1350
3D-TOF MRA at 5.0T MR:Visualization of Superior Cerebellar Artery1Shandong Provincial Third Hospital, Jinan, China, 2United Imaging Research Institute of Intelligent Imaging, Bejing, China
Synopsis
Keywords: Blood Vessels, Blood vessels
Motivation: To improve non-invasive visualization of the superior cerebellar artery (SCA) for better clinical outcomes.
Goal(s): To assess the feasibility of using 3D-TOF MRA at 5.0 T MR for detailed imaging of the SCA.
Approach: Retrospective analysis of high-resolution 5.0T MR images from patients with suspected cerebrovascular diseases, focusing on the SCA's anatomical details.
Results: The study confirmed that 5.0T MRA provides accurate SCA imaging, consistent with anatomical and CTA results, crucial for diagnosing and managing related cerebrovascular conditions.
Impact: The study provides a new non-invasive benchmark for SCA imaging, potentially reducing iatrogenic risks in neurosurgery and informing the etiology of trigeminal neuralgia, paving the way for safer surgical practices and targeted treatments.
Introduction
The Superior Cerebellar Artery (SCA), a crucial part of the vertebrobasilar artery system, plays a significant role in neuroimaging and neurosurgical procedures involving the cerebellum and brainstem. It serves as a landmark for identifying the trochlear nerve's path. With 75% of trigeminal neuralgia cases linked to SCA and about 36% of ischemic cerebellar strokes associated with its obstruction, the anatomical detailing of SCA is vital for diagnosis and treatment planning. Historically, evaluations of SCA relied on