1346
Enhanced Leptomeningeal Collateral Visualization in Moyamoya Disease: A 5.0-T 4D NCEMRA Study1Department of Radiology, State Key Laboratory of Complex Severe and Rare Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 2MR Collaboration, United Imaging Research Institute of Intelligent Imaging, Beijing, China, 3United Imaging Research Institute of Intelligent Imaging, Beijing, China, 4Department of Neurology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 5Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Beijing, China, 6China National Clinical Research Center for Neurological Diseases, Beijing, China, 7Department of Neurosurgery, Beijing Hospital, National Center of Gerontology, Beijing, China, 8Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, China
Synopsis
Keywords: Blood Vessels, Blood vessels, 5.0-T magnetic resonance angiography
Motivation: Moyamoya disease necessitates precise visualization of cerebral vessels for management, but current imaging may be inadequate.
Goal(s): To ascertain if 5.0-T 4D NCEMRA offers superior imaging of collateral circulation in Moyamoya disease compared to traditional TOF MRA.
Approach: Utilized 5.0-T MRI to compare 4D NCEMRA and TOF MRA in visualizing leptomeningeal collateral anastomoses in 19 patients.
Results: 5.0-T 4D NCEMRA outperformed TOF MRA, particularly in identifying leptomeningeal collaterals, with significant statistical support.
Impact: The study underscores 5.0-T 4D NCEMRA's potential to enhance cerebral vascular mapping in Moyamoya disease, prompting advancements in diagnostic and therapeutic strategies, possibly leading to more personalized patient care.
Introduction
Moyamoya disease (MMD) epitomizes a chronic, progressive cerebrovascular disorder that is hallmarked by stenosis or occlusion of the intracranial internal carotid artery (ICA) and the circle of Willis, leading to significant morbidity due to cerebral ischemia1. As MMD progresses, this compensatory mechanism of collateral circulation becomes crucial. It encompasses Moyamoya vessels, leptomeningeal anastomosis, and transdural anastomosis, each of which can be integral in preserving cerebral blood flow 2-3.The evaluation of these collateral pathways is pivotal in the management and prognostication of MMD. Time-of-flight (TOF) magnetic resonance angiography (MRA) has long been a cornerstone in the noninvasive imaging of MMD, with its ability to detect ICA occlusion and Moyamoya vessels rendering conventional angiography often unnecessary4. However, the conventional 1.5-T or 3.0-T TOF MRA systems have been challenged for their lack of precision in visualizing the collateral circulation, a critical component in the disease's pathology5. This limitation is particularly pronounced in vessels with slow flow or those oriented out of the standard inferior-to-superior direction, which are typically present in MMD9.The advent of ultra-high-field MRI systems, such as the 7.0-T, has shifted the paradigm by offering superior signal-to-noise ratios and longer T1 relaxation times, thus enabling better visualization of the small collateral vessels6-8. However, these systems are not without their drawbacks, which include increased susceptibility to artifacts and limited availability. In this context, the 5.0-T MRI system emerges as a promising middle ground, boasting an imaging quality that not only contends with the 7.0-T but also significantly surpasses the 3.0-T system10. A particularly notable advancement is the 4D non-contrast enhanced MRA (NCEMRA), which provides dynamic, high-resolution imaging of blood flow without the need for contrast agents. This technique mitigates the risk associated with gadolinium-based agents and offers both anatomical and hemodynamic information, thus holding the potential to revolutionize the visualization of collateral circulation in MMD. Our study conducts a comprehensive comparison between the 4D NCEMRA and TOF MRA in visualizing the intricate network of collateral vessels in MMD patients.Materials and Methods
