1352
Cerebral Blood Flow Pulsatility Predicts the Cerebral Hyperperfusion Syndrome after direct revascularization surgery—A pilot study1Radiology, Sichuan Provincial People's Hospital, Chengdu, China, 2Neurosurgery, Sichuan Provincial People's Hospital, Chengdu, China
Synopsis
Keywords: Blood Vessels, Blood vessels, 4D flow, cerebral hyperperfusion syndrome
Motivation: Little is known about cerebral hemodynamics after bypass surgery in patients with chronic arterial stenosis (CAS) and its role in the development of cerebral hyperperfusion syndrome (CHS).
Goal(s): The purpose of this study was to explore the hemodynamic characteristics of patients with CAS and occlusion before and after surgery and its relationship with CHS.
Approach: We used 4D flow MRI sequence to obtain the hemodynamic characteristics of patients with CAS and occlusion before and after bypass surgery.
Results: Postoperative total cerebral blood flow increased and resistance index and pulsatility index decreased maybe a higher risk factor of CHS events in bypass surgery patients.
Impact: This study provides a new insight into the hemodynamic characteristics of patients with chronic arterial stenosis, and holds a promising marker for marker for identifying CHS patients.
Introduction
Cerebral hyperperfusion syndrome (CHS) is one of the most serious complications after superficial temporal artery-middle cerebral artery (STA-MCA) bypass surgery. It is manifested as focal nerve defect, cerebral hemorrhage, epilepsy, etc. In severe cases, it can be fatal. Finding non-invasive tests to assess the risk of complications can help clinical early intervention in time 1.Non-contrast 4D flow MRI has recently been used to evaluate cerebrovascular hemodynamics, because it can accurately measure intracranial arterial flow, even in the case of hemodynamically significant stenosis 2. Although there have been studies suggesting that observing blood flow parameters in 4D flow may help improve vascular selection and provide more detailed postoperative evaluation in patients undergoing extracranial-to-intracranial bypass surgery 3, there have little reports on the estimation of possible postoperative complications by using 4D flow.This study aims to explore the hemodynamic characteristics of patients with chronic arterial stenosis and occlusion before and after surgery and its relationship with CHS.Methods
We recruited 15 patients undergoing STA-MCA bypass surgery for internal carotid artery stenosis (ICS), middle cerebral artery stenosis (MCS) caused by atherosclerotic diseases, and 5 of them reported suspected CHS reported by CT perfusion imaging or MRI perfusion imaging. The diagnostic criteria for CHS are the same as used by Fujimura et al 4. All patients underwent conventional head magnetic resonance scan, dynamic susceptibility contrast magnetic resonance scan and 4D flow magnetic resonance scan before and after surgery. 4D flow MRI was performed using a 3 T scanner (Vida, Siemens, Germany). The brief summary of 4D flow parameters was as follows: VENC =120 cm/s, voxel size = 1×1×1 mm3 isotropy, 15 cardiac phases, and acquisition time approximately 12 min. The MASS research software (MASS, Version 2019-EXP, Leiden University Medical Center, Leiden, The Netherlands) was used to obtain the blood flow and velocity of the internal carotid artery (ICA), anterior cerebral artery (ACA), middle cerebral artery (MCA), posterior cerebral artery (PCA), basilar artery (BA), and extracranial-to-intracranial bypass artery (Figure 1). The severe side of stenosis and occlusion was taken as the ipsilateral 5. The difference of cerebral blood flow in each bypass artery before and after surgery, and the difference of blood flow in the intracranial extracranial segment of the bypass artery were compared. The difference of cerebral blood flow in each bypass artery after surgery, the total cerebral blood flow, bypass artery flow resistance index (RI) and pulsatility index (PI) were compared between the non-cerebral hyperperfusion syndrome (N-CHS) group and the CHS group. For all analysis, P<0.05 was considered to be statistically significant.Results
As shown in Table 1, the total blood flow increased in the CHS group after surgery, and the P =0.099. The RI and PI values of bypass artery in CHS group are lower than that in N-CHS group, and the P values were 0.007 and 0.019, respectively. In addition, there was no significant difference between the extracranial segment and intracranial segment of bypass artery between the two groups, and the P values were 0.859 and 0.371, respectively. The blood flow of other vessels did not change significantly (Table 2).Discussion
In this study, we compared cerebral hemodynamics in patients who did not develop hyperperfusion syndrome after STA-MCA bypass with those who did. The results showed that the RI and PI values of STA-MCA bypass artery were significantly lower in the CHS group than in the N-CHS group (P< 0.05). However, there was no significant difference between the two groups in the comparison of the intracranial segment and the extracranial segment of the bypass artery. This suggests that the occurrence of CHS may be independent of blood flow. Generally, the decrease of PI and RI can directly reflect the decrease of cerebrovascular pulsation, the diastolic state of cerebrovascular, the decrease of downstream perfusion resistance, the high cerebral perfusion pressure or the impairment of cerebrovascular regulatory function 6-8.Conclusion
The visual and quantitative assessment of 4D flow MRI revealed that intracranial blood flow changes complementarily after STA-MCA bypass surgery. We initial data suggest that PI and RI values obtained by 4D flow may be a higher risk factor for CHS in STA-MCA bypass surgery patients.Acknowledgements
We are grateful to all the participants for their cooperation.References
1. Manojlovic V, Budakov N, Budinski S, et al. Cerebrovacular Reserve Predicts the Cerebral Hyperperfusion Syndrome After Carotid Endarterectomy. J Stroke Cerebrovasc Dis. 2020;29(12):105318.