invasive methods like DSA, which posed risks of radiation and allergic reactions. This study focuses on the non-invasive visualization of SCA using 3D Time-Of-Flight Magnetic Resonance Angiography (3D-TOF MRA) at 5.0 T, a method with high resolution and signal-to-noise ratio that mitigates the drawbacks of previous techniques. By leveraging the advanced capabilities of 5.0 T ultra-high field MR, this research seeks to establish a new standard for assessing the SCA, enhancing early diagnosis and treatment of related diseases.Method
This study entailed a retrospective analysis of imaging data from 55 patients (19 males and 36 females, aging 36-81), who underwent 5.0T MR brain MRA for suspected cerebrovascular diseases between May and June 2023. Ethical approval was granted by the Third Hospital of Shandong Province's Ethics Committee. Imaging was performed using a UIH 5.0 T ultra-high field MR system. Parameters for the 3D-TOF MRA included a TR of 20ms, TE of 3.8ms, with images captured over 4 minutes 15 seconds. These images were then assessed by four experienced radiologists for SCA origin, branching, and internal diameter using SYNAPSE PACS measurement tools. Data analysis was conducted with SPSS 23.0 software, employing the Kolmogorov-Smirnov test to ensure normality and recognizing p-values less than 0.05 as indicative of statistical significance.Results
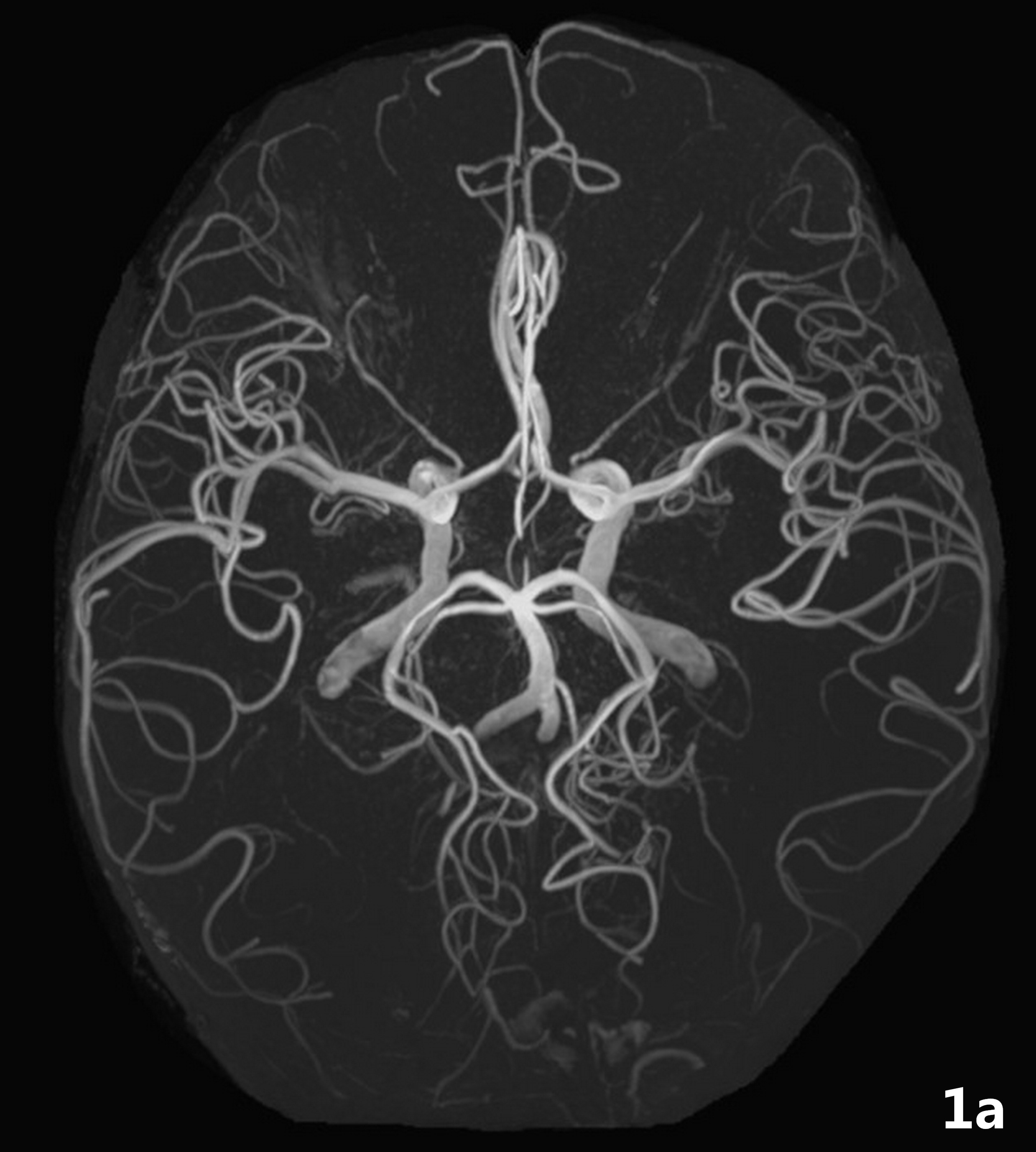
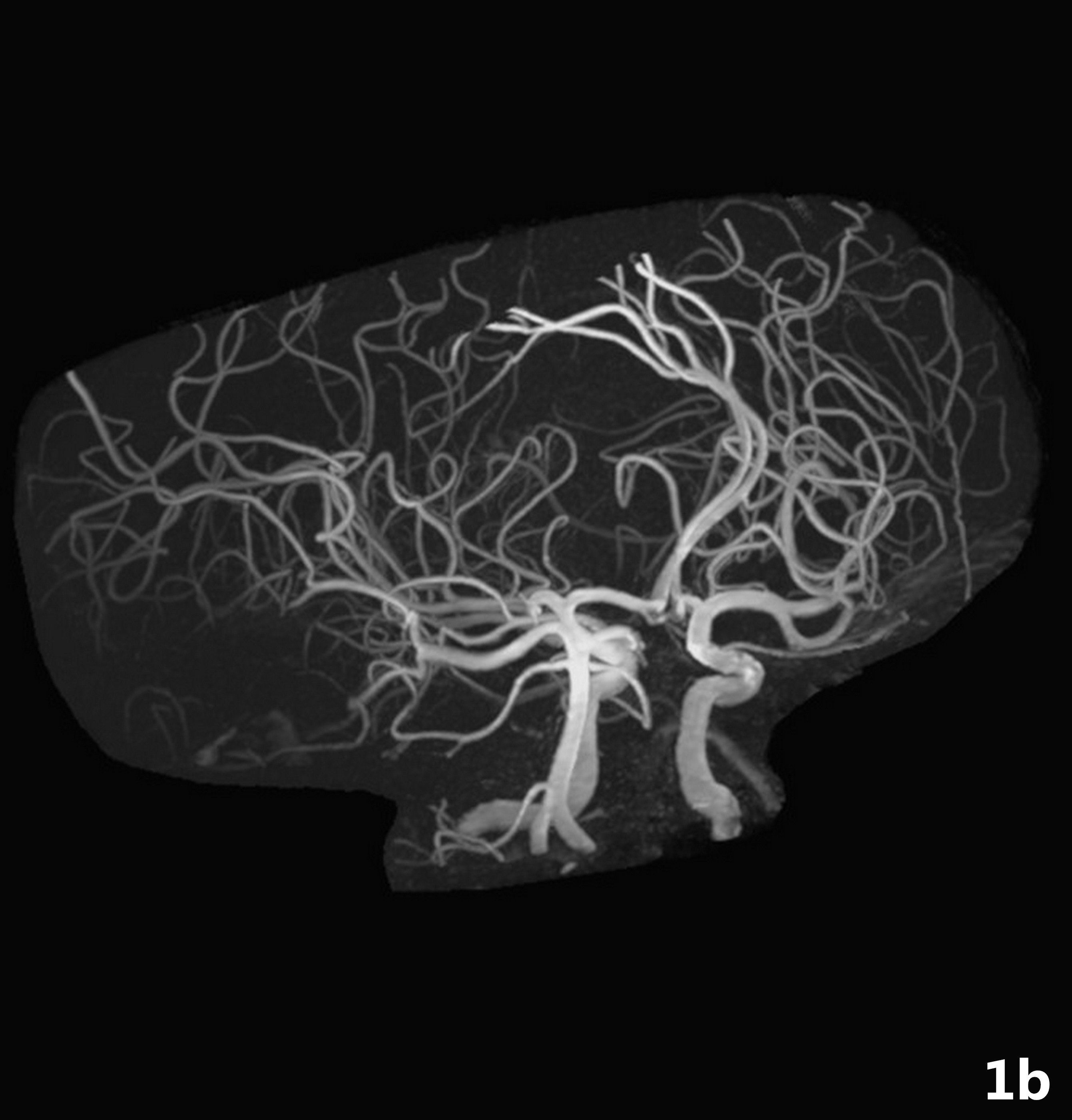
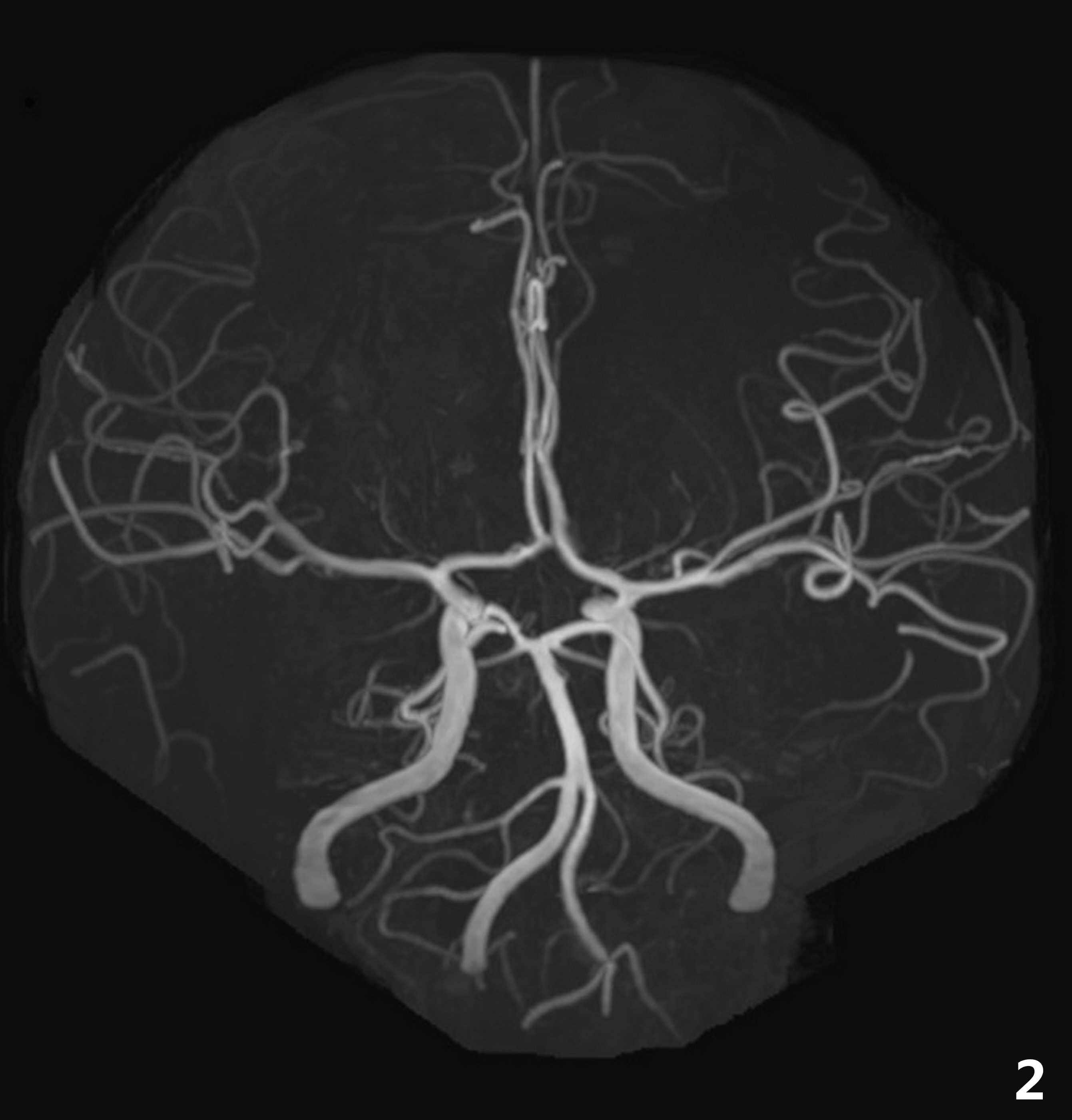
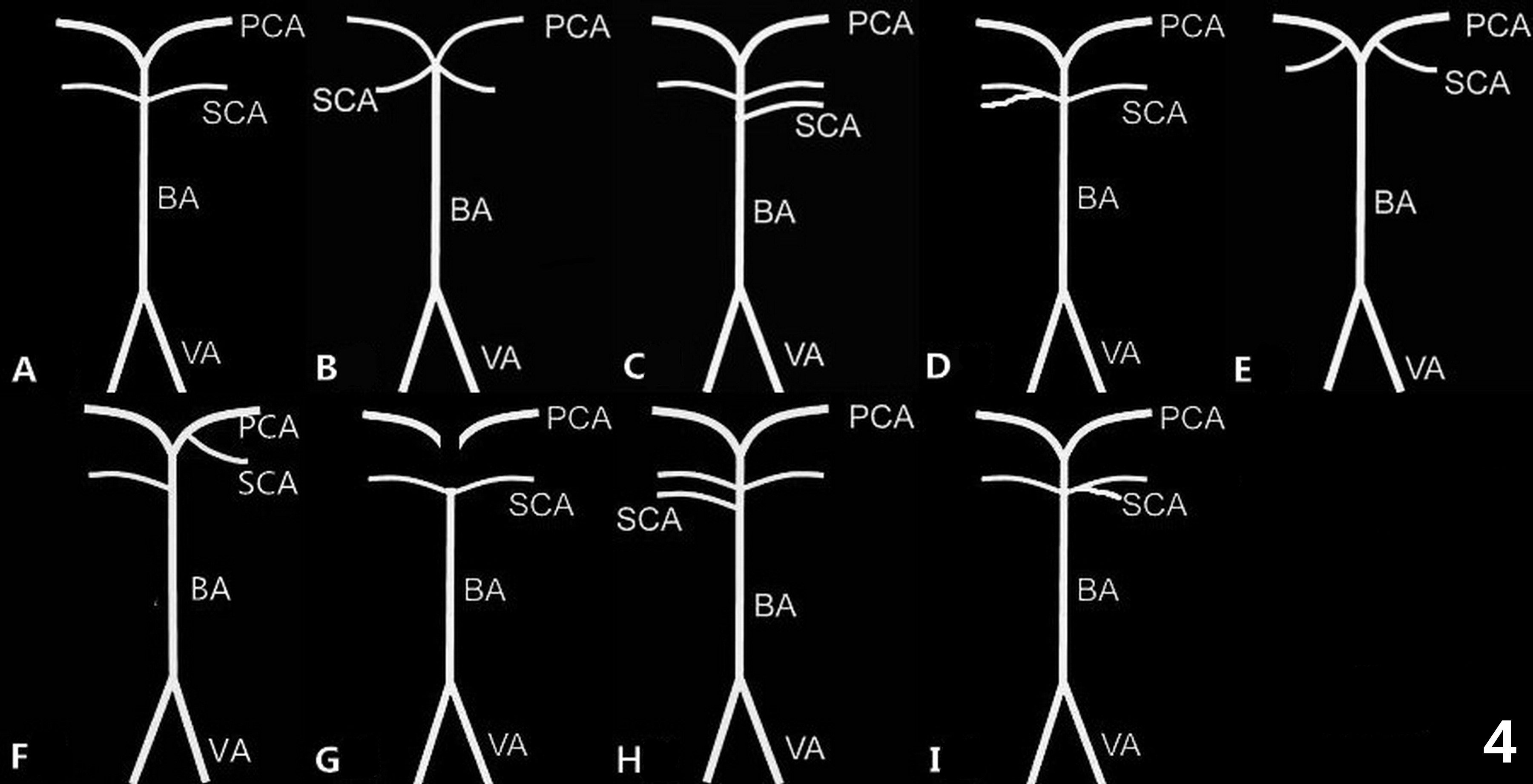
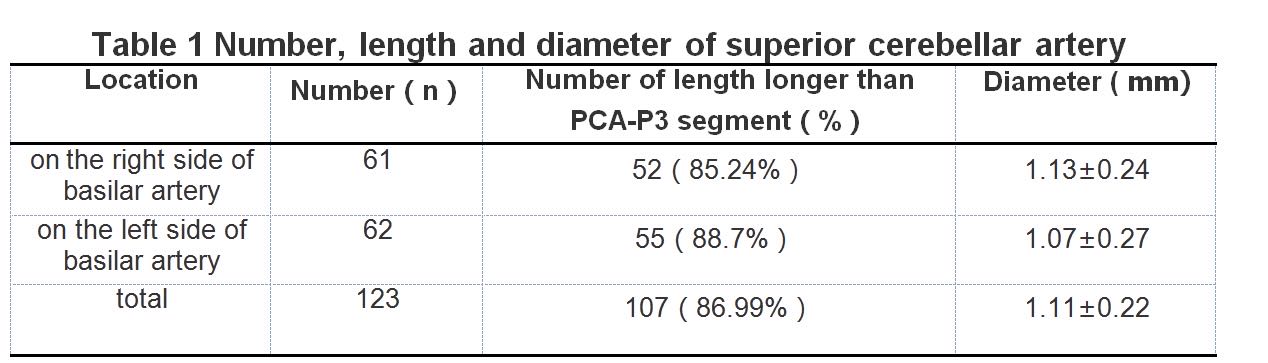
