dMRI after being aligned with the post-contrast T1-weighted images by an experienced radiologist (H.X. with 9 years of experience), excluding necrotic areas and surrounding tissue.
Statistical Analysis: An independent two sample t test and the Mann-Whitney U test were used to examine differences of IMPULSED parameters. Receiver operating characteristic (ROC) analysis and the corresponding area under the ROC curve (AUC) were used to assess the performance of each parameter in identifying IBC-IC.
Results
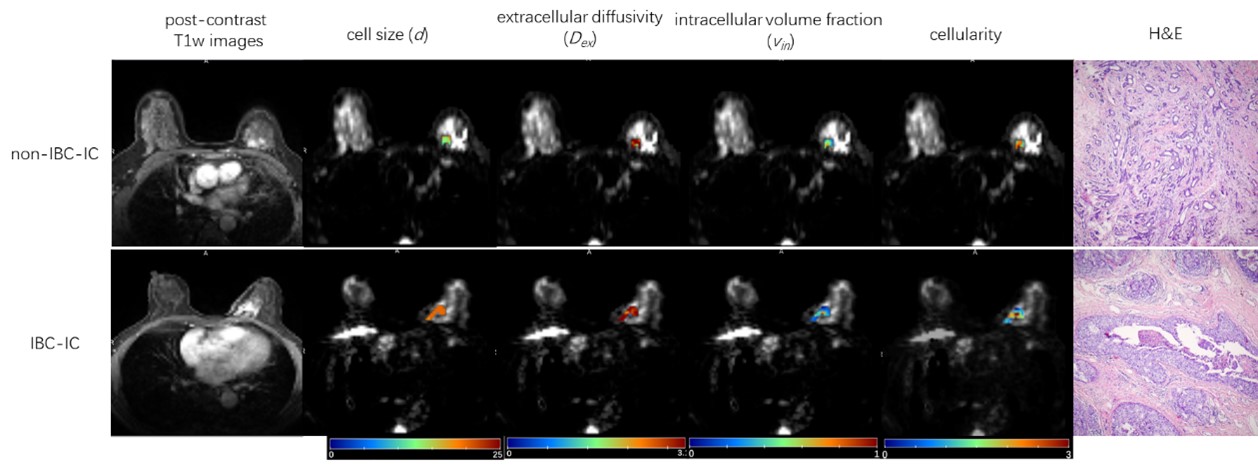
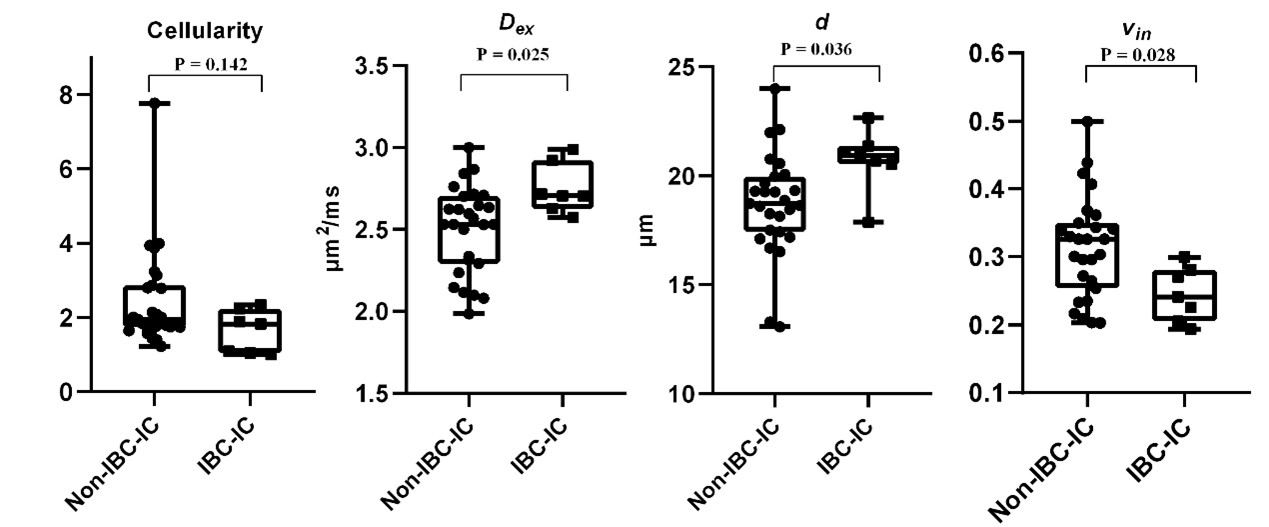
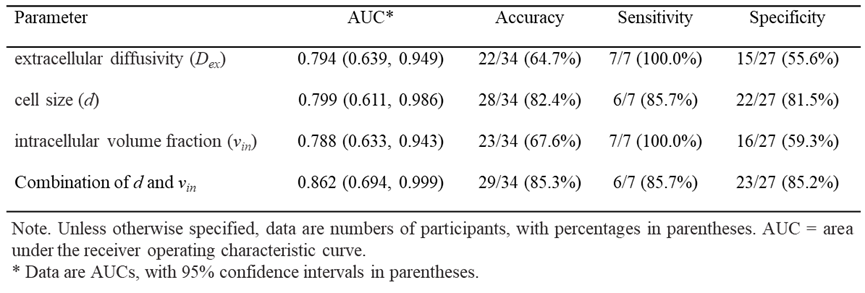
7 IBC-IC and 27 IBC patients were ultimately identified by histology. Figure 1 showed the microstructural mapping results using the td-dMRI in two representative cases. Compared with those of the non-IBC-IC group, d and Dex were significantly higher (P = 0.036 and 0.025), and vin was significantly lower (P = 0.028) in the IBC-IC group (Figure 2). Cellularity did not significantly differ between the groups (P = 0.142). For preoperatively predicting IBC-IC, the d index achieved the highest AUC of 0.799 among all parameters, while Dex and vin showed AUCs of 0.794 and 0.788, respectively. Combining d and vin further improved the AUC to 0.862 (Table 1 and Figure 3).Discussion
We found that the differential values of Dex, d, and vin were enabled to distinguish IBC-IC from non-IBC-IC cases. The significantly higher d and Dex in the IBC-IC group suggested alterations in the tumor microenvironment, possibly due to factors such as increased cell turnover, stromal changes, or heightened heterogeneity in cell sizes, which are