1331
Brain structure and glucose metabolism in juvenile and adult-onset Huntington disease: a cross-sectional and longitudinal PET/MR study1Neuroscience Research Center, Department of Medical and Surgical Sciences, Università degli Studi Magna Graecia di Catanzaro, Catanzaro, Italy, 2Nuclear Medicine Unit, Department of Experimental and Clinical Medicine, Università degli Studi Magna Graecia di Catanzaro, Catanzaro, Italy, 3Italian League for Research on Huntington Disease, Rome, Italy, 4IRCSS Casa Sollievo della Sofferenza/CSS-Mendel, Rome/San Giovanni Rotondo, Italy
Synopsis
Keywords: PET/MR, PET/MR
Motivation: Juvenile-onset Huntington Disease (JoHD) represents 4-10% of HD cases, has worse prognosis and psychiatric rather than motor symptomatology, compared to the adult form (AoHD). No study has yet investigated morphological and metabolic changes comparing these two forms with PET-MRI.
Goal(s): Are brain structural and metabolic changes different between patients with JoHD and AoHD? Do they evolve differently?
Approach: PET/MRI was acquired on AoHD and JoHD patients. Cortical and subcortical hybrid characteristics were compared between groups and overtime.
Results: POHD had the most remarkable striatum volume loss at baseline. Interestingly, POHD brain cortex volume was relatively spared at baseline if compared to AOHD patients.
Impact: This study provides first evidence that disease-related degeneration in JoHD first affects subcortical regions, where atrophy is more severe compared to AoHD, and ultimately spreads to the cortex, with faster rates of thinning and glucose metabolism changes compared AoHD.
Introduction
