1341
Determinants of 7T MRI microvascular function and link with small vessel disease burden in an ageing population1Center for Image Sciences, University Medical Center Utrecht, Utrecht, Netherlands, 2Radiology and Nuclear Medicine, Erasmus Medical Center, Rotterdam, Netherlands, 3Neurology, University Medical Center Utrecht, Utrecht, Netherlands, 4Epidemiology, Erasmus Medical Center, Rotterdam, Netherlands, 5Erasmus Medical Center, Rotterdam, Netherlands
Synopsis
Keywords: Blood Vessels, Blood vessels, Small vessel disease, white matter hyperintensities, 7T MRI, small vessel function, Rotterdam Study
Motivation: Novel 7T MR techniques allow non-invasive assessment of cerebral small vessel function, potentially relevant to small vessel disease (SVD), a common cause of stroke and dementia.
Goal(s): Assess determinants of small vessel function and its link to SVD lesion burden.
Approach: Perforating artery blood flow velocity and pulsatility were measured with 7T MRI in 200 participants >60 years from a population-based sample and linked to vascular risk factors and white matter hyperintensity (WMH) volume using linear regression.
Results: Age, blood pressure, and BMI were determinants of small vessel function. In turn, vessel function did not relate to WMH burden.
Impact: In the general aging population, perforating artery blood flow velocity and pulsatility do not relate to whole-brain SVD-lesion load. Other complementary small vessel function measures should be investigated as a potential early marker of SVD.
Introduction
Cerebral small vessel diseases (SVDs) are a major cause of stroke and dementia and roughly 70% of those aged 65 and older show manifestations of SVD, such as white matter hyperintensities (WMHs), on brain MRIs1,2. Microvascular function can be measured using 7T MRI3,4, and in earlier work we found that microvascular function was impaired in SVD patients and that lower blood flow velocity in the perforating arteries was associated with higher WMH-volume5,6. To assess if microvascular dysfunction already relates to structural brain changes in a preclinical setting, we studied if perforating artery blood flow velocity and pulsatility were associated with SVD-lesion burden in a general ageing population and if known SVD risk factors were determinants for these measures. We hypothesized that lower blood flow velocity or increased pulsatility were associated with WMH-volume.Methods
All 200 participants were part of The Rotterdam Study7, a prospective population-based cohort study among middle-aged and elderly persons. Participants >60 years of age who had recently undergone 1.5T MRI (with WMH-volume assessment) within the Rotterdam Study context were invited for 7T MRI. Participants with a clinical diagnosis of dementia, previous stroke or major neurological conditions, as well as contraindications for 1.5T and 7T MRI were excluded.7T MRI scans (Philips Healthcare, Best, The Netherlands) were acquired with a 32-channel head coil to assess perforating artery flow and pulsatility as described previously4. 1.5T MRI scans (GE Healthcare, Milwaukee, Wisconsin, USA) with a 8-channel head coil were used to assess WMH volume (ml)7,8. The following risk factors were collected: age, sex, BMI, systolic blood pressure, diastolic blood pressure, pulse pressure, total cholesterol levels, HDL-cholesterol, LDL-cholesterol, triglycerides, glucose, antihypertensives, diabetes mellitus, and smoking.
