1337
Robust data-driven cerebral artery segmentation using functional magnetic resonance imaging1Weldon School of Biomedical Engineering, Purdue University, West Lafayette, IN, United States, 2Department of Radiology and Imaging Sciences, Indiana University School of Medicine, Indianapolis, IN, United States, 3Department of Biostatistics and Health Data Science, Indiana University, Indianapolis, IN, United States
Synopsis
Keywords: Blood Vessels, Segmentation
Motivation: In this work, we address the challenge of cerebral artery segmentation when time-of-flight (TOF) imaging is unavailable.
Goal(s): Develop an automatic data-driven segmentation of large cerebral arteries.
Approach: Arteries were identified within the fMRI signal by leveraging large pulsation-driven fluctuations.
Results: In the local subjects with TOF images, the approach displayed high levels of agreement with TOF-derived segmentation. Additionally, the segmentation demonstrated high scan-to-scan reproducibility in 430 subjects with four repeated fMRI scans from the HCP aging cohort. Lastly, the segmentation performed robustly across two different scanning protocols supporting its potential to be used for datasets with various acquisition parameters.
Impact: Our robust data-driven approach reliably automatically segments the large cerebral arteries of fMRI datasets. This work enables more accessible large cerebral artery segmentation in existing MRI datasets, independent of TOF images.
Introduction
With the growing interest in neurofluid dynamics, researchers are increasingly studying large cerebral arteries to better comprehend hemodynamics and their link to cerebrospinal fluid dynamics. Currently, time-of-flight (TOF) imaging is the gold standard for cerebral artery segmentation but is unavailable in most existing magnetic resonance imaging (MRI) databases. Notably, functional MRI (fMRI) signals in large cerebral arteries exhibit large pulsation-driven fluctuations1,2,3. We leveraged this behavior and developed a data-driven approach for robust and automatic arterial segmentation. To evaluate its reliability, reproducibility, and robustness across different scanning protocols, we systematically validated the results using a local dataset with TOF images and a public dataset with 430 subjects from the HCP aging cohort.Methods
Data-driven cerebral artery segmentation:We applied a two-step approach to segment the large cerebral arteries using fMRI with simultaneous finger photoplethysmography (PPG) as detailed below.
Step 1: Preliminary artery segmentation
In the first step, we aimed to identify which voxels show pulsatile signal patterns. We excluded the initial 10 volumes from the rs-fMRI signal to reduce T1-relaxation effects and then performed detrending and filtering. This involved the application of a Butterworth high-pass filter with a cutoff frequency of 0.005Hz. Subsequently, we randomly split the fMRI signals into two temporal subsets and retrospectively aligned each to the cardiac cycle resulting in a voxel-wise cardiac-aligned signal pair (Figure 1, a-c). Then we computed the voxel-wise correlation coefficient between each pair. This process was repeated 100 times, and the mean voxel-wise correlation was used to create a robust correlation map. A higher correlation coefficient corresponded to a higher likelihood of arterial regions as these regions expressed increased pulsatility compared to signals from the rest of the brain. We selected voxels with a high correlation coefficient using a data-driven cutoff, which was based on three standard deviations from the mean. These voxels were the preliminary artery region (Figure 1, d-e). By taking the mean waveform of the preliminary artery region, we constructed a global mean waveform that presents pulsatile signal dynamics within the arterial region (Figure 1, f).
Step 2: Refined artery segmentation
In the second step, we applied voxel-wise correlation with the global mean waveform. The voxels showing a high correlation coefficient (>0.5) with the global mean were considered major cerebral arteries (Figure 1, g-h).
Data Acquisition:
All scans were collected on 3T Prisma Siemens scanners. Two cohorts were included: 1) Four local subjects (age 21-36) with four repeated resting state fMRI scans and corresponding TOF images, and 2) 430 subjects (age 36-100) from the HCP aging cohort with two anterior-to-posterior and two posterior-to-anterior phase encoding resting state scans. Detailed scanning parameters for two cohorts are listed in Figure 5. Finger PPG was simultaneously recorded throughout the fMRI acquisitions. All PPG signals were quality-checked by an in-house algorithm before being included in the analysis.