We included 29 hemispheres from 19 patients diagnosed with ischemic-type MMD (11 females, age 18 - 61 years). Each patient underwent both 4D NCEMRA and TOF MRA using a state-of-the-art 5.0-T MR system. The 4D NCEMRA protocol was based on a pseudo-Continuous Arterial Spin Labeling (pCASL) sequence, with six different labeling durations ranging from 100 to 1800 ms, achieving an isotropic spatial resolution of 0.7mm. For TOF MRA, the acquisition yielded a resolution of 0.6mm isotropic, which was subsequently refined to 0.3 mm3 isotropic via post-processing interpolation. The imaging evaluation employed the modified Houkin’s grading system to assess the main intracranial arteries (MRA score)11. Additionally, a specific Moyamoya vessels (MMVs) area score was utilized to quantify the visualized vessels4. We established a leptomeningeal anastomosis scoring system, ranging from 1 to 4, based on anatomical details such as the extension of retrograde flow into the Sylvian fissure or its presence in superficial vessels only. Statistical comparisons of the imaging modalities were performed using the Wilcoxon matched-pair signed-rank test. We also retrospectively analyzed digital subtraction angiography (DSA) data for corroboration of our findings.Results
The comparative analysis revealed no significant discrepancies between 5.0-T 4D NCEMRA and TOF MRA in MRA score (median score: 3.0 vs 3.0, p = 0.71) and MMV area score (median score: 2.0 vs 2.0, p = 0.18). Nonetheless, a stark contrast emerged in the visualization of collateral anastomoses. The 4D NCEMRA significantly outperformed TOF MRA in detailing the leptomeningeal collateral vessels, as reflected by the the leptomeningeal anastomosis score (median score: 3.0 vs. 1.0, p < 0.001). In particular, leptomeningeal collaterals from the parieto-occipital branch of the PCA to the MCA were identified in 26 hemispheres via 4D NCEMRA, while TOF MRA only detected them in 11 hemispheres. The retrospective DSA comparison supported these findings, demonstrating comparable visualization capabilities with the 4D NCEMRA.Conclusion
The implementation of 5.0-T 4D NCEMRA has proven superior in the visualization of leptomeningeal collateral anastomoses in MMD, markedly better than TOF MRA. This superiority is especially pronounced in delineating retrograde flows from the parieto-occipital branch of the PCA to the MCA. The implications of this study suggest that 5.0-T 4D NCEMRA could serve as a critical imaging modality in the diagnosis, therapeutic planning, and management of MMD, offering clinicians a detailed map of the cerebral vasculature that is paramount in the effective treatment of this complex disease.Acknowledgements
No acknowledgement found.References
1. Guidelines for diagnosis and treatment of moyamoya disease (spontaneous occlusion of the circle of Willis). Neurol Med Chir (Tokyo). 2012;52(5):245-66. doi:10.2176/nmc.52.245
2. Togao O, Mihara F, Yoshiura T, et al. Cerebral hemodynamics in Moyamoya disease: correlation between perfusion-weighted MR imaging and cerebral angiography. AJNR Am J Neuroradiol 2006;27(2):391–39
3. Liu ZW, Han C, Zhao F, et al. Collateral Circulation in Moyamoya Disease: A New Grading System. Stroke. Oct 2019;50(10):2708-2715. doi:10.1161/strokeaha.119.024487
4. Jin Q, Noguchi T, Irie H, et al. Assessment of Moyamoya disease with 3.0-T magnetic resonance angiography and magnetic resonance imaging versus conventional angiography. Neurol Med Chir (Tokyo). 2011;51(3):195-200. doi:10.2176/nmc.51.195
5. Filimonova E, Ovsiannikov K, Rzaev J. Neuroimaging in Moyamoya angiopathy: Updated review. Clin Neurol Neurosurg. Nov 2022;222:107471. doi:10.1016/j.clineuro.2022.107471
6. Deng X, Zhang Z, Zhang Y, et al. Comparison of 7.0- and 3.0-T MRI and MRA in ischemic-type moyamoya disease: preliminary experience. J Neurosurg. Jun 2016;124(6):1716-25. doi:10.3171/2015.5.Jns15767
7. Oh BH, Moon HC, Baek HM, et al. Comparison of 7T and 3T MRI in patients with moyamoya disease. Magn Reson Imaging. Apr 2017;37:134-138. doi:10.1016/j.mri.2016.11.019
8. Matsushige T, Kraemer M, Sato T, et al. Visualization and Classification of Deeply Seated Collateral Networks in Moyamoya Angiopathy with 7T MRI. AJNR Am J Neuroradiol. Jul 2018;39(7):1248-1254. doi:10.3174/ajnr.A5700
9. Togao O, Hiwatashi A, Obara M, et al. Acceleration-selective Arterial Spin-labeling MR Angiography Used to Visualize Distal Cerebral Arteries and Collateral Vessels in Moyamoya Disease. Radiology. 2018 Feb;286(2):611-621. doi: 10.1148/radiol.2017162279/
10. Shi Z, Zhao X, Zhu S, et al. Time-of-Flight Intracranial MRA at 3 T versus 5 T versus 7 T: Visualization of Distal Small Cerebral Arteries. Radiology. Dec 2022;305(3):E72. doi:10.1148/radiol.229027
11. Houkin K, Nakayama N, Kuroda S, et al: Novel magnetic resonance angiography stage grading for moyamoya disease. Cerebrovasc Dis 20:347– 354, 2005.
