1362
Intravoxel incoherent motion imaging with phase-cycled stimulated-echoes for simultaneous cardiac diffusion tensor and perfusion imaging1National Heart and Lung Institute, Imperial College London, London, United Kingdom, 2Royal Brompton and Harefield Hospitals, Guy’s and St Thomas’ NHS Foundation Trust, London, United Kingdom
Synopsis
Keywords: IVIM, Cardiovascular
Motivation: Intravoxel incoherent motion (IVIM) imaging can provide information about cardiac microstructure and microvascular perfusion from a single examination. Current spin-echo based approaches for cardiac IVIM suffer from low perfusion sensitivity.
Goal(s): We implemented a stimulated-echo (STEAM)-based method for cardiac IVIM and diffusion tensor imaging to enable accurate cardiac diffusion and perfusion imaging in vivo in the human heart.
Approach: We introduced a novel IVIM-STEAM sequence incorporating phase cycling to obtain true b=0 s/mm2 images.
Results: We tested the feasibility of our approach in 9 healthy subjects and obtained homogeneous perfusion and diffusion tensor maps, with values in the range described in the literature.
Impact: Phase-cycled IVIM-STEAM provides good quality images that enable reliable fitting of cardiac diffusion tensor and perfusion parameters in healthy subjects. This approach may identify areas of microstructural aberration and perfusion abnormalities in patients with cardiovascular disease without exogenous contrast agents.
Introduction
The intravoxel incoherent motion (IVIM) framework has shown potential for the simultaneous characterization of myocardial microstructure and microvascular perfusion in the human heart, from a single scan and without the need for exogenous contrast agents1,2. IVIM models perfusion as a pseudo-diffusion process, resulting in an additional mono-exponential decay of the MR signal with increasing diffusion weighting. Considering both compartments, the overall IVIM signal model for data acquired with diffusion encoding strength b, S(b), can be described as:$$S(b)/S_0 = f exp(-bD^*)+(1-f)exp(-bD)$$