Huntington disease (HD) is caused by an expanded stretch of 36 CAG repeats and more in Huntingtin gene1,2. In 4-10% of HD cases, neurological symptoms may manifest before the age of 21 years, a condition referred to as Juvenile-Onset Huntington Disease (JoHD) (Quarrell – Oxf Univ Press Book 2009). It has been recently pointed out that while the two forms of HD pathology share certain characteristics, JoHD and AoHD also present pathological differences. Histopathological and imaging studies have suggested that damage of subcortical structures might be more severe in JoHD patients compared to the adult forms. Comparative imaging studies between JoHD and AOHD are strongly needed to robustly assess the differential involvement of brain tissues and regions in the two forms to correctly address further experimental therapeutic strategies. Of note, the majority of existing studies focused on structural abnormalities in JOHD, while none investigated glucose metabolism in these patients, especially compared to the adult form.Methods
Five patients with JoHD and 14 patients with adult-onset HD, part of a larger cohort within the RAREST-JHD project, were enrolled in this study. Three JoHD and six adult HD were also assessed longitudinally, with average 12 months follow-up. All participants underwent an extensive neurological and neuropsychological evaluation and the same hybrid [18F] fluorodeoxyglucose (FDG) PET/MRI protocol on a 3T PET/MR scanner (Biograph mMR, Siemens Healthcare, Erlangen, Germany), 40 minutes after the intravenous injection of 185 MBq 18F-FDG. PET acquisition was conducted according to the European Association of Nuclear Medicine procedure guidelines for brain PET imaging. The MRI protocol comprised a 3D T1-weighted magnetization-prepared rapid acquisition gradient-echo sequence (MPRAGE, 176 sagittal planes, 256 × 247 mm2 field of view, voxel size 1 × 