2. Wahlin A, Eklund A, Malm J. 4D flow MRI hemodynamic biomarkers for cerebrovascular diseases. J Intern Med. 2022;291(2):115-127.
3. Callen AL, Caton MT, Rutledge C, et al. The Effect of Extracranial-to-Intracranial Bypass on Cerebral Vasoreactivity: A 4D Flow MRI Pilot Study. J Neuroimaging. 2020;30(5):587-592.
4. Fujimura M, Mugikura S, Kaneta T, et al. Incidence and risk factors for symptomatic cerebral hyperperfusion after superficial temporal artery-middle cerebral artery anastomosis in patients with moyamoya disease. Surg: Neurol. 2009;71(4):442–447,
5. Sekine T, Murai Y, Orita E, et al. Cross-Comparison of 4-Dimensional Flow Magnetic Resonance Imaging and Intraoperative Middle Cerebral Artery Pressure Measurements Before and After Superficial Temporal Artery-Middle Cerebral Artery Bypass Surgery. Neurosurgery. 2021;89(5):909-916.
6. Greene ER, Yonan KA, Sharrar JM, et al. Middle cerebral artery resistivity and pulsatility indices in systemic lupus erythematosus: evidence for hyperperfusion. Lupus. 2012;21(4):380-385.
7. Shakur SF, Amin-Hanjani S, Mostafa H, et al. Relationship of pulsatility and resistance indices to cerebral arteriovenous malformation angioarchitectural features and hemorrhage. J Clin Neurosci. 2016;33:119-123.
8. Ackerstaff RG, Moons KG, van de Vlasakker CJ, et al. Association of intraoperative transcranial doppler monitoring variables with stroke from carotid endarterectomy. Stroke. 2000; 31(8):1817–1823.
Figures
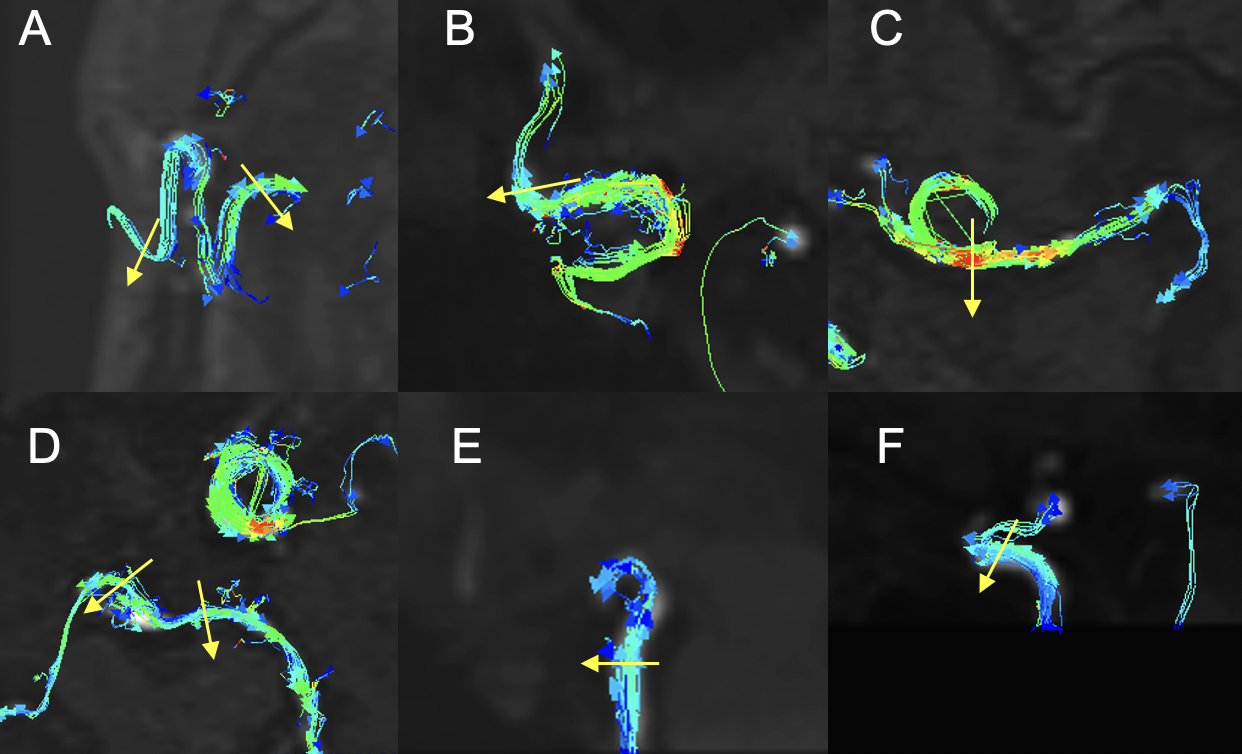
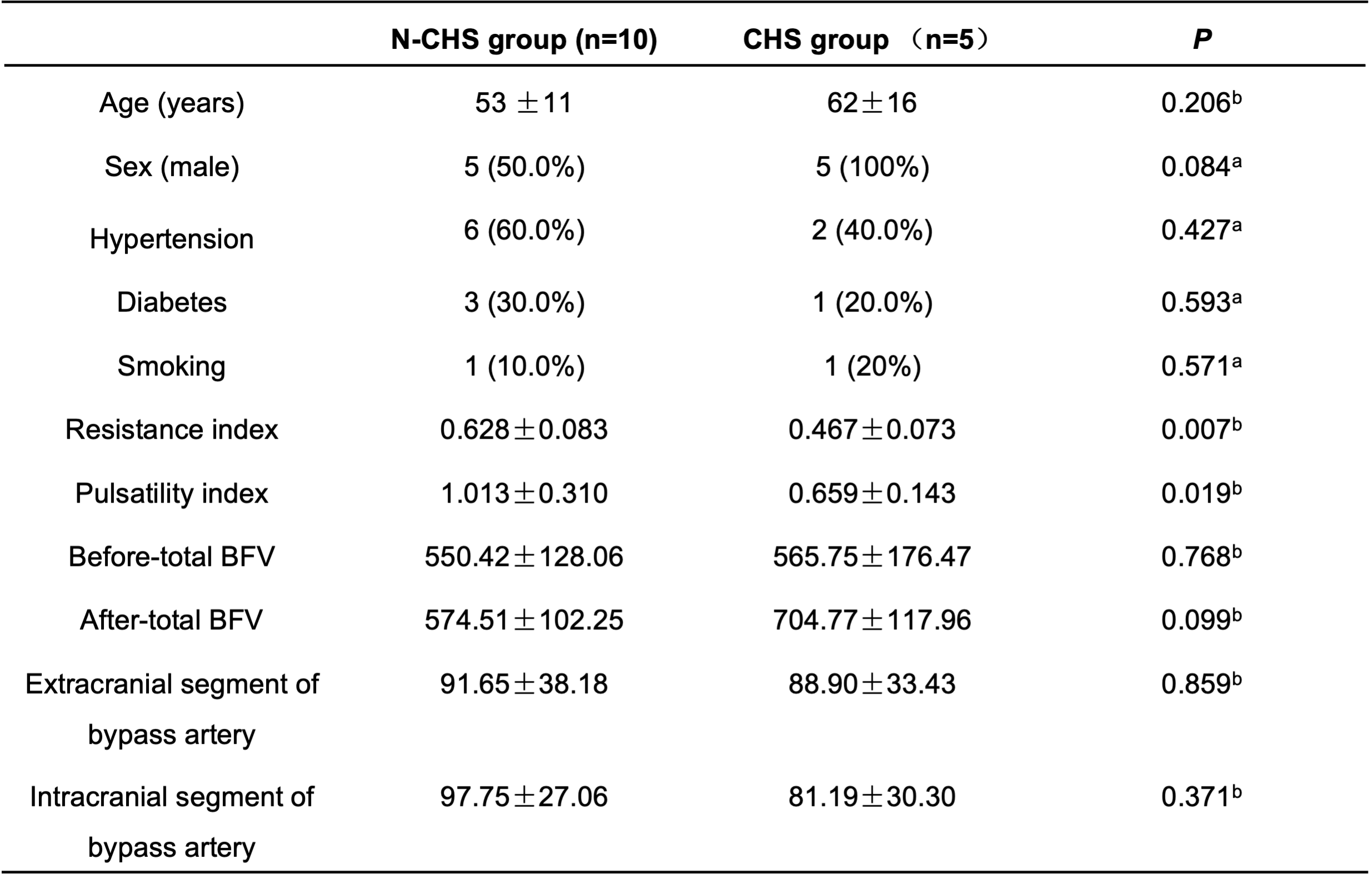
Table 1. Characteristics of participants with non-cerebral hyperperfusion syndrome and cerebral hyperperfusion syndrome.