with S0 the unweighted image, f the perfusion fraction, D the diffusion coefficient, and D* the perfusion coefficient3.
Recent studies have shown that in the heart, stimulated echo-based IVIM (IVIM-STEAM) has a higher sensitivity to changes in microvascular perfusion than spin-echo based IVIM4,5. However, IVIM-STEAM has so far only been applied in small pre-clinical studies4,6. In this work we present for the first time the application of the IVIM-STEAM framework to the live human heart.
Methods
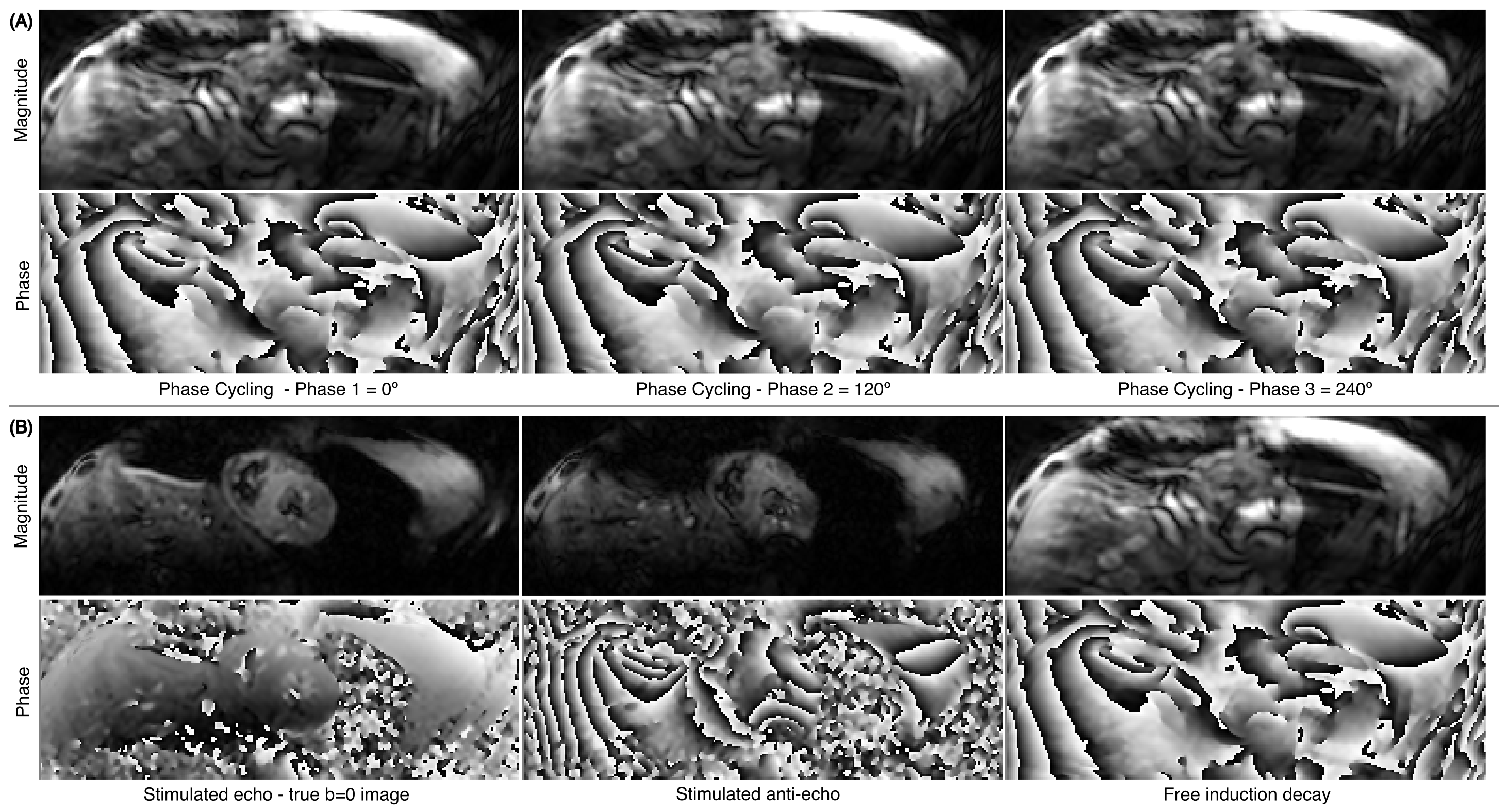
We implemented IVIM-STEAM on a 3T scanner (MAGNETOM Vida, Siemens) using an ECG-triggered stimulated-echo single-shot echo-planar diffusion tensor (DT) imaging sequence. At low b-values, the stimulated echo is mixed with residual stimulated anti-echo and free induction decay components7. To acquire true b=0 STEAM images, a 3-point phase cycling scheme (0/120/240°) of the second 90° pulse was implemented to enable isolation of the stimulated echo6 (Fig1), and an additional fat saturation pulse was used to further suppress the fat signal from the free induction decay which is not nulled in the phase cycling.To fit the perfusion and diffusion coefficients, we considered two fitting algorithms:
(1) Segmented-Unconstrained (SU), which is the most frequently used fitting algorithm in IVIM8. Based on the assumption that $$$D^*\gg D$$$, the perfusion component $$$f exp(-bD^*)$$$ is negligible at high b-values. Therefore, D can be obtained by fitting data acquired with b>bsplit to a mono-exponential decay, with bsplit a pre-defined threshold. Subsequently, f and D* can be obtained by fitting the acquired data to Eq.1, with known D.
(2) Segmented-Constrained (SC). Similar to SU, this algorithm fits the data acquired with b>bsplit to a mono-exponential decay, but obtains estimates of both D and f. In the second step, only D* is estimated by fitting the acquired data to Eq.1, with known D and f.