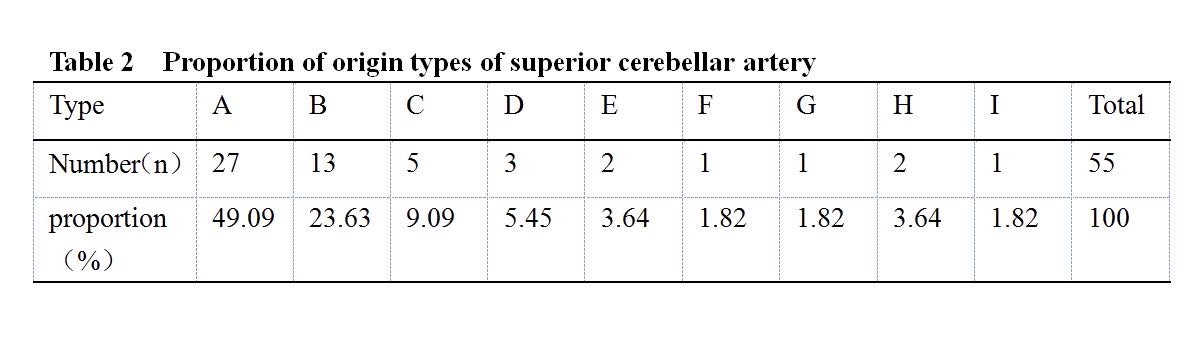
The origin and shape of superior cerebellar artery can be well displayed in 5.0 T 3D-TOF MRA (Figure 1-3). About 87% of the subjects showed that the superior cerebellar artery was longer than the P3 segment of the posterior cerebral artery. 123 superior cerebellar arteries were detected in 55 subjects, 61 on the right side of basilar artery and 62 on the left side of basilar artery. There is no obvious difference in the diameters of the left and right blood vessels (t=1.345, P = 0.184). (Table 1) According to the origin of superior cerebellar artery and the relationship between superior cerebellar artery and posterior cerebral artery, 55 subjects in this study were divided into 9 types of origin (Figure 4), of which type A accounted for the highest proportion, about 49%, followed by type B, about 24%;the proportion of other types is shown in Table 2.Discussion
This study utilized 3D-TOF-MRA at 5.0T MR to depict the superior cerebellar artery (SCA), demonstrating that this high-resolution imaging can non-invasively delineate SCA's origin, caliber, and course. The SCA, a consistent branch in the cerebellar artery system, is crucial for evaluating cerebellar infarction, trigeminal neuralgia, and other cerebellopontine angle pathologies. Previous morphological studies on SCA were mostly autopsy-based, with limited research utilizing MRA. The findings indicate that the SCA's diameter measured by 5.0T MRA aligns with anatomical and CTA results, which is significant since narrower vessels may be predisposed to ischemic events. Recognizing abnormal SCA stenosis