Figures
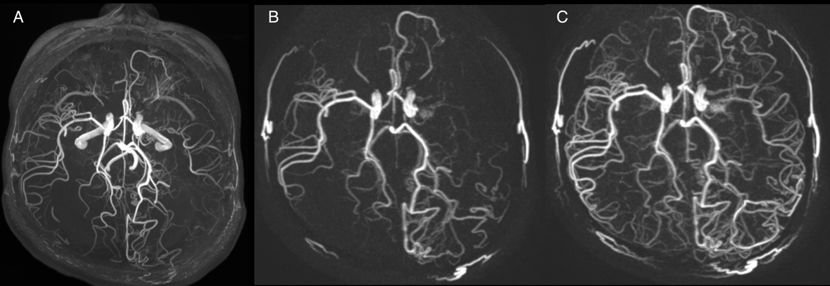
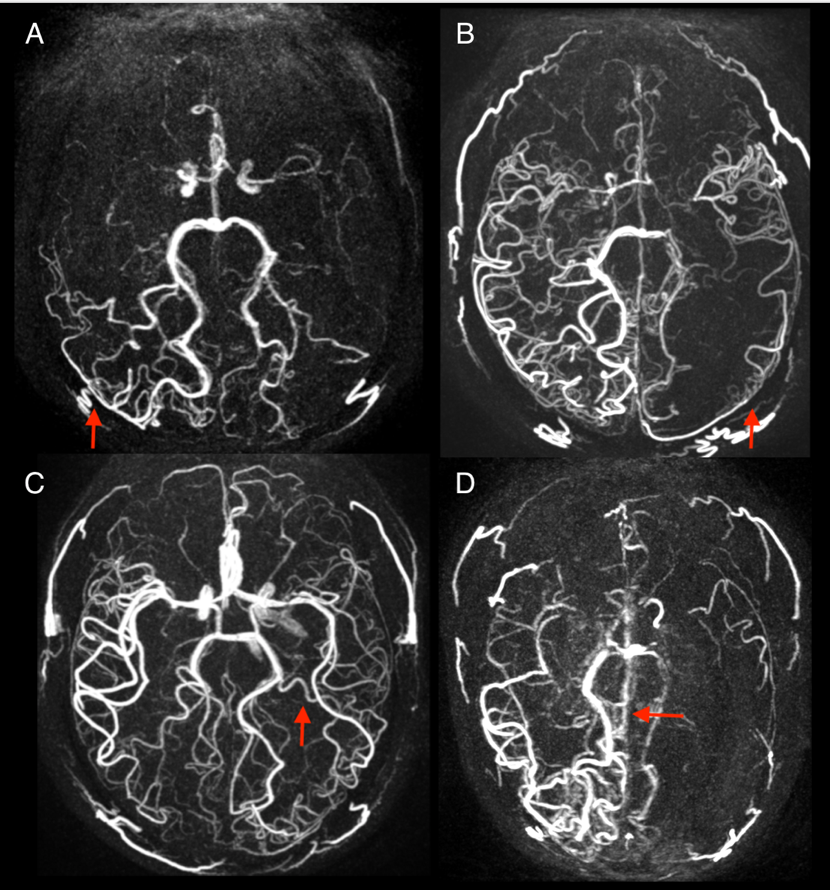
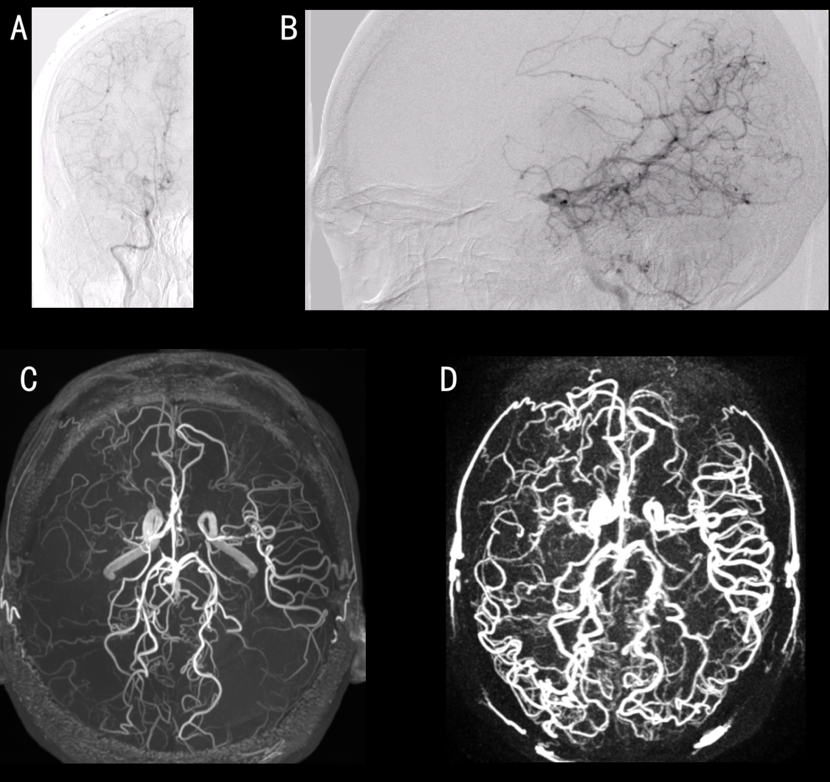