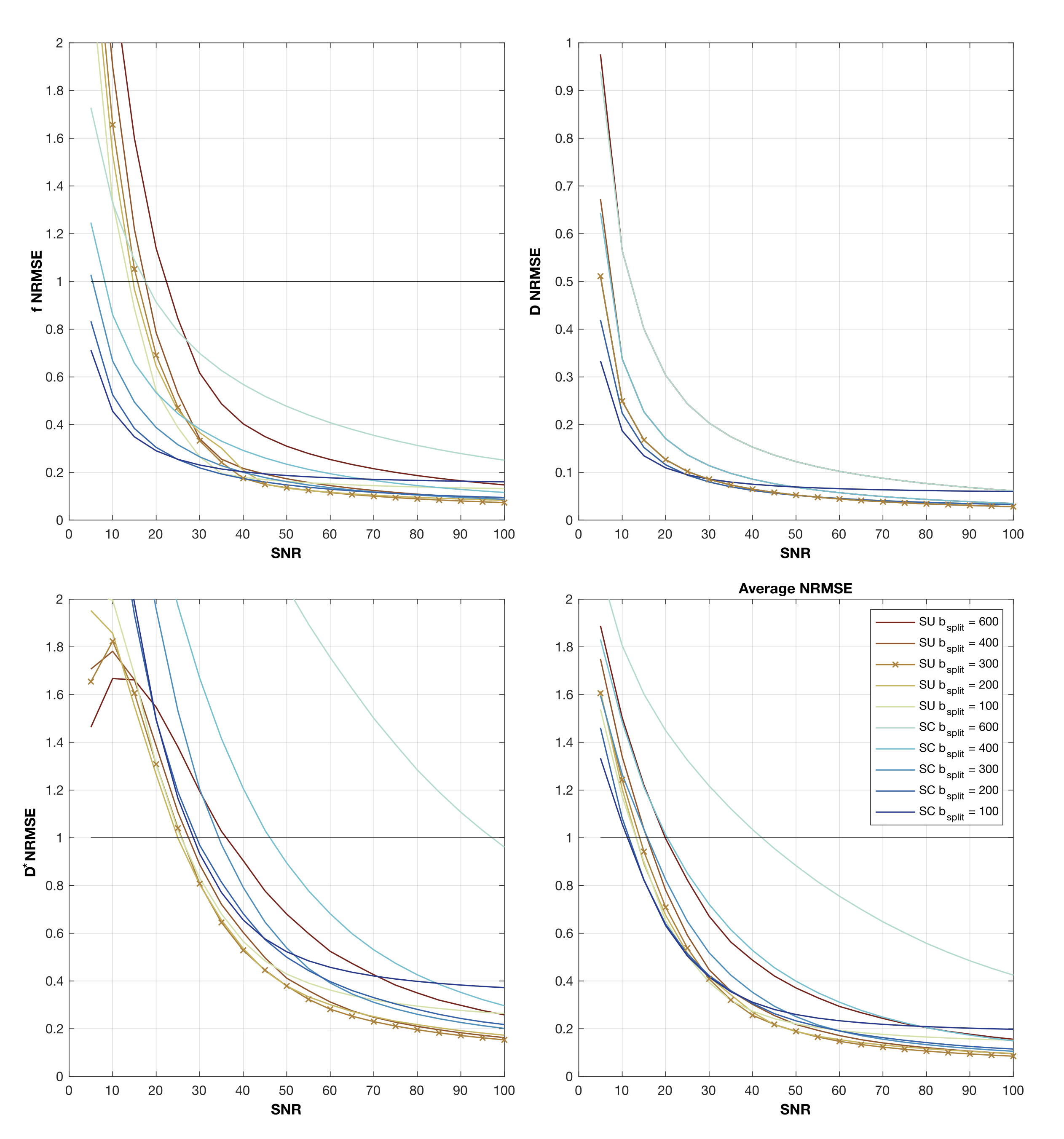
Simulations at different signal-to-noise ratio (SNR) levels (5 to 100) were performed to find the optimal bsplit and fitting algorithm, for tissue parameters in the following range: f:{10-25}%, D:{0.75-1.5}×10-3 mm/s2, D*:{10-25}×10-3mm/s2. Normalized root-mean square error (NRMSE) was computed to compare the performance of the different fitting algorithms. The optimal algorithm was then used for the in vivo experiments.