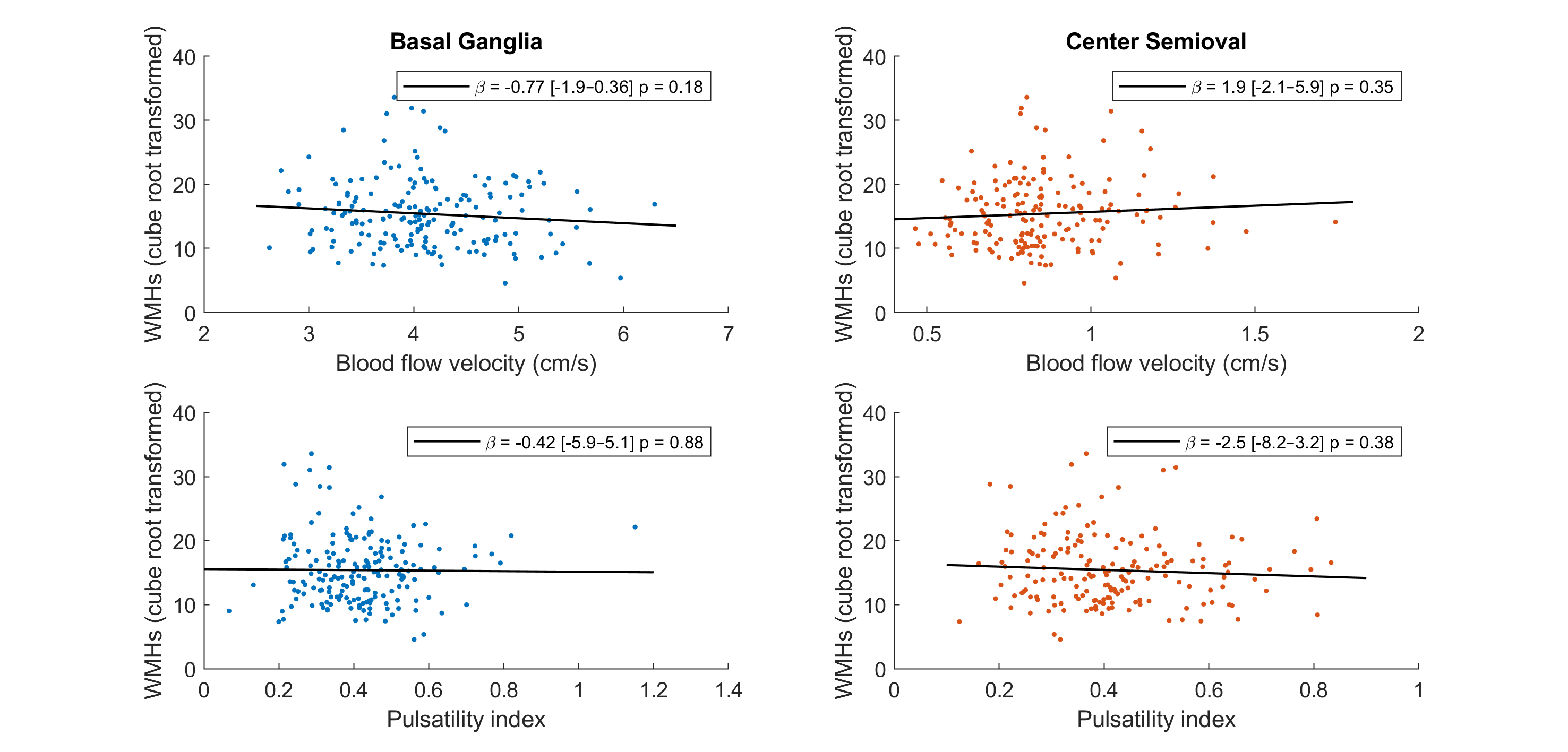
Blood flow velocity and pulsatility index in the perforating arteries of the basal ganglia (BG) and semioval center (CSO) were related to WMHs normalized to intracranial volume and cube-root transformed. The relation between these measures and risk factors were assessed with univariate linear regression or independent samples t-tests for continuous and categorical risk factors, respectively.
Results
After exclusion due to technical problems, patient discomfort, or poor scan quality, 184 BG and 175 CSO scans (mean age=71±5; 44% female) remained in the analysis.None of the blood flow velocity or pulsatility measures in the BG or CSO were significantly associated with whole-brain WMH volume (median WMH volume=0,24% [0,01-2,75%] of intracranial volume) (Figure 1).