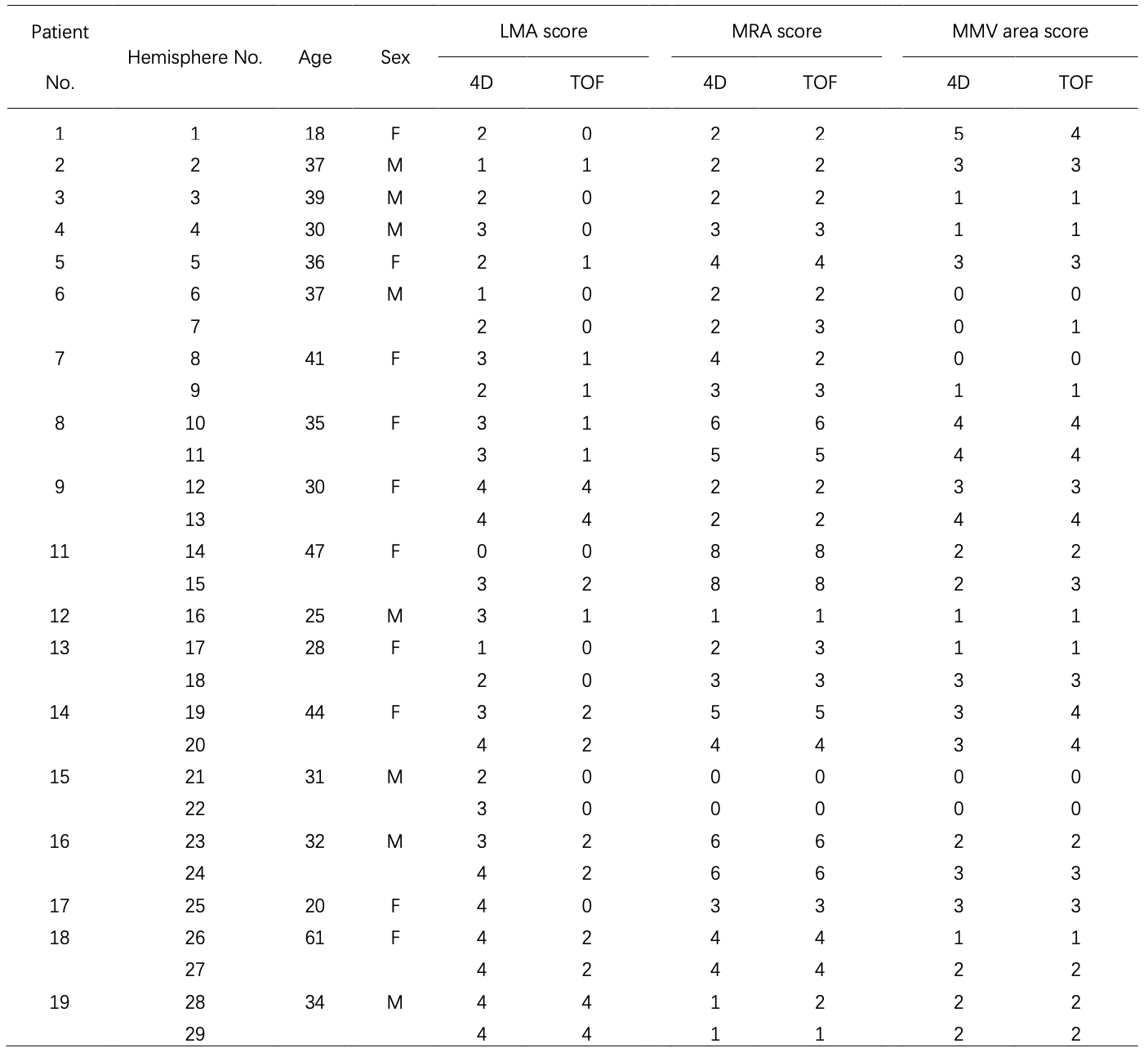
Table 1. Characteristics, LMA scores, MRA scores and MMV area scores of the subjects.
LMA= Leptomeningeal anastomosis