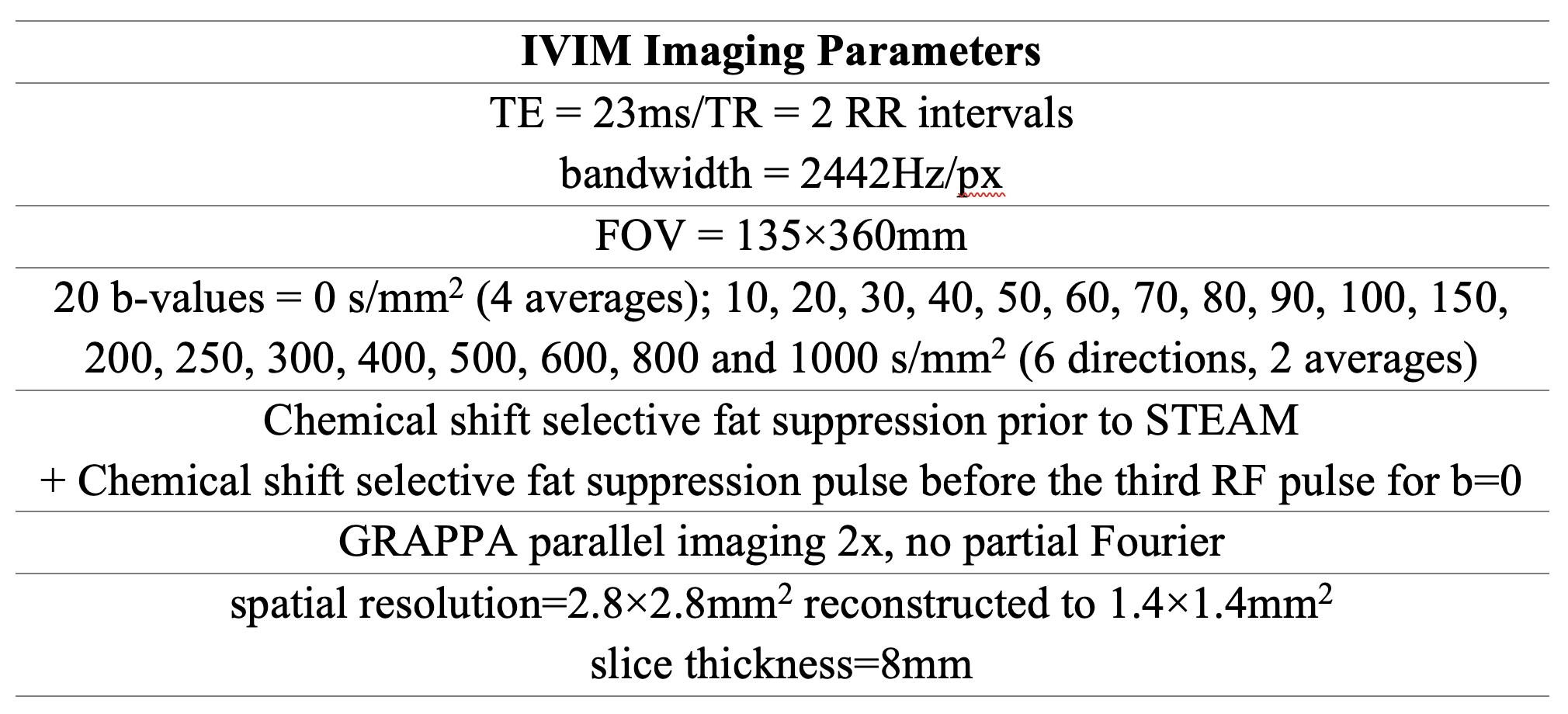
Nine healthy subjects (6 female, 33±10 years old) were scanned with the proposed IVIM-STEAM approach. bSSFP cine images were used to identify a mid-ventricular short-axis plane and the peak-systolic trigger delay for IVIM-STEAM imaging. Table 1 shows relevant imaging parameters. Note that 6 encoding directions were acquired for b>0, allowing for reconstruction of the DT.
