1356
Discrimination Between Malignant and Healthy Breast Tissue Using Restriction Spectrum Imaging and MultiBand in a Screening Population1Radiology, UCSD, San Diego, CA, United States, 2Radiation oncology, UCSD, San Diego, CA, United States, 3Bioengineering, UCSD, San Diego, CA, United States, 4Global MR Application and Workflow, GE Healthcare, Boston, MA, United States
Synopsis
Keywords: Breast, Breast, Diffusion, RSI
Motivation: Diffusion weighted imaging (DW-MRI) holds great potential in improving specificity of findings detected on contrast enhanced breast MRI. A breast-specific Restriction spectrum imaging (BS-RSI) has been developed and proved to be able to discriminate cancers from benign lesions and healthy breast tissue.
Goal(s): To evaluate BS-RSI’s performance in differentiating malignant from healthy fibroglandular tissue in a breast cancer screening dataset (BCS).
Approach: We prospectively scanned 14 BCS patients with high-resolution multishell DWI added to standard BCS clinical protocol.
Results: The BS-RSI model was able to discriminate healthy tissue from cancers in all C-compartments.
Impact: Differences were observed between healthy tissue and malignant lesions in all C-compartments (p<0.01). ADC values were also significantly different in cancers than in healthy issue (p=0.044).
Introduction
Diffusion Weighted- (DW-) MRI is now part of breast cancer screening (BCS) protocol for high-risk population1. DW-MRI provides insight on tissue cellularity and advanced models can help discriminate cancers from healthy fibroglandular tissue, such as Restriction Spectrum Imaging (RSI)2.A breast-specific RSI (BS-RSI) model has been developed on a population of large known cancers and allows discrimination between cancers and benign lesions and from healthy breast tissue3, 4. Moreover, it has proven capable of assessing neoadjuvant chemotherapy (NAC) response in patients5. The BS-RSI model aims at separating signal in pools of different diffusion types (restricted, hindered, and free) and requires using time consuming high b-values (>2000 s/mm2). This constraint, plus the large FOV in the z-direction required to cover the whole breasts for efficient screening, forces using thick slices (4-6mm) which are suboptimal for cancer screening.
A promising solution to reduce slice thickness without increasing scanning time is using simultaneous multi-slice excitation (SMS or MultiBand – MB). This technique allows for a greater number of collected slices in the same amount of time, potentially enabling high-resolution multishell DWI for RSI. However, achieving high-resolution in DW-MRI, and even more at high-b-values, is challenging due to high noise levels.
In this study, we applied MB DW-MRI for RSI in a BCS population. We aimed to assess the performances of the BS-RSI model in discriminating cancers from healthy breast fibroglandular tissue.
Methods
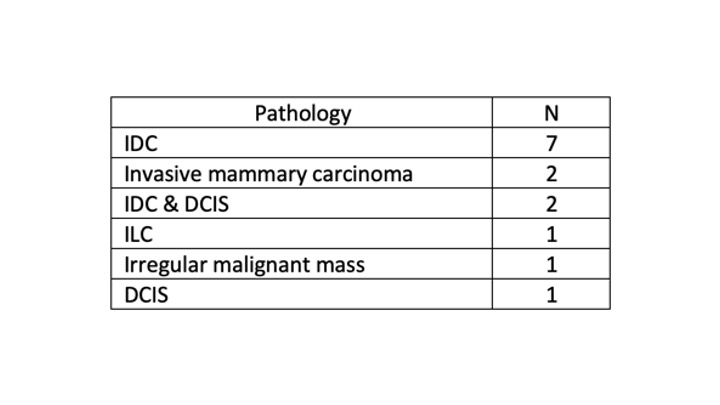
Images were prospectively collected at a single institution on a total of 14 patients undergoing routine screening MRI due to high-risk status. Pathology summary is reported in Table 1. All pathologies were assessed via core-needle biopsy.Images were following standard BCS protocol, including sequences and parameters: CUBE T2: TR/TE: 2500/91, FOV: 340x340, Matrix: 388x388, slices 94, Resolution: 0.88x088, Acq time: 2min 41s. High-resolution Multiband RSI: TR/TE: 9000/7906, FOV: 340x340, Matrix: 170x170, 90 slices, Resolution: 2.0x2.0x2.0, b-values (n directions) (s/mm2): 0 (1), 800 (6), 1500 (6), 3000 (6*2 Nex), Acq time, 3min 54s.
Images were distortion corrected using Reverse Polarity Gradient6, eddy current and noise corrected. Finally, images were normalized by the 98th percentile before being fitted into the BS-RSI model:
$$S(b) = C_1 + C_{2}e^{-b×1.4×10^{-3}} + C_{3}e^{-b×10.3×10^{-3}}$$
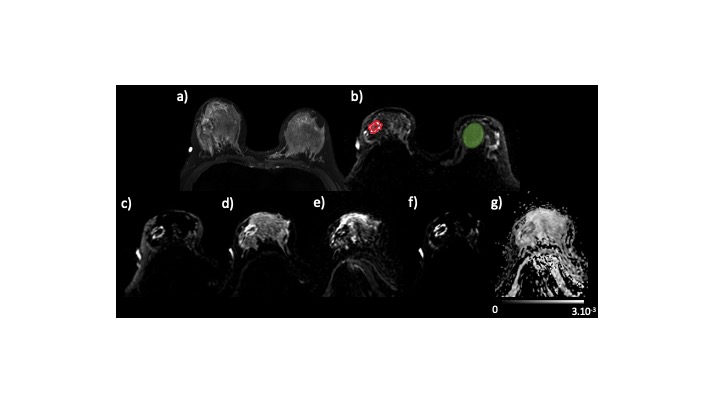
The outputs are hypothesized to correspond to cancer and fatty tissue (C1), fibroglandular tissue (C2), and vascular flow (C3). The product C1C2 has been reported to improve discrimination between cancer and healthy breast tissue, so it was estimated as well. In addition, ADC maps were computed using b = 0 and 800 s/mm2. ROIs were delineated on Osirix under the supervision of an expert radiologist on post-processed b = 1500 s/mm2 images (Figure 1b). Cancer ROIs were drawn on a single slice where the lesion appeared the largest. Control ROIs were drawn on the same slice in the contralateral breast, including as much healthy breast tissue as possible and avoiding any other lesion or cyst. Statistical analysis was performed using SPSS (IBM, USA). Differences in each C-component, as well as in ADC values, were evaluated pairwise among groups, and significances were assessed using two-sided t-tests.
