1354
Depicting ability of 7 Tesla MRA for lenticulostriate arteries: practical assessment based on intraoperative video of aneurysm neck clipping1Department of Neurosurgery, Iwate Medical University School of Medicine, Shiwa, Japan, 2Division of Ultrahigh Field MRI, Institute for Biomedical Sciences, Iwate Medical University School of Medicine, Shiwa, Japan
Synopsis
Keywords: Blood Vessels, Neuro
Motivation: To clear the depicting ability for the lenticulostriate arteries at 7 Tesla in patients with unruptured the middle cerebral artery aneurysm.
Goal(s): MRA at 7 Tesla can depict the lenticulostriate arteries more than that at 3 Tesla in assessment using the intraoperative video.
Approach: Comparison of accuracy of identification of LSAs at standard 3D TOF imaging at 3T, standard 3D TOF imaging at 7Tand high-resolution 3D TOF at 7T, using the findings of intraoperative video as the reference.
Results: LSAs were identified more accurately by HR7T 3D TOF than by S3T 3D TOF.
Impact: In patients with an unruptured MCA aneurysm, LSAs were identified more accurately by HR7T 3D TOF than by S3T 3D TOF; however, the ability to depict the vessels could depend on the resolution rather than the signal-to-noise ratio.
Introduction
Some studies have reported that compared with MRA at 3 Tesla (T), time-of flight (TOF) MRA at 7 T could clearly delineate microvessels including the LSAs, and that the ability of 7 T TOF MRA to depict the LSAs was comparable to that of digital subtraction angiography 1,2. 