1343
Simulation-based optimization and experimental comparison of intracranial T2-weighted DANTE-SPACE vessel wall imaging at 3T and 7T1Wellcome Centre for Integrative Neuroimaging, FMRIB, Nuffield Department of Clinical Neurosciences, University of Oxford, Oxford, United Kingdom, 2Spinoza Centre for Neuroimaging, Amsterdam, Netherlands, 3Computational Cognitive Neuroscience and Neuroimaging, Netherlands Institute for Neuroscience, KNAW, Amsterdam, Netherlands, 4Department of Radiology and Nuclear Medicine, Amsterdam University Medical Centers, University of Amsterdam, Amsterdam, Netherlands
Synopsis
Keywords: Blood Vessels, Vessels, Vessel Wall; Neurovascular; Ultra-high field
Motivation: T2-weighted DANTE-SPACE is a promising sequence for intracranial black-blood vessel wall imaging at 7T. However, it is limited by signal and contrast variations and its performance versus 3T remains unclear.
Goal(s): To optimize T2-weighted DANTE-SPACE at both 3T and 7T, and to quantitatively compare their performance.
Approach: A recently introduced DANTE-SPACE simulation framework was used for protocol optimization. Data acquired from six healthy volunteers at 3T and 7T were then quantitatively compared.
Results: Optimization of DANTE-SPACE parameters at 7T provides a 24% increase in vessel visibility over a literature protocol. Contrasts at 7T are 90% higher than at 3T.
Impact: Through simulation-based optimization, the vessel wall contrasts from T2-weighted DANTE-SPACE at 7T were improved by 24% versus a literature protocol. When optimized and implemented at 3T, in-vivo data showed a much lower vessel wall contrast-to-noise relative to 7T.
Introduction
Intracranial vessel wall imaging (VWI) aims to non-invasively characterize vessel wall (VW) pathology. For this, the DANTE-SPACE sequence uses DANTE (delay alternating with nutation for tailored excitation)1 preparation for suppression of blood and CSF, followed by a variable flip angle turbo-spin-echo (SPACE)2 readout module.Previous T2-weighted DANTE-SPACE results at 7T showed substantial variations in the achieved contrasts and a 50% reduced wall-to-lumen contrast compared to regular SPACE3, hindering clinical implementation. At 3T, DANTE-SPACE is frequently used as a T1-weighted sequence, but no conclusive information is available about the optimization and performance of 3D T2-weighted DANTE-SPACE at 3T. Furthermore, no information is currently available about the relative performance of DANTE-SPACE at 3T versus 7T.
This abstract first uses DANTE-SPACE simulations to propose optimized T2-weighted DANTE-SPACE protocols for three scenarios: at 3T; at 7T without parallel transmission (pTx); and at 7T using pTx shims. Subsequently, in vivo data are used to quantitatively compare all three scenarios.