during imaging is vital to prevent iatrogenic injury during surgical interventions. Moreover, understanding the variability in SCA's origin and morphology can influence the pathophysiology of conditions like trigeminal neuralgia, where vessel compression is a known factor.Conclusion
This research highlights that 5.0T MR imaging can effectively display SCA, with a high consistency in showing distal branches compared to anatomical studies. However, limitations include the single-center study design, lack of quantitative signal strength analysis, and absence of validation against CTA/DSA or comparison with 3.0T imaging. Further research could address these gaps and expand on the clinical implications of SCA-related diseases.Acknowledgements
We would like to thank the following people for their support, without those help this work would never have been possible.We gratefully acknowledge the help provided by Dr. Jie Gan, who providing many help in the experiment design,research summary,technology support.We thank Dr.Zudong Yin,Dr.Xiangsen Jiang,Dr.Lei Yu for assistance with sample collection,test data, tables and figures. Thanks are also due to Dr. Dan Yu, for her valuable suggestions and discussions. We also thank UNITED IMAGE for providing us with the equipment and technical support,who gave us much valuable support in the early stages of this work.References
[1]Lv Boshi,Xia Hui,Sun Fenggang, et al. Applied Anatomy of Superior Cerebellar Artery of Human[J].Progress of Anatomical Sciences,2007,13(4):303-305.DOI:10.3969/j.issn.1006-2947.2007.04.005[2]Barker FG 2nd, Jannetta PJ, Bissonette DJ, Larkins MV, Jho HD. The long-term outcome of microvascular decompression for trigeminal neuralgia[J]. N Engl J Med. 1996;334(17):1077-1083. DOI:10.1056/NEJM199604253341701[3]Venti M. Cerebellar infarcts and hemorrhages[J].Front Neurol Neurosci. 2012;30:171-175.DOI:10.1159/000333635[4]KRZYżEWSKI RM,STACHURA MK,STACHURA AM,et al.Variations and morphometric analysis of the proximal segment of the superior cerebellar artery[J].Neurol Neurochir Pol.2014;48(4):229-235.DOI:10.1016/j.pjnns.2014.07.006[5] MacDonald ME, Frayne R. Cerebrovascular MRI: a review of state-of-the-art approaches, methods and techniques[J]. NMR Biomed. 2015;28(7):767-791. DOI:10.1002/nbm.3322 [6] Ozsarlak O, Van Goethem JW, Maes M, Parizel PM. MR angiography of the intracranial vessels: technical aspects and clinical applications[J]. Neuroradiology. 2004;46(12):955-972. DOI:10.1007/s00234-004-1297-9[7]Guo Aiwen,Gao Ppeng,Zeng Feihong,et al. The value of combining basi-parallel anatomical scanning and MRA for the diagnosis of intracranial vertebrobasilar artery diseases[J].Journal of Practical Radiology,2020(06):855-858. DOI:10.3969/j.issn.1002-1671.2020.06.001[8]Shan Yanli,Ji Shengzhang,Chen Shengli. MRA classification and imaging features of vertebrobasilar dolichoectasia[J].Journal of Practical Radiology,2017,33(5):674-676,687. DOI:10.3969/j.issn.1002-1671.2017.05.006[9] Shi Zhang,Miao Xiyin,Zhu Shuo,et al. The clinical value of 5.0 T ultra-high field MRI in assessing intracranial arteries and branches [J]. Chinese Journal of Radiology,2022,56(08):886-891.DOI:10.3760/cma.j.cn112149-20211224-01142[10]SHI