Validation and reproducibility:
Three sets of analyses were conducted to evaluate the overall performance of our artery segmentation results. First, we qualitatively compared our segmentation results of the four local subjects with their TOF images to validate their reliability, where TOF was brought to the fMRI space. Second, we conducted an intraclass correlation (ICC) analysis on the volumes of the artery segmentation masks generated for subjects from the HCP aging cohort to evaluate the segmentation reproducibility. Only subjects with all four replicates who passed a PPG quality check are included in the analysis. Finally, comparing the results from both cohorts, we evaluated the sensitivity of our approach to the variations in imaging protocols.
Results
Our data-driven artery segmentation results strongly agreed with TOF images across all four local subjects in the 3D projection view (Figure 2). Among the HCP aging participants, the intraclass correlation coefficient for the volumes of artery segmentation across four repeated scans was 0.79 (95% CI: 0.761 to 0.816, p<0.001), indicating a high level of reproducibility. Finally, when comparing the segmentation results between local data and the HCP aging data scanned with different temporal and spatial resolutions, our method showed good consistency and reproducibility between diverse imaging protocols as illustrated in Figure 3.Discussion
We developed a robust, automatic, data-driven approach for large cerebral artery segmentation. Our approach revealed a strong agreement with the gold standard (TOF) while demonstrating high reproducibility across MRI spatial and temporal resolutions. Our approach showed its potential as a valuable alternative for cerebral artery segmentations, where TOF imaging data is not accessible. In addition, the adaptability to different MRI resolutions highlighted its broad applicability across various scanning protocols.Acknowledgements