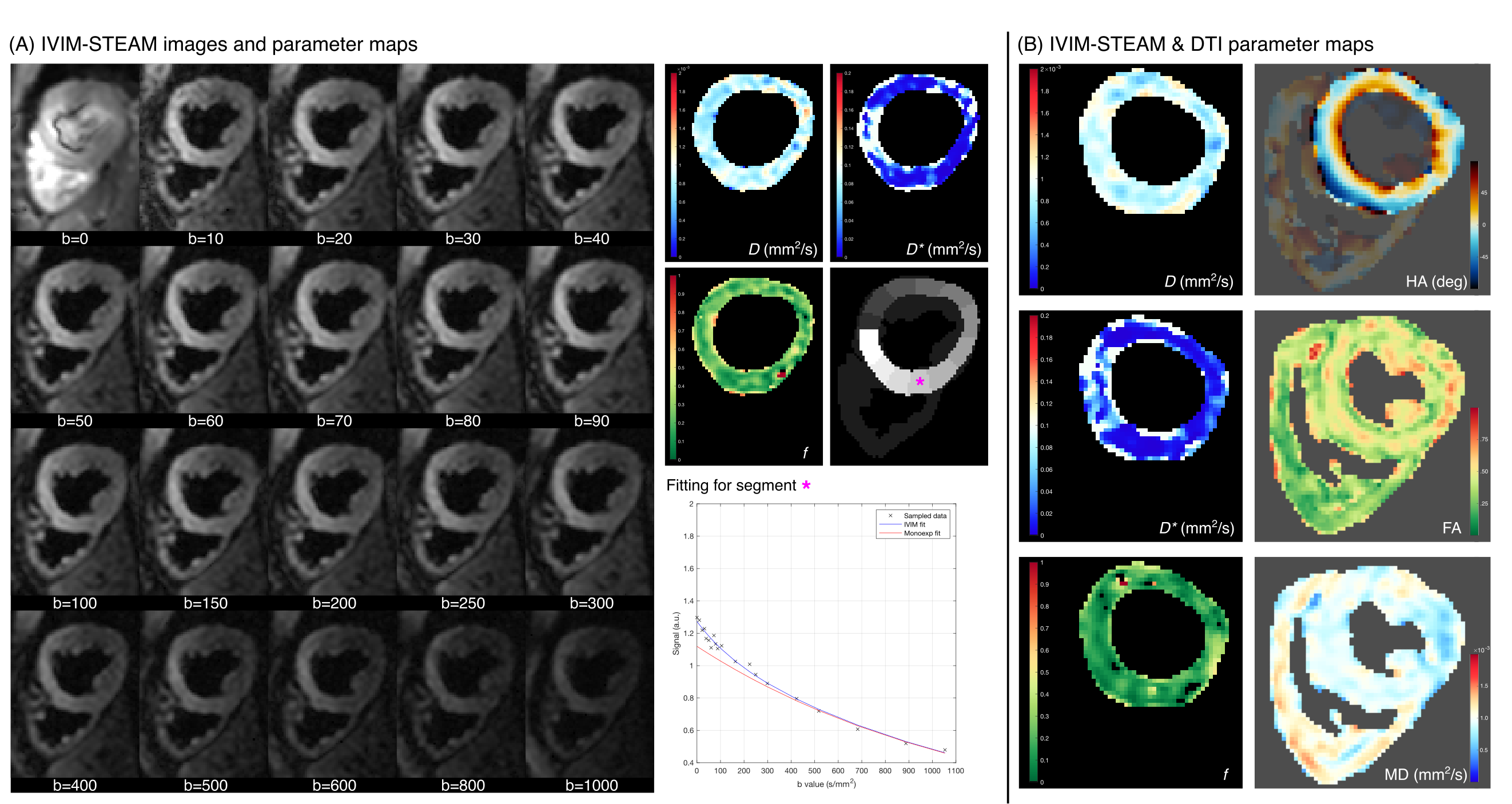
In post-processing, non-rigid image registration was performed to align images, and signal intensities S(b) were fitted to the IVIM model using a SU approach with bsplit=300s/mm2. Fitting was performed in a pixel-wise manner. As a proof of concept, we also fitted a DT model to data acquired with b>150s/mm2 for one representative subject.