Results
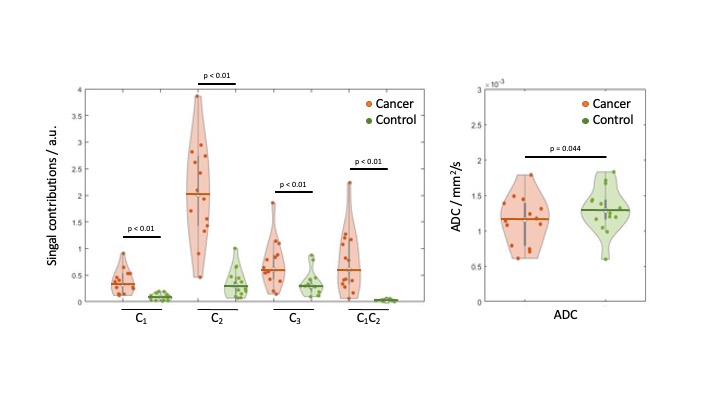
A total of 14 cancer lesions were identified in 14 BCS patients. After fitting the pre-processed reduced-FOV DW-MRI data to the breast-specific RSI model, we quantified median signal from cancer lesions and control ROIs in the RSI outputs. An example case of IDC is shown in Figure 1.We found that RSI signal compartment C1 was higher (p<0.01) in cancer than in fibroglandular tissue, while C2 was higher (p<0.01) in cancer compared to fibroglandular tissue. Interestingly, C3 was higher (p<0.01) in cancer lesions than in control ROIs (Figure 2). C1C2 was also higher in cancers than in healthy tissue (p<0.01), while ADCs were significantly lower in cancers than in healthy tissue (1.14.10-3 vs 1.3.10-3, p=0.044)
Discussion
In this study we evaluate the performance of the BS-RSI model on a BCS dataset when used with high-resolution DWI. The BS-RSI enabled discriminating cancer lesions from healthy breast tissue in every C-compartment. The ADC values obtained with b0 and b800 from the BS-RSI model acquisition were also consistent with literature7, though groups had only slightly different distributions (p=0.044).Next steps of the study focus on including more BCS patients. A major challenge in BCS is discriminating high-risk benign lesion from average-risk benign lesion, and BCS would highly benefit from a robust model improving specificity, reducing unnecessary biopsies.
In addition, the BS-RSI fixed ADCs should be re-calculated when a larger dataset is available to estimate its reproducibility and accuracy.
Acknowledgements
GE Healthcare Research Grant
Krueger Wyeth Award
References
1. Lee CH, Dershaw DD, Kopans D, et al. Breast Cancer Screening With Imaging: Recommendations From the Society of Breast Imaging and the ACR on the Use of Mammography, Breast MRI, Breast Ultrasound, and Other Technologies for the Detection of Clinically Occult Breast Cancer. J Am Coll Radiol. 2010;7(1):18-27. doi:10.1016/j.jacr.2009.09.022
2. White NS, Leergaard TB, D’Arceuil H, Bjaalie JG, Dale AM. Probing tissue microstructure with restriction spectrum imaging: Histological and theoretical validation. Hum Brain Mapp. 2013;34(2):327-346. doi:10.1002/hbm.21454
3. Rodríguez-Soto AE, Andreassen MMS, Fang LK, et al. Characterization of the diffusion signal of breast tissues using multi-exponential models. Magn Reson Med. 2022;87(4):1938-1951. doi:10.1002/mrm.29090
4. Besser AH, Fang LK, Tong MW, et al. Tri-Compartmental Restriction Spectrum Imaging Breast Model Distinguishes Malignant Lesions from Benign Lesions and Healthy Tissue on Diffusion-Weighted Imaging. Cancers. 2022;14(13):3200. doi:10.3390/cancers14133200
5. Andreassen MMS, Rodríguez-Soto AE, Conlin CC, et al. Discrimination of Breast Cancer from Healthy Breast Tissue Using a Three-component Diffusion-weighted MRI Model. Clin Cancer Res. 2021;27(4):1094-1104. doi:10.1158/1078-0432.CCR-20-2017
6. Rodríguez-Soto AE, Fang LK, Holland D, et al. Correction of Artifacts Induced by B0 Inhomogeneities in Breast MRI Using Reduced-Field-of-View Echo-Planar Imaging and Enhanced Reversed Polarity Gradient Method. J Magn Reson Imaging. 2021;53(5):1581-1591. doi:10.1002/jmri.27566
7. Baltzer P, Mann RM, Iima M, et al. Diffusion-weighted imaging of the breast—a consensus and mission statement from the EUSOBI International Breast Diffusion-Weighted Imaging working group. Eur Radiol. 2020;30(3):1436. doi:10.1007/s00330-019-06510-3
Figures