This work was supported by the National Institutes of Health award F30 AG084336, RF1 AG083762. Research reported in this publication was supported by the National Institute On Aging of the National Institutes of Health under Award Number U01AG052564 and by funds provided by the McDonnell Center for Systems Neuroscience at Washington University in St. Louis. The HCP-Aging 2.0 Release data used in this report came from DOI: 10.15154/1520707.
References
1. Hermes, D., Wu, H., Kerr, A. B., Wandell, B. A. Measuring brain beats: Cardiac‐aligned fast functional magnetic resonance imaging signals. Human Brain Mapping. 2023 Jan;44(1):280–294.
2. Voss, Henning U., “Hypersampling of pseudo-periodic signals by analytic phase projection.” Computers in biology and medicine. 2018 July;98: 159-167.
3. Aslan S, Hocke L, Schwarz N, Frederick B. (2019) Extraction of the cardiac waveform from simultaneous multislice fMRI data using slice sorted averaging and a deep learning reconstruction filter. NeuroImage. 2019 September;198: 303–316.
Figures
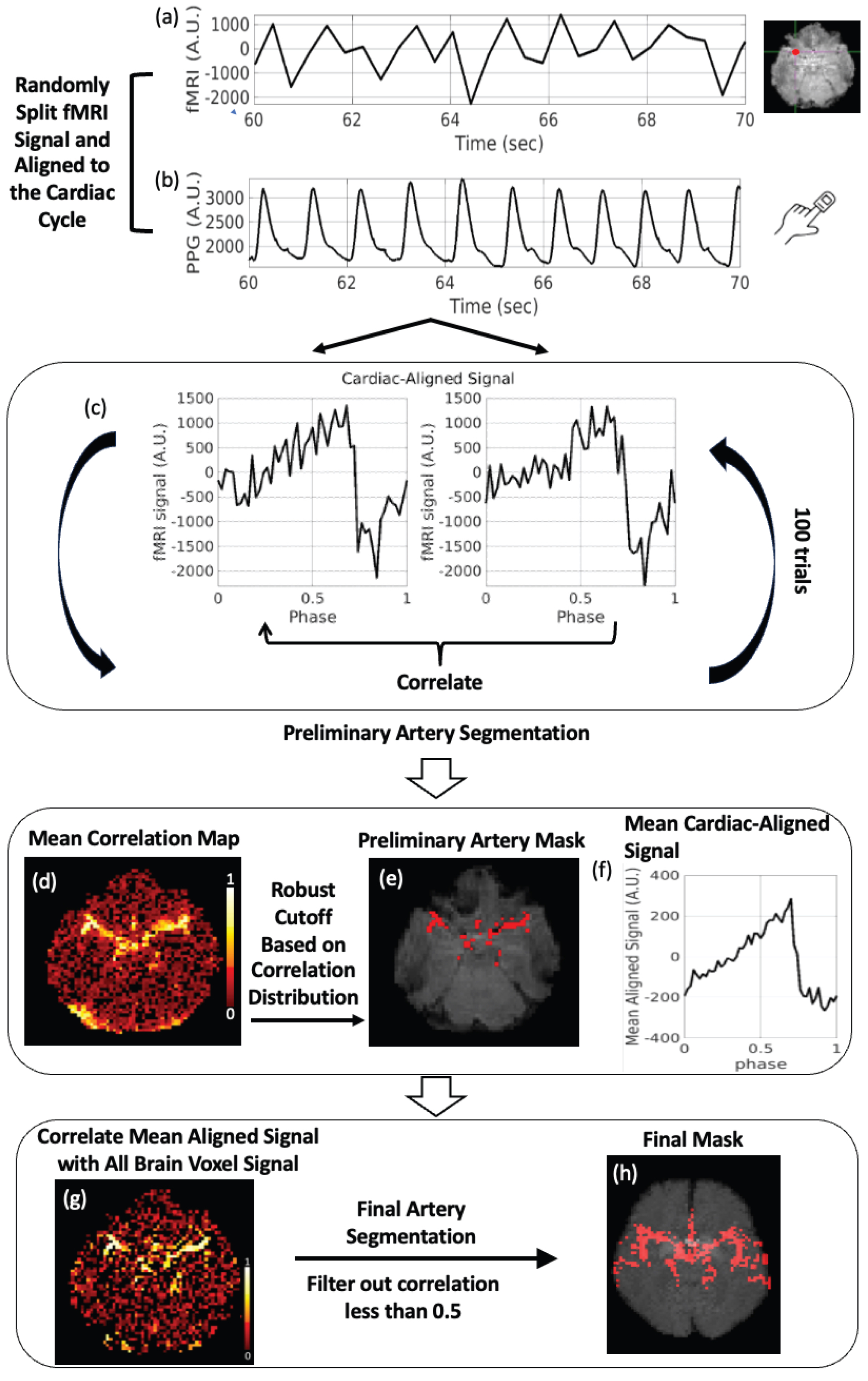
Figure 1. Schematic overview of the segmentation pipeline. (a) A single voxel time-series fMRI signal; (b) Corresponding finger photoplethysmography signal; (c) Cardiac-aligned signal pair from an artery voxel (random splits all fMRI volumes into two temporal subsets); (d) Mean correlation map between signal pairs of 100 splitting iterations; (e) Preliminary artery segmentation, (f) its global mean cardiac-aligned signal; (g) Correlation map with global mean signal, and (h) final segmentation shown as 3D projection.
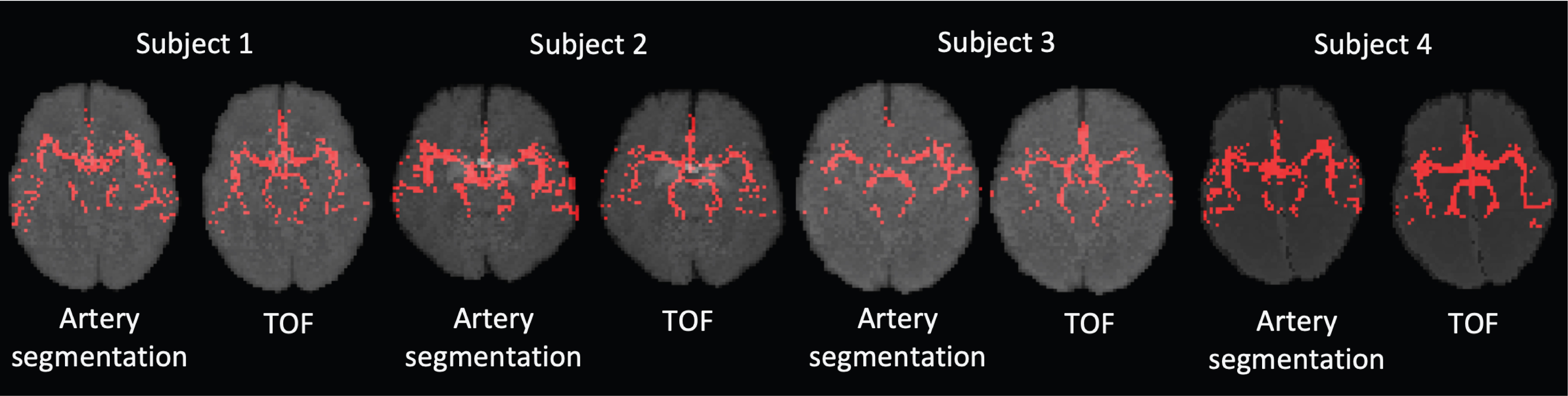
Figure 2. 3D projection of the fMRI-derived artery segmentation (left) in comparison to TOF images, in fMRI space (right) for four local subjects. The ages of the four participants ranged from 21 to 36 years old. Results demonstrated a high agreement between our artery segmentation results and TOF images across all four subjects.