Methods
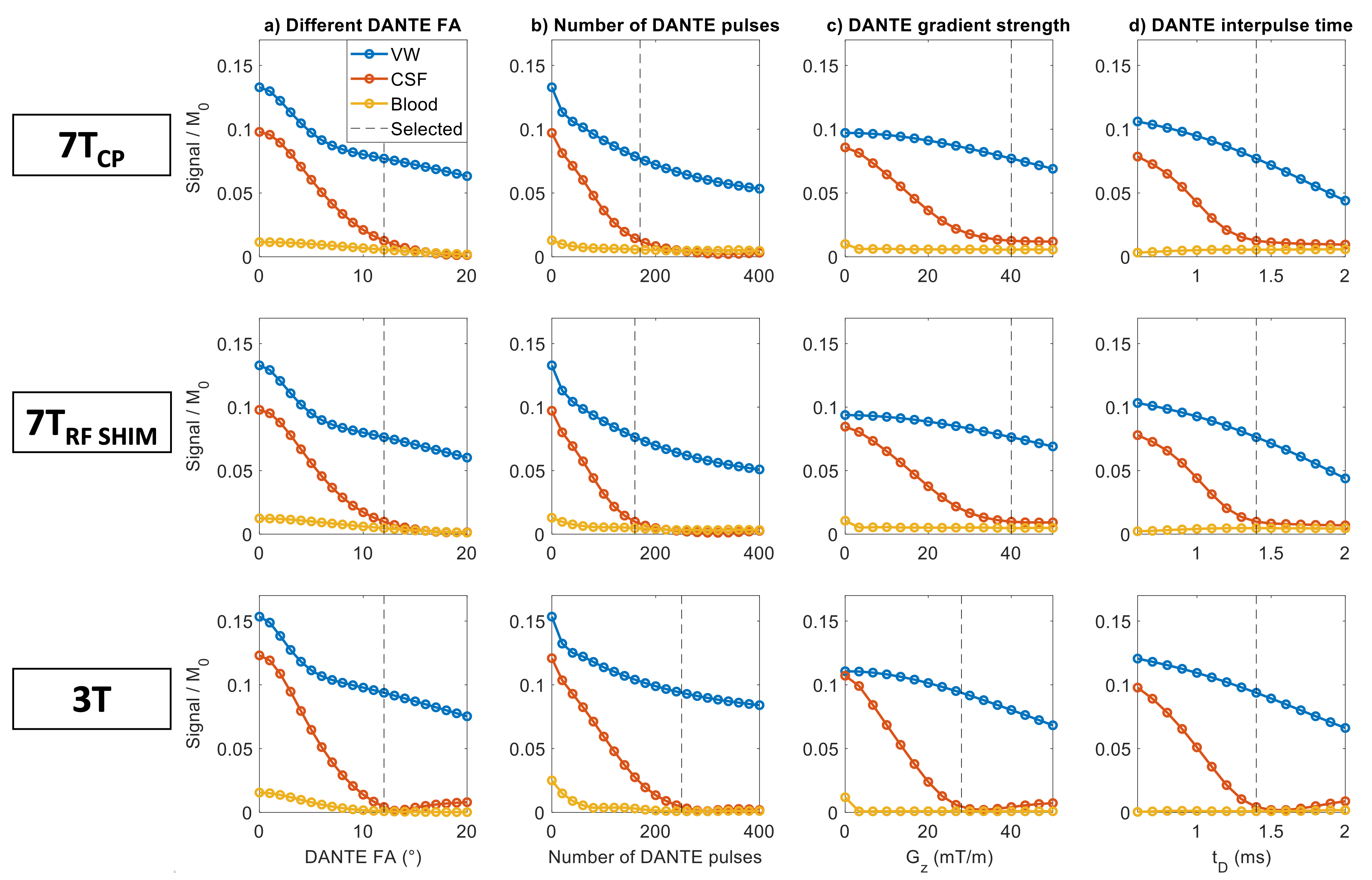
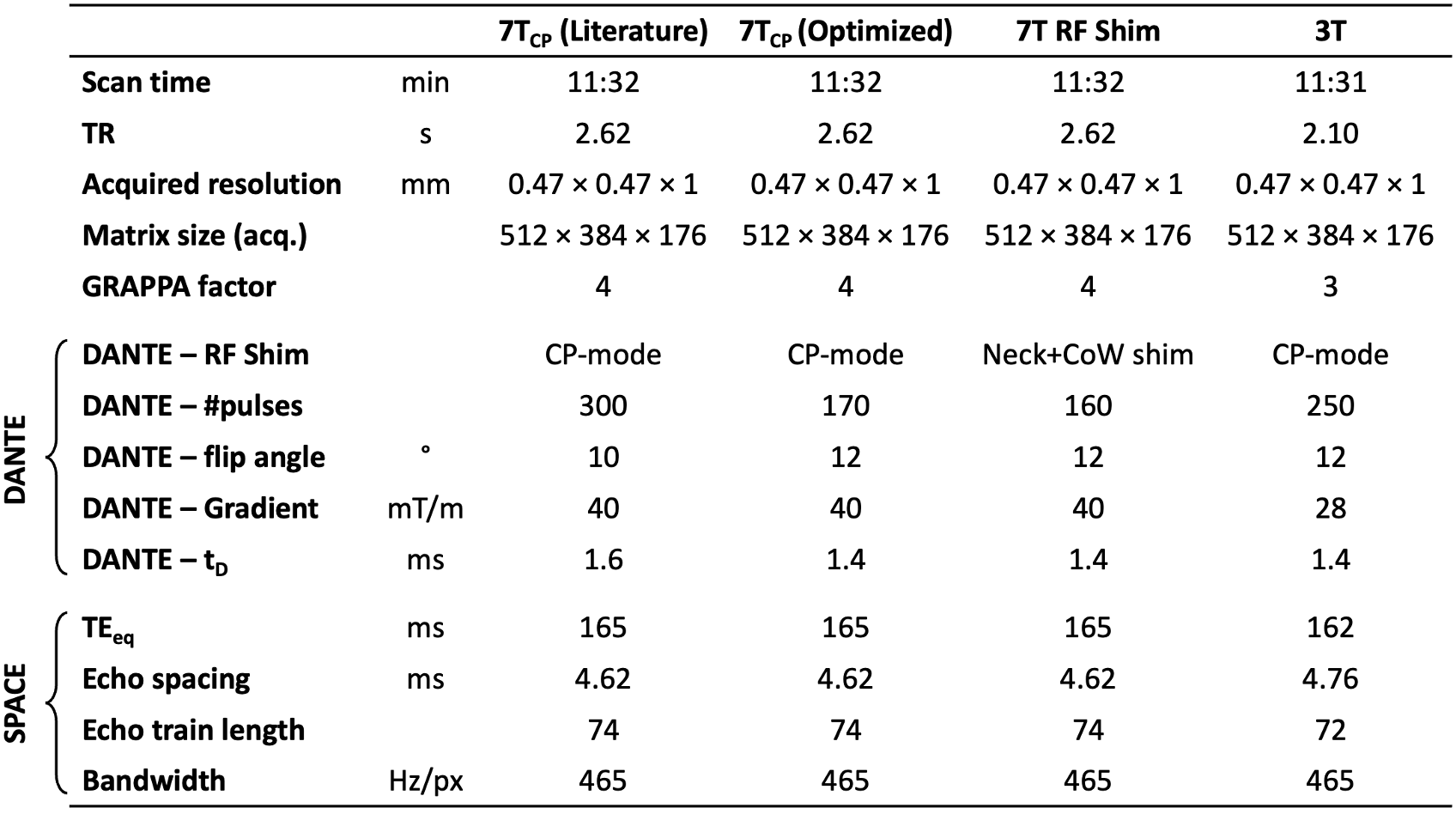
Using a previously presented simulation framework4, VW, CSF, and blood signal were simulated. B1+ variations at 7T were included based on a previously presented database of 7T multi-channel head-and-neck pTx B1+ maps5. Homogeneous B1+ fields were assumed at 3T. Parameter sweeps were used to determine DANTE parameters that optimize the VW-CSF and VW-blood contrasts.At 3T, simulations were first used to propose a T2-weighted SPACE protocol, followed by simulations for DANTE optimization. The scan time, field-of-view, matrix size, echo time, and receive bandwidth were matched to a previous 7T literature protocol3.
Data were acquired from 6 healthy volunteers (24-57 years old) using a Siemens Prisma 3T with a 32Rx head coil and a Siemens Magnetom 7T with a Nova Medical 8Tx/32Rx head coil. Data were reconstructed in B1-weighted SNR units6 using MATLAB. ESPIRiT receive coil sensitivities were estimated using BART7. Acquisitions at 3T and 7T were registered using three-dimensional translation and in-plane rotation.