characteristic of invasive ductal carcinoma. Conversely, the lower vin in the IBC-IC group might reflect a denser extracellular matrix or increased fibrosis, which was common in more aggressive tumors. These findings emphasized the potential of these microstructural markers in guiding surgical approaches.Conclusion
td-dMRI-based microstructural mapping showed a good ability to preoperatively predict IBC-IC, which might facilitate individualized surgical planning for patients with breast cancer before breast conserving surgery.Acknowledgements
This study was supported by the National Natural Science Foundation of China (grant number U21A20521).References
1.Van Deurzen CH. Predictors of surgical margin following breast-conserving surgery: a large population-based cohort study. Ann Surg Oncol. 2016;23:627-633.
2.Jeevan R, Cromwell DA, Trivella M, et al. Reoperation rates after breast conserving surgery for breast cancer among women in England: retrospective study of hospital episode statistics. BMJ. 2012;345:450.
3.Schnitt SJ, Harris JR. Evolution of breast-conserving therapy for localized breast cancer. J Clin Oncol. 2008;26:1395-1396.
4.Xu J, Jiang X, Li H, et al. Magnetic resonance imaging of mean cell size in human breast tumors. Magn Reson Med. 2020;83:2002-2014.
5.Ba R, Wang X, Zhang Z, et al. Diffusion-time dependent diffusion MRI: effect of diffusion-time on microstructural mapping and prediction of prognostic features in breast cancer. Eur Radiol. 2023;33:6226-6237.
6. Jiang X, Li H, Zhao P, et al. Early detection of treatment-induced mitotic arrest using temporal diffusion magnetic resonance spec-troscopy. Neoplasia. 2016;18:387–397.
Figures