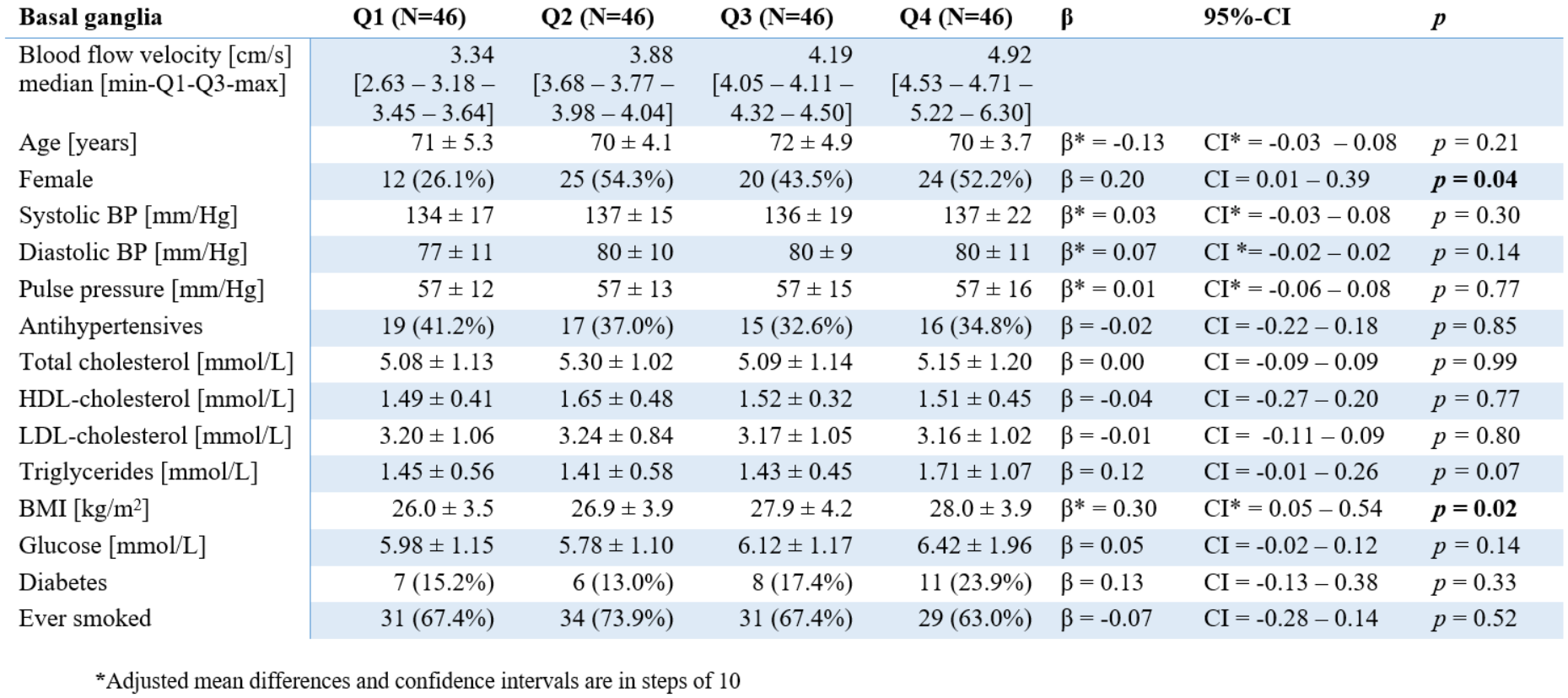
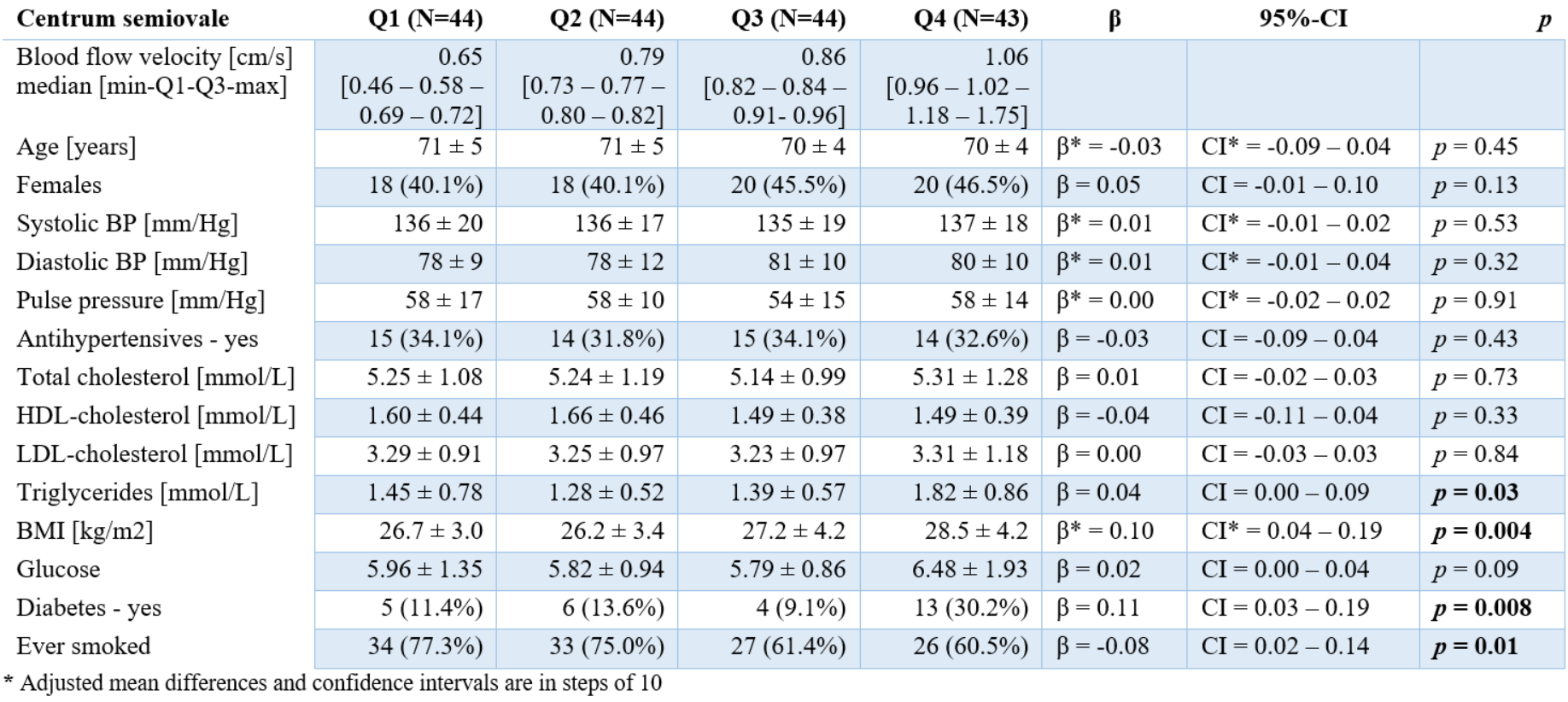
Females had higher velocities than males in the perforating arteries of the BG (mean diff=0.20, p=0.04) (Table 1). Higher BMI was associated with higher velocity in the BG and CSO (BG:β=0.030, p=0.018; CSO:β=0.011, p=0.004). Higher