Z,ZHAO X,ZHU S,et al.Time-of-Flight Intracranial MRA at 3 T versus 5 T versus 7 T: Visualization of Distal Small Cerebral Arteries.Radiology.2022;305(3):E72. DOI:10.1148/radiol.229027[11] von Morze C, Xu D, Purcell DD, et al. Intracranial time-of-flight MR angiography at 7T with comparison to 3T[J]. J Magn Reson Imaging,2007;26(4):900-904.DOI:10.1002/jmri.21097[12]Sartoretti T, van Smoorenburg L, Sartoretti E, et al. Ultrafast Intracranial Vessel Imaging With Non-Cartesian Spiral 3-Dimensional Time-of-Flight Magnetic Resonance Angiography at 1.5 T: An In Vitro and Clinical Study in Healthy Volunteers[J]. Invest Radiol 2020;55(5):293-303. DOI:10.1097/RLI.0000000000000641[13]Deng X, Zhang Z, Zhang Y, et al. Comparison of 7.0- and 3.0-T MRI and MRA in ischemic-type moyamoya disease: preliminary experience[J]. J Neurosurg 2016;124(6):1716-1725. DOI:10.3171/2015.5.JNS15767[14] Willinek WA, Born M, Simon B, et al. Time-of-flight MR angiography: comparison of 3.0-T imaging and 1.5-T imaging-initial experience[J]. Radiology, 2003, 229(3):913-920. DOI: 10.1148/radiol.2293020782[15]Sun Shengjun,DaiJianping,Gao Peiyi. Infarction of the Cerebellum Dignosis by MRI [J]. Chinese Journal of Medical Imaging Technology,2000(11):942-944.DOI:10.13929/j.1003-3289.2000.11.011[16]SONGUR A,GONUL Y,OZEN OA,et al.Variations in the intracranial vertebro-basilar system.Surg Radiol Anat.2008;30(3):257-264. DOI:10.1007/s00276-008-0309-6. [17] CUI Yu-hui,XU Tao,CHEN Jiong, et al.Microsurgical anatomy of the superior cerebellar artery and the variations [J]. Military Medical Journal of