Results
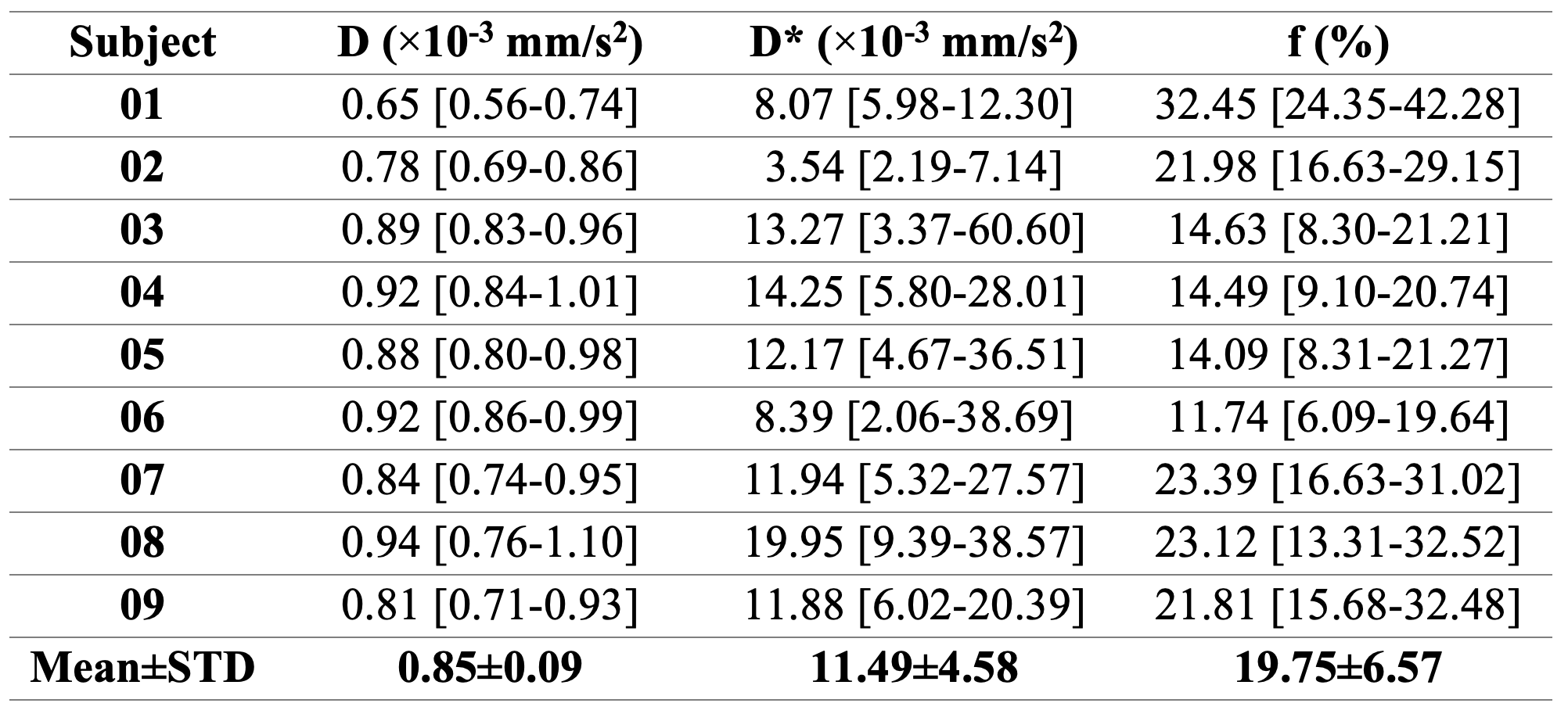
Simulations show that while the optimal fitting algorithm and choice of bsplit varies with SNR level and parameter of interest, overall, the SU algorithm with bsplit=300s/mm2 outperforms the other options for SNR>30 (Fig2).In vivo, IVIM-STEAM with phase cycling for b=0 resulted in good image quality for b-values ranging from 0 to 1000s/mm2 and corresponding D, D* and f maps showed generally consistent values across the myocardium (Fig3A). A segment-based fitting illustrates the difference in fitting accuracy between conventional mono-exponential fitting models and the IVIM model fitting, particularly at low b-values. Table 2 shows summary results for all subjects, with values within the range of those reported from pre-clinical data in the literature4,6. Fig3B shows both the IVIM model fitting (left column) and typical DT-CMR parameters (right column) for a representative subject, showing that the proposed approach also enables good quality estimation of tensor parameters.
Conclusion
The proposed IVIM-STEAM with phase cycling provides good quality b=0 images and shows potential for the simultaneous assessment of cardiac perfusion and microstructure from a single scan. We have demonstrated that DT-CMR results can be obtained from the STEAM-IVIM data in addition to perfusion parameters and future work will investigate the ability to detect areas of microstructural derangement and perfusion abnormalities in patients with cardiovascular disease.Acknowledgements