7 T TOF MRA studies conducted quantitative assessment1,3 but these studies did not compare the MRA data with the intraoperative findings. Therefore, the purpose of the present study was to clear depicting ability for LSAs at 7 T in patients with unruptured MCA aneurysm, using the findings of intraoperative video of the neck clipping surgery as the reference.Methods
Patients who satisfied the following inclusion criteria were included in this prospective study: 1) unruptured intracranial aneurysm (UIA) located in the unilateral MCA as detected by MRA or CTA, 2) age 20–75 years, 3) modified Rankin Scale of 0 or 1, and 4) no obvious cognitive impairment. All patients underwent MRA with a 7T scanner (Discovery MR950; GE Healthcare, Milwaukee, WI, USA) using a 32-channel receive head coil. For comparison, MRA with a 3T MRI scanner (Discovery MR750, the same vendor) using an 8-channel receive head coil was also performed in each patient. Standard 3D TOF imaging at 7T (S7T) was performed with the following parameters: TR/TE = 15/2.9 ms, matrix = 512 × 320, slice thickness = 1 mm, field of view = 240 mm, and scan time = 7 min 35 s. High-resolution 3D TOF at 7T (HR7T) was performed with the following parameters: TR/TE = 14/2.3 ms, matrix = 1024 × 448, slice thickness = 0.6 mm, field of view = 240 mm, and scan time = 12 min 49 s. Standard 3D TOF imaging at 3T (S3T) was performed with the following parameters: TR/TE = 122/3.8 ms, matrix = 512 × 320, slice thickness = 1 mm, field of view = 240 mm, image