triglycerides (β=0.044, p=0.033), diabetes (mean diff=0.11, p=0.008), and never smoking (mean diff=0.08, p=0.01) were associated with higher velocity in the CSO (Table 2).
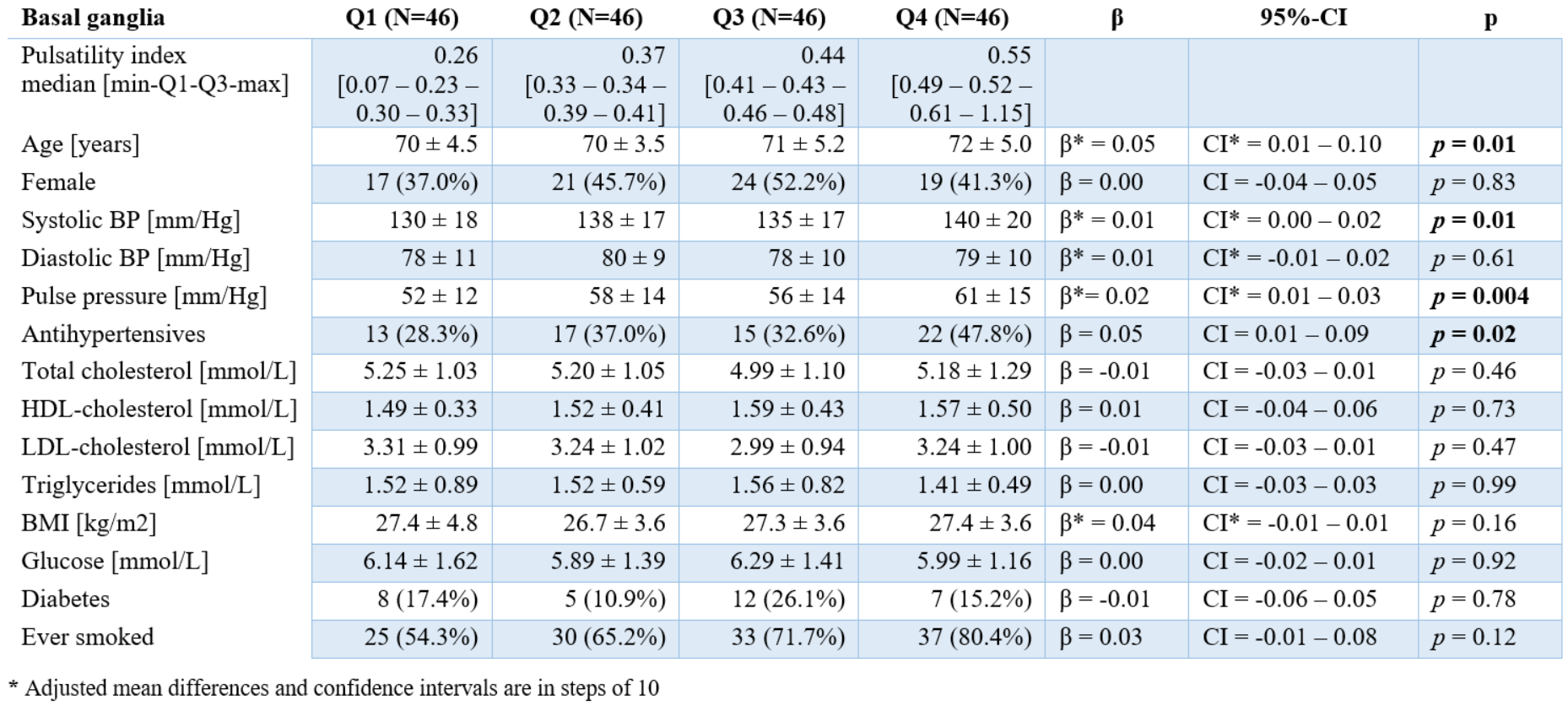
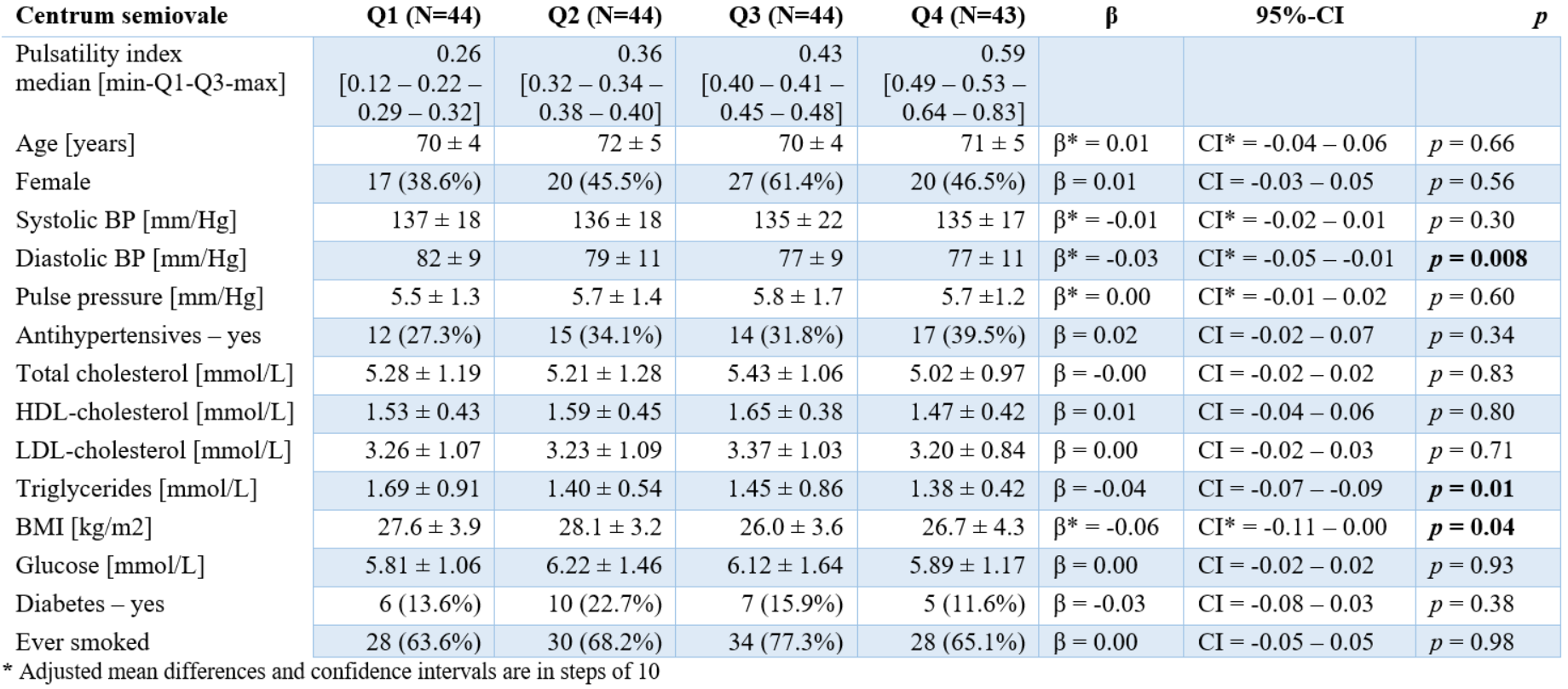
Higher age (β=0.05, p=0.01), systolic blood pressure (β=0.001, p=0.014), and pulse pressure (β=0.002, p=0.004) were associated with higher pulsatility in the perforating arteries of the BG. Participants taking antihypertensives showed significantly higher pulsatility than those who did not (mean diff=0.20, p=0.04) (Table 3).