Notes: Values are presented as mean ± standard deviation (SD) or number (%). a Chi-Squared Test. b Mann-Whitney U test. Abbreviations: BFV, blood flow volume; N-CHS, non-cerebral hyperperfusion syndrome; CHS, cerebral hyperperfusion syndrome.
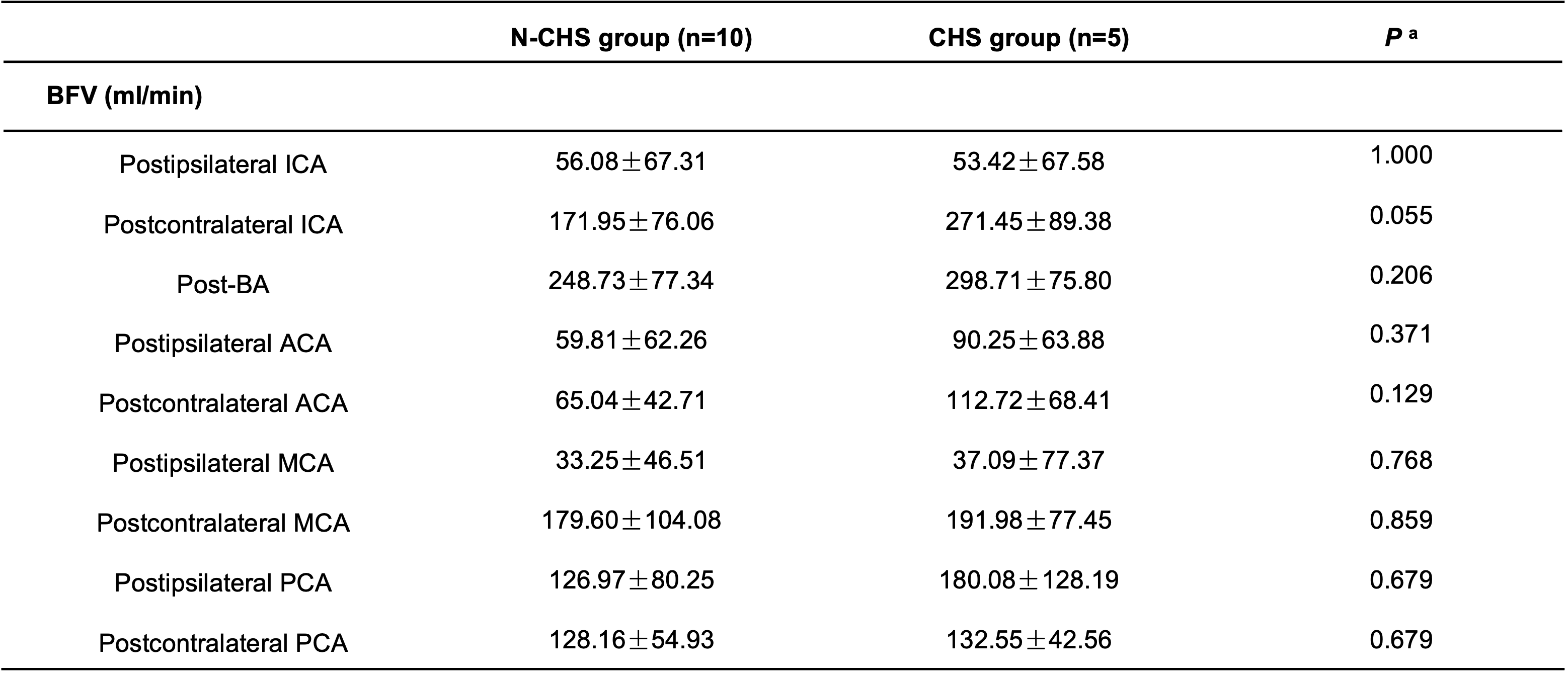
Table 2. The blood flow of each artery after STA-MCA bypass.
Notes: Values are presented as mean ± standard deviation (SD). a Mann-Whitney U test. Abbreviations: BFV, blood flow volume; N-CHS, Non-cerebral hyperperfusion syndrome; CHS, cerebral hyperperfusion syndrome.