Southeast China,2013,15(2),147-149. DOI:10.3969/j.issn.1672-271X.2013.02.016[18] BAI Mingjun,LI Qingling, GUO Yuefei,et al. Morphological Study on Superior Cerebellar Artery with 320 -Detector Row Computed Tomography Angiography [J]. Chinese Journal of Medical Physics,2014,31(06):5285-5287.DOI:10.3969/j.issn.1005-202X.2014.06.015[19]Uchino A, Sawada A, Takase Y, Kudo S. Variations of the superior cerebellar artery: MR angiographic demonstration. Radiat Med. 2003 Nov-Dec;21(6):235-8.PMID: 14743895[20]Mi Long,Song Yunlong,Chen Hong,et al. Preliminary study of vascular compression and morphological characteristics of trigeminal nerve bridge forebay section by 3D-TOF MRA combined with 3D-FIESTA [J]. Journal of Practical Radiology,2018,34(8):1160-1163,1171. DOI:10.3969/j.issn.1002-1671.2018.08.002[21]ZhuChuanqing,Yu Zefeng,GuoChunfeng,et al. The diagnostic value of 3D-TOF-MRA in combination with 3D-FIESTA-C in preoperative evaluation of vascular compressive trigeminal neuralgia[J].Journal of Practical Radiology,2018,34(2):180-183.DOI:10.3969/j.issn.1002-1671.2018.02.004[22]Shen Jian,Zhang Huimei,Shen Weiqiang,et al. Value of Magnetic Resonance 3D-FIESTA Combined with 3D-TOF Sequence in Locating Neurovascular Compression for Primary Trigeminal Neuralgia[J].Journal of Clinical Radiology,2018,37(02):190-193. DOI:10.13437/j.cnki.jcr. 2018.02.003.[23]Wang Wuqing,Fu Rong,Bi Guorong,et al. China expert consensus on diagnosis and treatment of vascular dizziness/vertigo [J]. Chinese Journal of Neuroimmunology and Neurology,2020, 27(04):253-260.DOI10.3969/j.issn.1006-2963.2020.04.002Figures