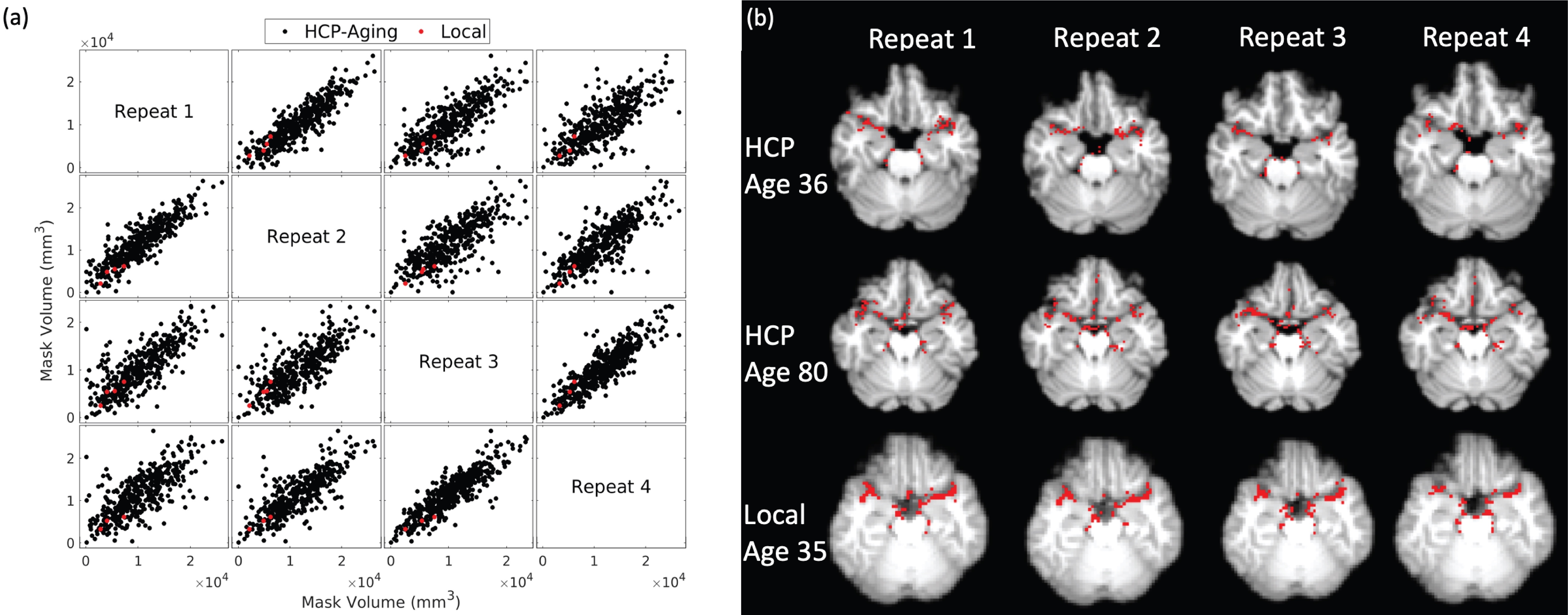
Figure 3. (a) Scatter plots showing good agreement of mask volumes among four repeated scans in the HCP aging (black) and local cohort (red), with ICC = 0.79 (α=0.05, p<0.001); (b) Representative artery segmentation results of slice with middle cerebral artery from one young HCP participant (age 36, top), one old HCP participant (age 80, middle) and one local participant (age 35, bottom) across four repeats. We observed consistent results across subjects of varying ages and different imaging protocols.

Figure 4. Imaging parameters for local subjects and HCP subjects.