Using a semi-automatic vessel delineation algorithm8, three vessel acutance (perceived sharpness) parameters9 were derived: inner boundary acutance, outer boundary acutance, and directional root-mean-square signal gradient ($$$G_{RMS}$$$). For 90 radial directions, $$$G_{RMS}$$$ was calculated from the radial gradient $$$G_i=SNR_i-SNR_{i-1}$$$ at each of the $$$n_i$$$ radial profiles across the VW:
$$G_{RMS}=\sqrt{\frac{\sum_{i=1}^{n_i}G_i^2}{n_i}}.$$
Results
At 7T, two separate optimizations were performed: with and without a pTx radiofrequency (RF) shim during the DANTE preparation. A universal “neck-and-CoW” RF shim was found to increase the B1+ in the neck without reducing the B1+ around the Circle of Willis (CoW), thereby improving the suppression of inflowing blood without penalizing CSF suppression.The resulting single-parameter simulation sweeps for 7T without pTx, 7T with pTx, and 3T are shown in Figure 1. SPACE parameters were separately optimized (not shown). The resulting protocols are shown in Table 1.
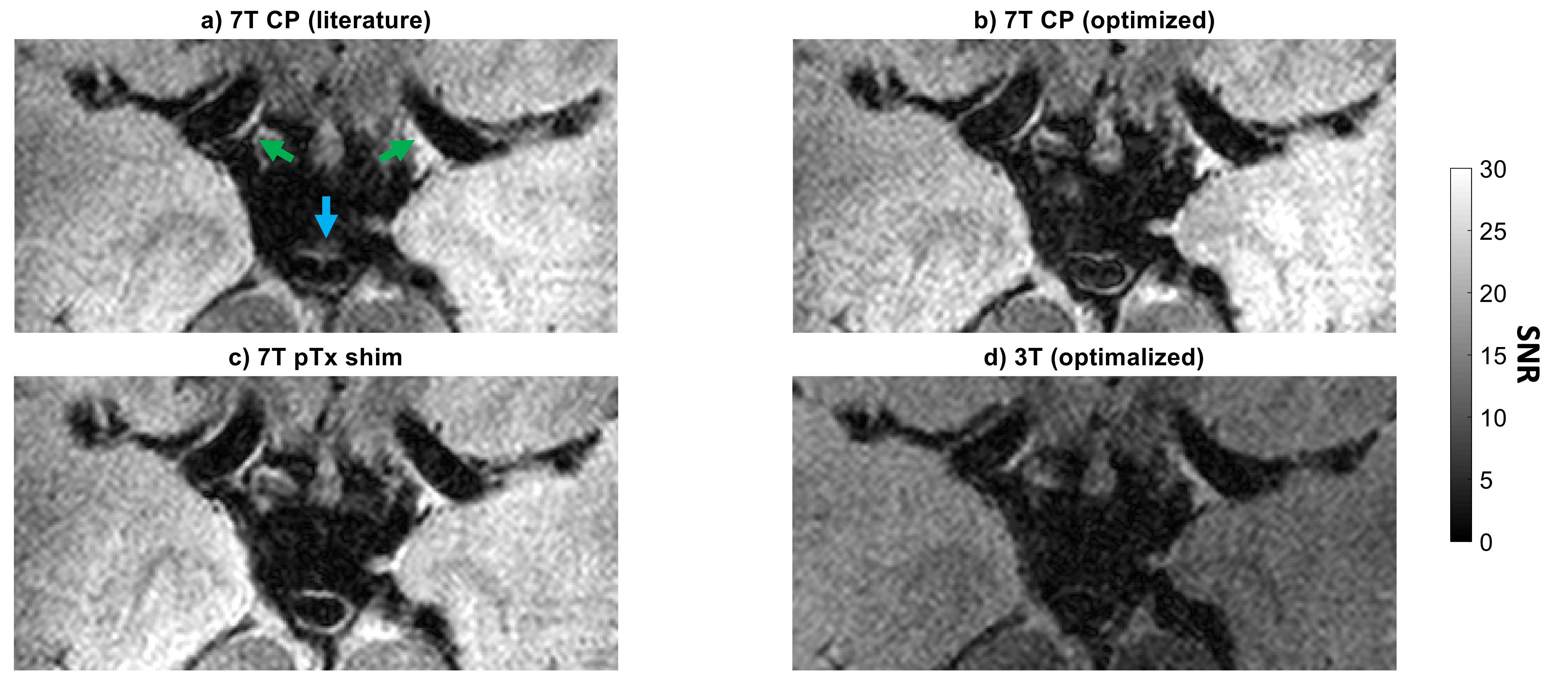
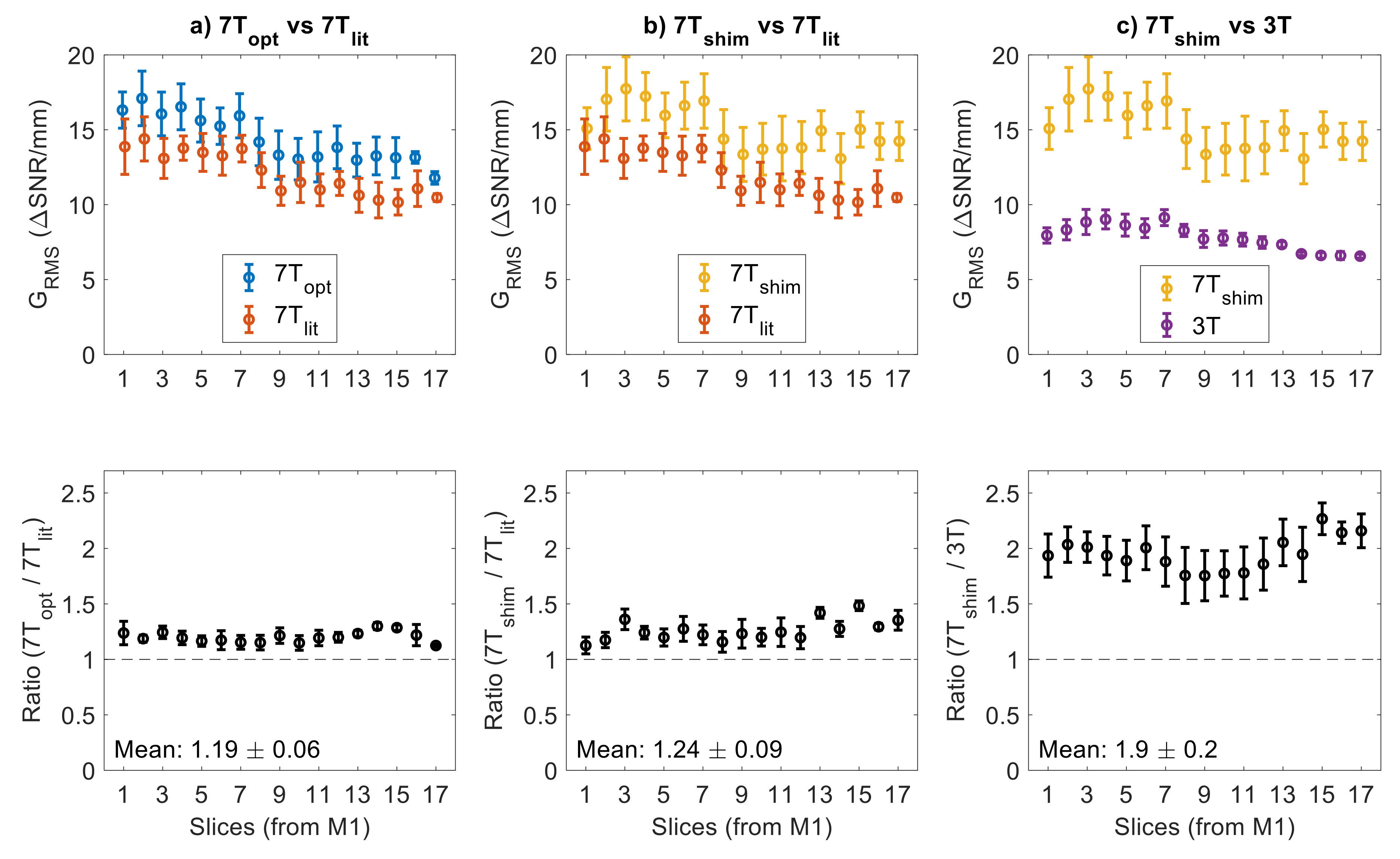
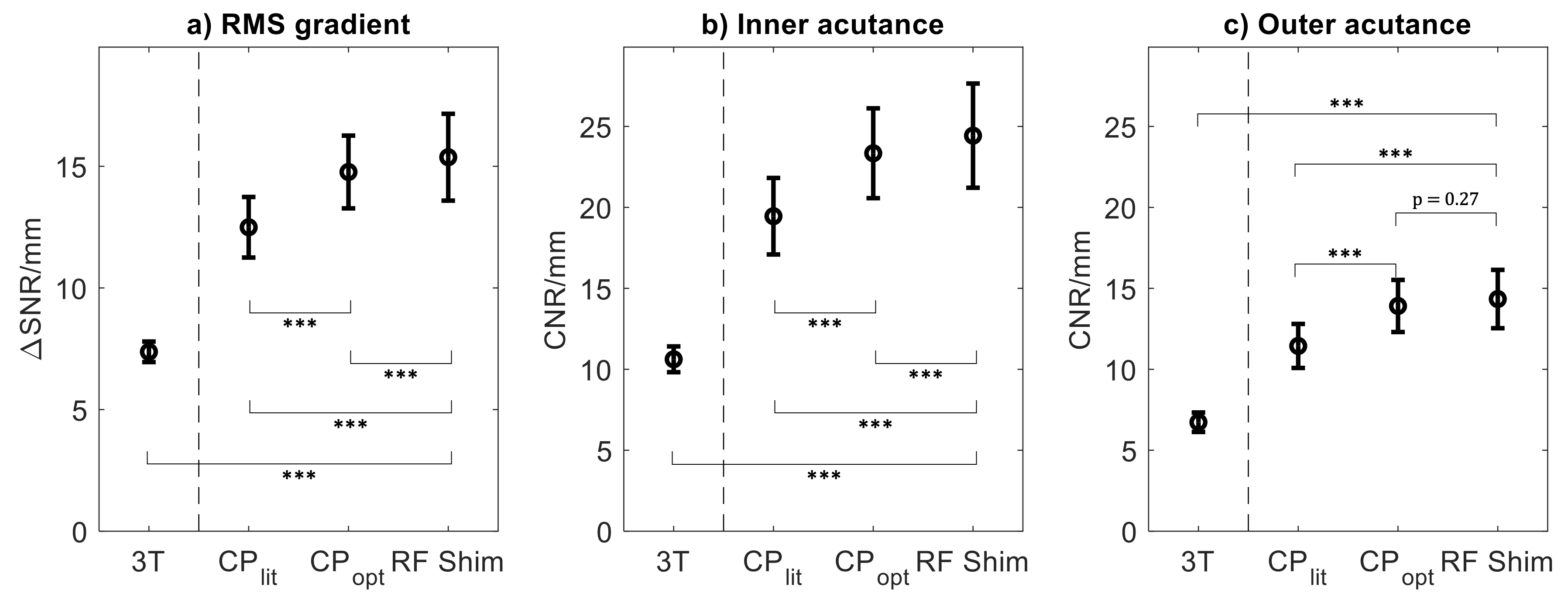
Example data acquired using all four protocols are shown in Figure 2. Figure 3 shows the average $$$G_{RMS}$$$ at different locations. At 7T, compared to the literature protocol, the slice-wise average $$$G_{RMS}$$$ increases by 19±6% using CP (circular polarization)-mode optimized parameters and by 24±9% using the RF shim. The $$$G_{RMS}$$$ is almost two times higher in optimized acquisitions at 7T than at 3T.
Using all three metrics (Figure 4), both optimized protocols at 7T perform significantly ($$$p<0.001$$$) better than the literature protocol, while the results at 3T are significantly worse than at 7T for all metrics.