Lower diastolic blood pressure (β=-0.003, p=0.008), higher BMI (β=-0.006, p=0.042), and triglycerides (β=-0.037, p=0.011) were associated with higher pulsatility in the perforating arteries of the CSO (Table 4).
Discussion
None of the small vessel function measures in the perforating arteries of the BG or CSO were significantly associated with WMHs. Higher blood pressure and BMI were identified as determinants of several small vessel function measures. Higher blood flow velocity was not associated with more WMHs. This could be explained by the relatively low WMH burden in this population when compared to other cohorts of individuals with SVDs5,6. In clinical samples, blood flow velocity was associated with WMHs in sporadic and monogenic forms of SVD.We found higher blood systolic and pulse pressure to be associated with higher pulsatility in the BG, but not in the CSO. This could be explained by the fact that the pulse pressure has been more attenuated further down the vascular tree in the perforating arteries of the CSO than in the perforating arteries of the BG which are more proximal to the larger arteries of the circle of Willis.
An important strength of this study is that we measured small vessel function at the level of the small arterioles using 7T MRI and that we have identified determinants for small vessel function at the level of the these small arterioles. Another strength is the large community-dwelling sample.
Conclusion
Blood flow velocity and pulsatility were not related to SVD burden in the general ageing population. Higher blood pressure and BMI amongst others were identified as determinants of small vessel function.Acknowledgements
We want to thank all study participants for participating in the ZOOM@Rotterdam study. Furthermore, we want to thank all partners of collaborative study between University Medical Center Utrecht and Erasmus Medical Center for their efforts in this study. This work was supported by the European Union’s Horizon 2020 research and innovation programme under grant agreement no. 101032288 (MSCA-IF-GF), Alzheimer’s Association Research Grant (no. AARG-22-972229), ZonMw Memorabel grant (no. 733050817) and Vici Grant (918.16.616) from The Netherlands Organisation for Health Research and Development (ZonMw) to GJB. SDTP and ND are funded by the UMCU Brain Center Young Talent Fellowship 2019.References
1. Wardlaw JM, Smith C, Dichgans M. Small vessel disease: mechanisms and clinical implications. The Lancet Neurology. 2019;18:684–696.
2. Debette S, Schilling S, Duperron MG, et al. Clinical Significance of Magnetic Resonance Imaging Markers of Vascular Brain Injury: A Systematic Review and Meta-analysis. JAMA Neurology. 2019;76:81–94.
3 Zwanenburg JJM, Van Osch MJP. Targeting cerebral small vessel disease with MRI. Stroke. 2017;48(11):3175-3182.
4. Van Den Brink H, Kopczak A, Arts T, et al. Zooming in on cerebral small vessel function in small vessel diseases with 7T MRI: Rationale and design of the “ZOOM@SVDs” study. Cereb Circ - Cogn Behav. 2021;2:100013.
5. Van Den Brink, H., Kopczak, A., Arts, et al. CADASIL Affects Multiple Aspects of Cerebral Small Vessel Function on 7T‐MRI. Annals of Neurology, 2023;93(1):29-39
6. Van Den Brink H, Pham SDT, Siero JCW, et al., Cerebral small vessel function with 7T-MRI in sporadic cerebral small vessel disease: the ZOOM@SVDs study. Manuscript submitted
7. Ikram, M. A., Brusselle, G., Ghanbari, et al. (2020). Objectives, design and main findings until 2020 from the Rotterdam Study. European journal of epidemiology, 35, 483-517.
8. Ikram, M. A., van der Lugt, A., Niessen, et al. (2011). The Rotterdam Scan Study: design and update up to 2012. European journal of epidemiology, 26, 811-824.
Figures