This work was supported by the BHF programme grant RG/19/1/34160 and the Engineering and Physical Sciences Research Council [grant number EP/X014010/1].References
[1] Delattre, B. M. A., et al. (2012). In Vivo cardiac diffusion-weighted magnetic resonance imaging: Quantification of normal perfusion and diffusion coefficients with intravoxel incoherent motion imaging. Investigative Radiology, 47(11), 662–670.
[2] Spinner, G. R., et al. (2017). Bayesian intravoxel incoherent motion parameter mapping in the human heart. Journal of Cardiovascular Magnetic Resonance, 19(1), 1–14.
[3] Le Bihan, D. (2019). What can we see with IVIM MRI? NeuroImage, 187, 56–67
[4] Spinner, G.R., et al. (2019). On probing intravoxel incoherent motion in the heart-spin-echo versus stimulated-echo DWI. Magnetic Resonance in Medicine, 82(3), 1150–1163.
[5] Alemany, I., et al. (2023). Realistic numerical simulations of diffusion tensor cardiovascular magnetic resonance: The effects of perfusion and membrane permeability. Magnetic Resonance in Medicine. https://doi.org/10.1002/mrm.29737
[6] Callot, V., et al. (2003). In vivo study of microcirculation in canine myocardium using the IVIM method. Magnetic Resonance in Medicine, 50(3), 531–540.
[7] Zhu, J.-M., & Smith, I. C. P. (1999). Stimulated Anti-Echo Selection in Spatially Localized NMR Spectroscopy. Journal of Magnetic Resonance, 136(1), 1–5
[8] Barbieri, S., et al C. (2016). Impact of the calculation algorithm on biexponential fitting of diffusion-weighted MRI in upper abdominal organs. Magnetic Resonance in Medicine, 75(5), 2175–2184.
Figures