size = 512 × 512, and scan time = 7 min 59 s. Zero-fill interpolation was performed for all images after each scan. In each patient, sequential maximum intensity projection (MIP) images were reconstructed from each 20-mm-thick 3D TOF dataset at intervals of 1 mm in the coronal direction parallel to the horizontal portion of each MCA that had a UIA. Two independent neuroradiologists visually identified LSAs branching from the horizontal portion of the MCA that had a UIA on the MIP and axial source images, and counted the number of LSAs in each TOF dataset (NTOF). On video that was recorded intraoperatively, LSAs branching from the horizontal portion of each MCA with a UIA (Nv) were visually identified by two experienced neurosurgeons, who checked the same video recordings cooperatively. The number of LSAs on each patient’s 2D video (NV) was counted and the diameter of each LSA was measured. The estimated diameter of the determined LSA was defined as the TOF-visible diameter. Finally, the incidence of patients with NTOF / NV = 100% was calculated for each of S3T 3D TOF, S7T 3D TOF, and HR7T 3D TOF.Results
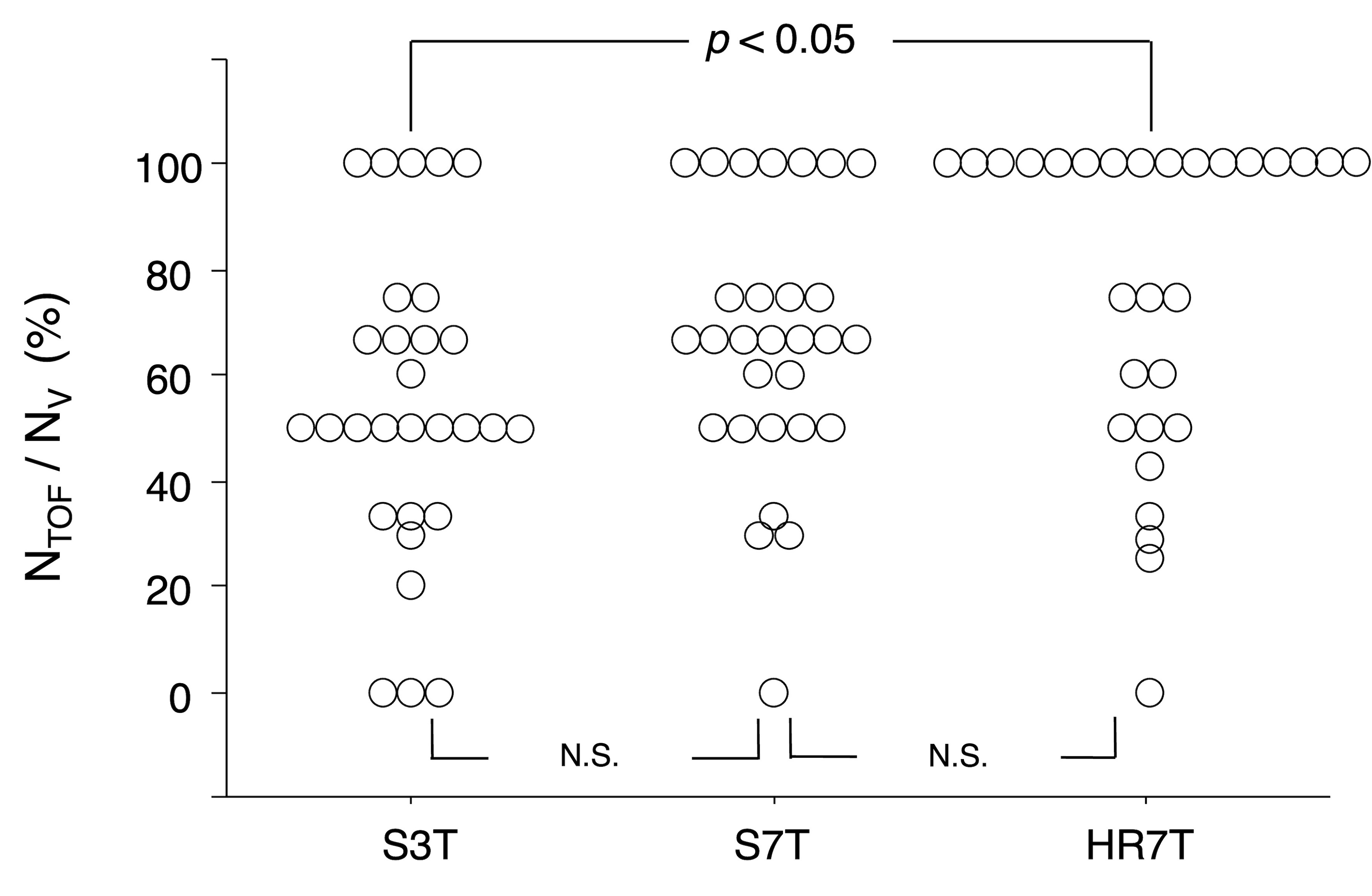
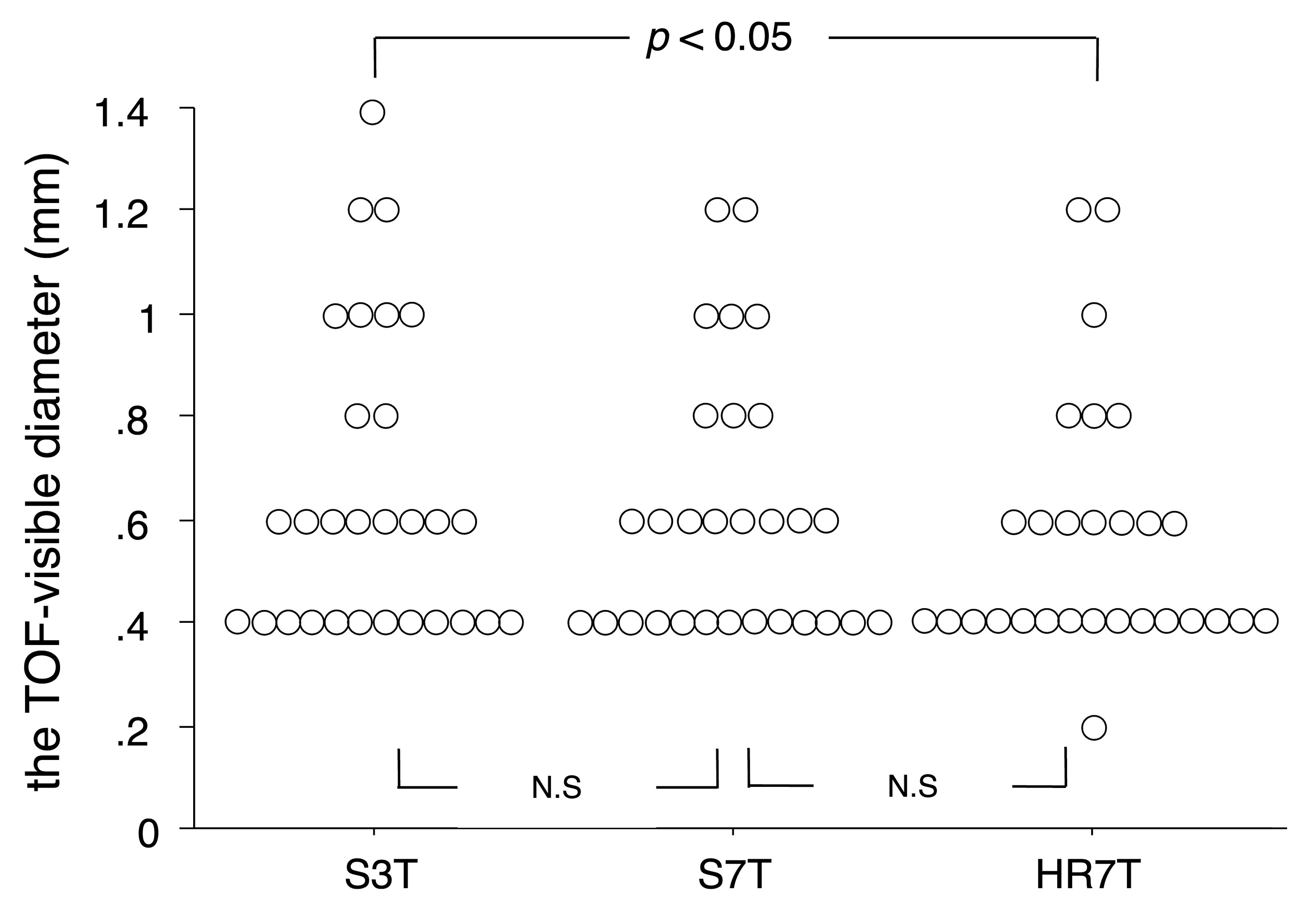
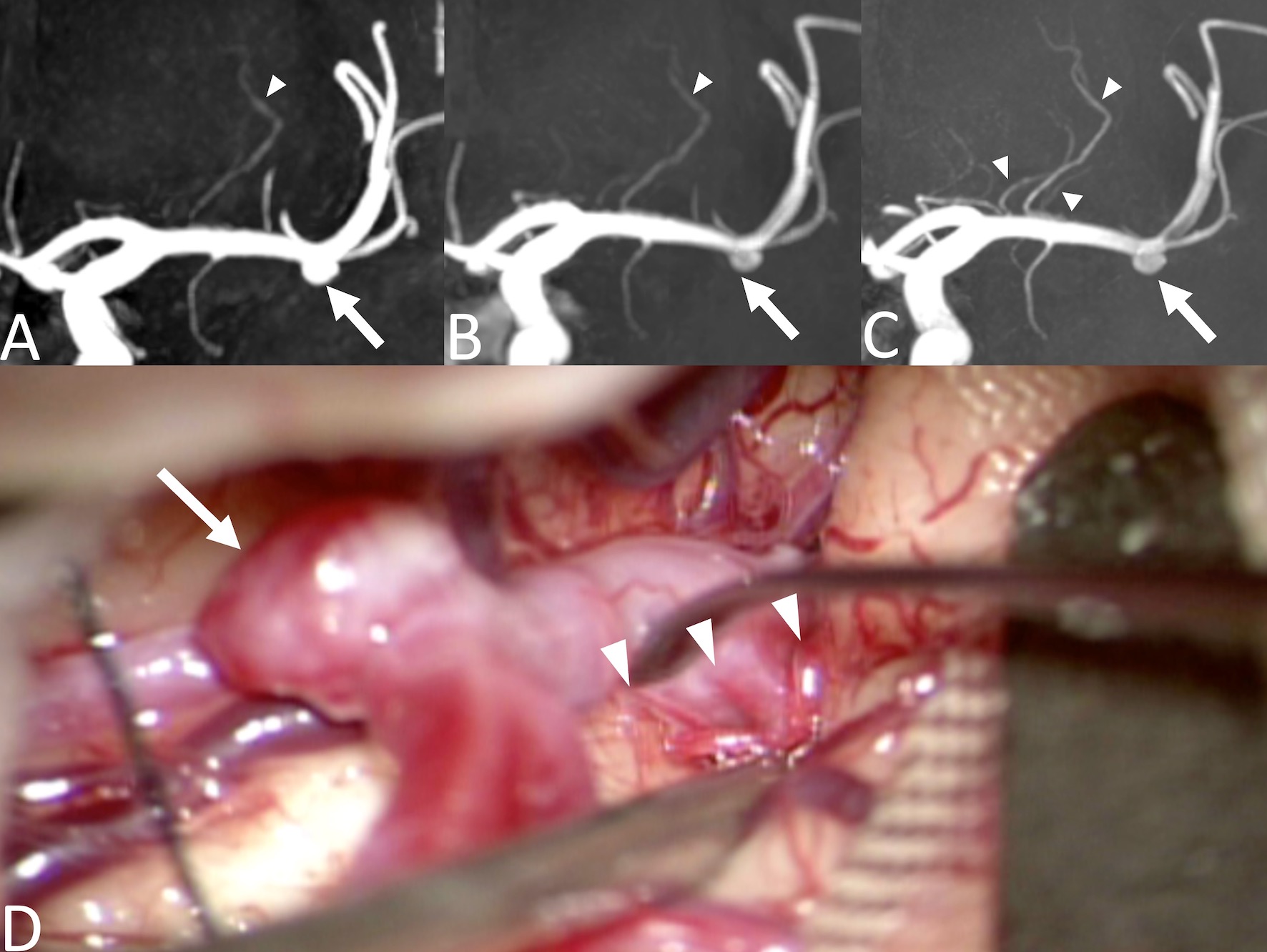
A final total of 29 patients (median age, 64 years; 21 women) successfully underwent neck clipping through craniotomy under general anesthesia and were included in the study. NTOF / NV was 50% for S3T 3D TOF, 66.7% for S7T 3D TOF, and 100% for HR7T 3D TOF; and was greater