Discussion
For CP-mode at 7T, optimized DANTE parameters were proposed to improve vessel wall contrasts. A 7T protocol using a universal pTx shim during DANTE was also proposed. Simulations suggest that this shim improves blood suppression by 32% without penalizing the CSF suppression.Figures 2-4 confirm that both optimized protocols at 7T result in significantly improved contrasts relative to the literature protocol. By including an RF shim, a small but significant incremental further improvement is achieved for the $$$G_{RMS}$$$ and inner acutance, but not the outer acutance – consistent with the hypothesized improved blood suppression.
The proposed 3T protocol contains longer DANTE preparation than at 7T. This is required for sufficient CSF-suppression but also substantially reduces VW signal, resulting in a near two-fold reduction in $$$G_{RMS}$$$ relative to 7T. Therefore, whereas DANTE preparation is a suitable option for CSF-suppression in T1-weighted and 7T T2-weighted VWI, better options might be available for T2-weighted imaging at 3T.
Conclusion
Using optimized parameters at 7T, T2-weighted DANTE-SPACE contrasts can be improved. A neck-and-CoW pTx shim during DANTE can be used for additional suppression of inflowing blood.At 3T, T2-weighted DANTE-SPACE requires more DANTE pulses to achieve sufficient CSF suppression. This substantially reduces the VW signal, resulting in nearly 2× lower contrasts than at 7T.
Acknowledgements
MdB received financial support from Siemens Healthineers and the Dunhill Medical Trust. PJ receives support from the Dunhill Medical Trust and the NIHR Oxford Biomedical Research Centre. The Wellcome Centre for Integrative Neuroimaging is supported by core funding from the Wellcome Trust (203139/Z/16/Z).References
1. Li L, Miller KL, Jezzard P. DANTE-prepared pulse trains: A novel approach to motion-sensitized and motion-suppressed quantitative magnetic resonance imaging. Magn Reson Med. 2012;68(5):1423-1438. doi:10.1002/mrm.24142
2. Mugler JP. Optimized three-dimensional fast-spin-echo MRI. Journal of Magnetic Resonance Imaging. 2014;39(4):745-767. doi:10.1002/jmri.24542
3. Viessmann O, Li L, Benjamin P, Jezzard P. T2-Weighted intracranial vessel wall imaging at 7 Tesla using a DANTE-prepared variable flip angle turbo spin echo readout (DANTE-SPACE). Magn Reson Med. 2017;77(2):655-663. doi:10.1002/mrm.26152
4. de Buck MHS, Jezzard P, Hess AT. An Extended Phase Graph-based framework for DANTE-SPACE simulations including physiological, temporal, and spatial variations in model parameters. ArXiv Pre-print. Published online 2023:1-25. doi:10.48550/arXiv.2310.03429
5. de Buck MHS, Kent JL, Jezzard P, Hess AT. Head-and-neck multi-channel B1+ mapping and carotid arteries RF shimming using a parallel transmit head coil. Magn Reson Med. 2023;(EarlyView):1-15. doi:10.1002/mrm.29845
6. Kellman P, McVeigh ER. Image reconstruction in SNR units: A general method for SNR measurement. Magn Reson Med. 2005;54(6):1439-1447. doi:10.1002/mrm.20713
7. Tamir JI, Ong F, Cheng JY, Uecker M, Lustig M. Generalized magnetic resonance image reconstruction using the Berkeley advanced reconstruction toolbox. Proceedings of the ISMRM 2016 Data Sampling and Image Reconstruction Workshop. 2016;2486. doi:10.5281/zenodo.31907
8. Wang Q, Robson MD, Francis JM, et al. Accuracy of quantitative MR vessel wall imaging applying a semi-automated gradient detection algorithm - A validation study. Journal of Cardiovascular Magnetic Resonance. 2004;6(4):895-907. doi:10.1081/JCMR-200036198
9. Biasiolli L, Lindsay AC, Choudhury RP, Robson MD. Loss of fine structure and edge sharpness in fast-spin-echo carotid wall imaging: Measurements and comparison with multiple-spin-echo in normal and atherosclerotic subjects. Journal of Magnetic Resonance Imaging. 2011;33(5):1136-1143. doi:10.1002/jmri.22569
Figures