on HR7T 3D TOF than on S3T 3D TOF (p < 0.05) (Fig. 1). The percentage of patients with NTOF / NV = 100% was significantly higher on HR7T 3D TOF (55%) than on S3T 3D TOF (17%) (p < 0.05/3 = 0.017). Median TOF-visible diameter was 0.6 mm for S3T 3D TOF, 0.6 mm for S7T 3D TOF, and 0.4 mm for HR7T 3D TOF; and was significantly smaller on HR7T 3D TOF than on S3T 3D TOF (p < 0.05) (Fig. 2).Representative 3D TOF images and 2D intraoperative video in a patient with a left MCA aneurysm are shown in Fig. 3.Discussion
We observed the significant difference in identification accuracy for LSAs between S3T 3D TOF and HR7T 3D TOF, but between S3T 3D TOF and S7T 3D TOF. This finding suggests that the ability to depict the vessels could depend on the resolution adjusted by voxel size rather than signal-to-noise ratio.Conclusion
LSAs in patients with an unruptured MCA aneurysm were identified more accurately by HR7T 3D TOF than by S3T 3D TOF.Acknowledgements
NoneReferences
1. Cho ZH, Lee YB, Kang CK, et al. Microvascular imaging of asymptomatic MCA steno-occlusive patients using ultra-high-field 7T MRI. J Neurol. 2013;260:144-50.
2. Lee YB, Kang CK, Kim KT, et al. A non-invasive technique for visualization of microvessels in asymptomatic patients with middle cerebral artery steno-occlusion. Vasc Med. 2013;18:314-7.
3. Miyazawa H, Natori T, Kameda H, et al. Detecting lenticulostriate artery lesions in patients with acute ischemic stroke using high-resolution MRA at 7 T. Int J Stroke. 2019;14:290-297.
Figures