1 × 1 mm3, TR/TE/TI 2300/2.34/900 ms, flip angle 8°, TA = 5:12); ii) T2*-weighted single-shot EPI sequence (voxel-size 3.5 × 3.5 × 3 mm3, TR/TE = 2040/30 ms, flip angle = 90°, 300 measurements, FOV 224 x 224, distance factor = 0, TA = 10:20), useful for optimal PET/MRI registration and motion correction. An Ultrashort Time Echo (UTE) sequence was also acquired after the simultaneous PET/fMRI acquisition for attenuation correction. Image postprocessing comprised: 1) Freesurfer recon-all pipeline on all subjects at all timepoints; 2) longitudinal Freesurfer stream to ensure accurate estimate of changes over time; 3) PET images were smoothed using a 4mm full-width half-maximum (FWHM) Gaussian smoothing kernel. Voxel-wise PET standardized uptake value ratios were obtained normalizing each voxel value by the average uptake of whole-brain parenchyma (defined as the sum of GM and WM segmentations, available from FreeSurfer output). Partial volume correction (PCV) was also applied on PET scans using Symmetric Geometric Transfer Matrix (SGTM) in PETSurfer, a set of Freesurfer tools for end-to-end integrated PET-MRI analysis. PV-corrected uptake values were rescaled by the intensity of whole-brain parenchyma. To compare differences in structural and metabolic measures (i.e., cortical thickness, subcortical volume, PVC-uptake), we used analysis of covariance, with age, sex and total intracranial volume included as covariates. Correction for multiple comparisons was performed using False Discovery Rate method (p_adj<0.05). Once the longitudinal processing was performed, annualized changes in different regional metrics were calculated as percentage of baseline value.Results
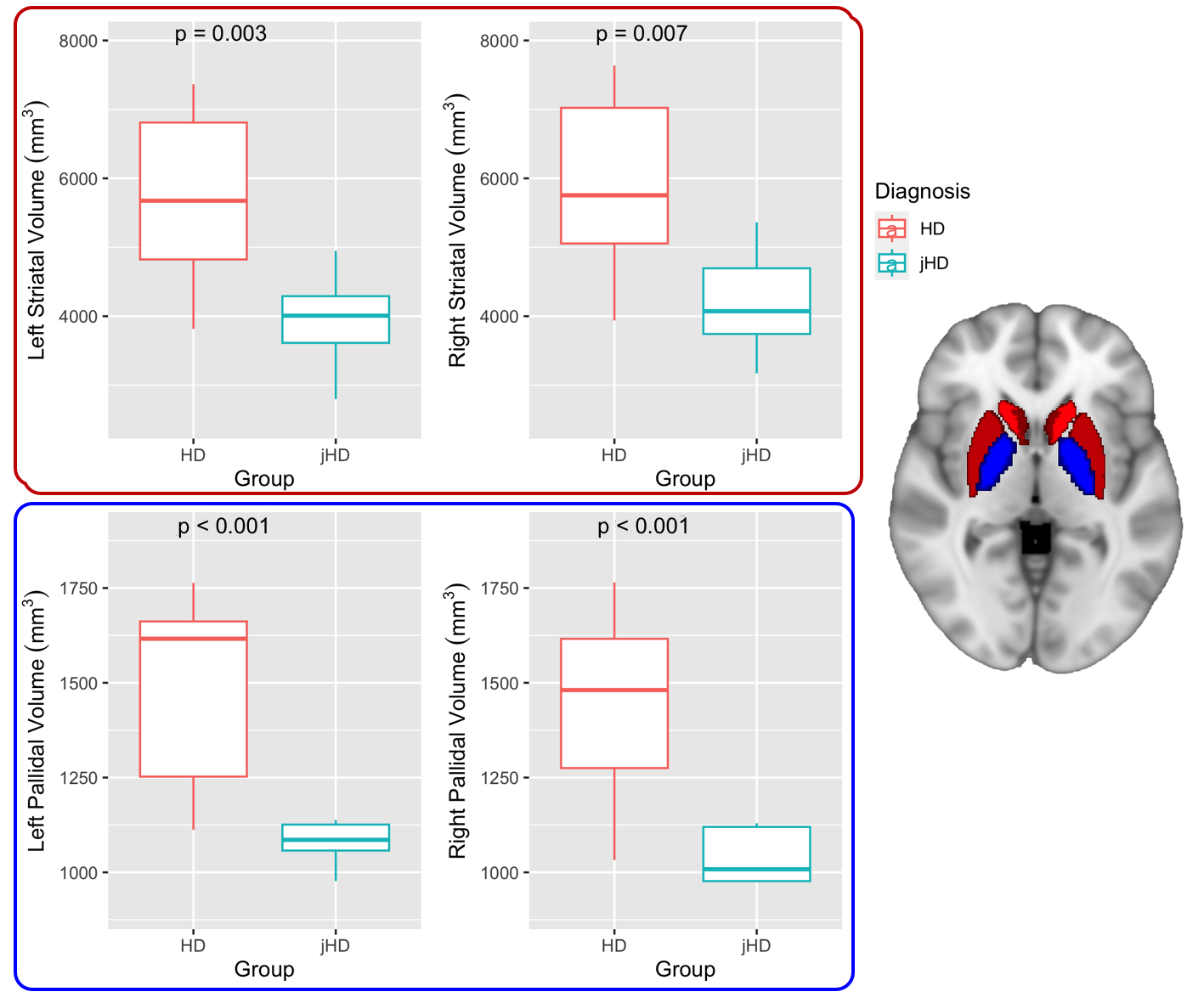
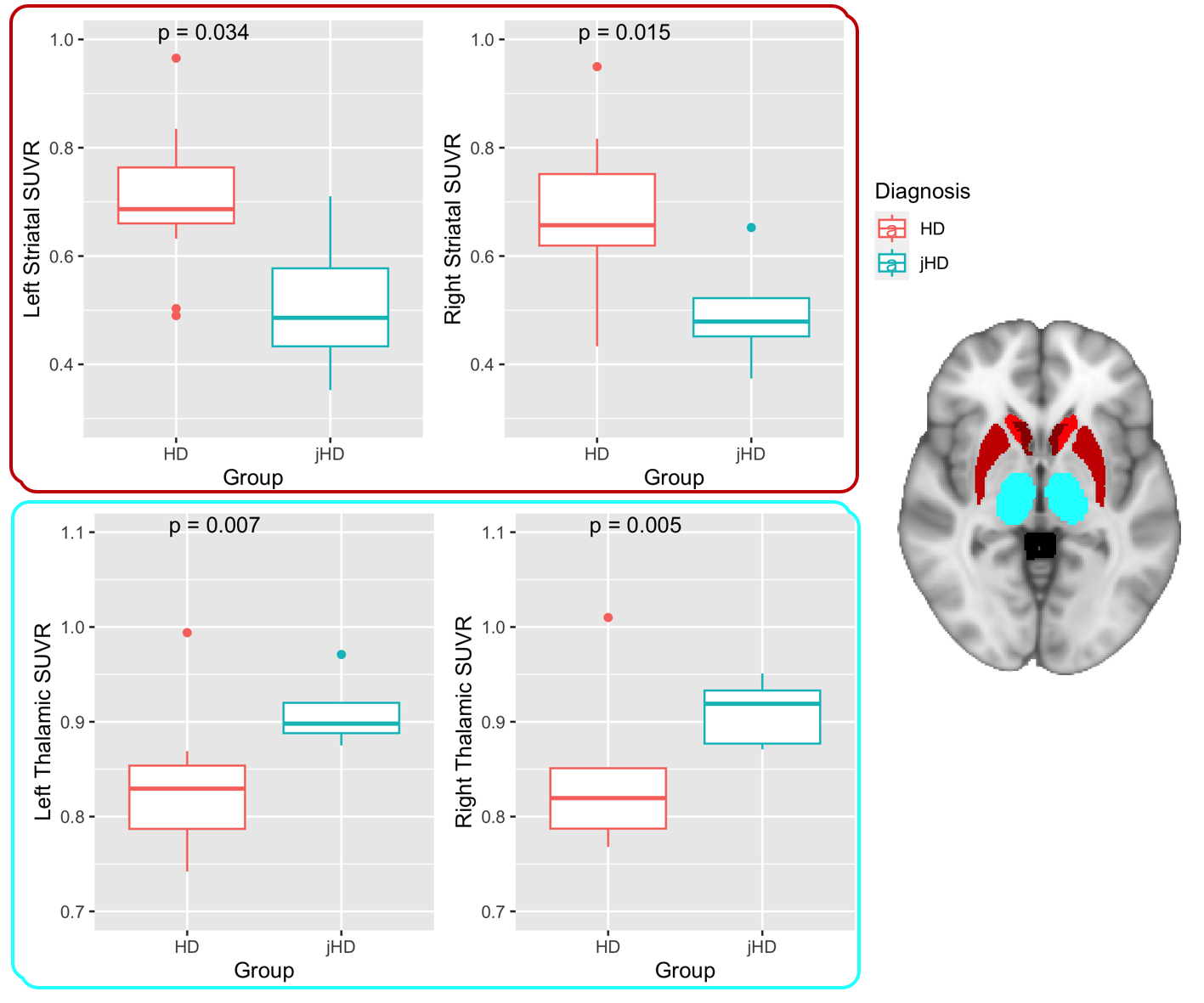
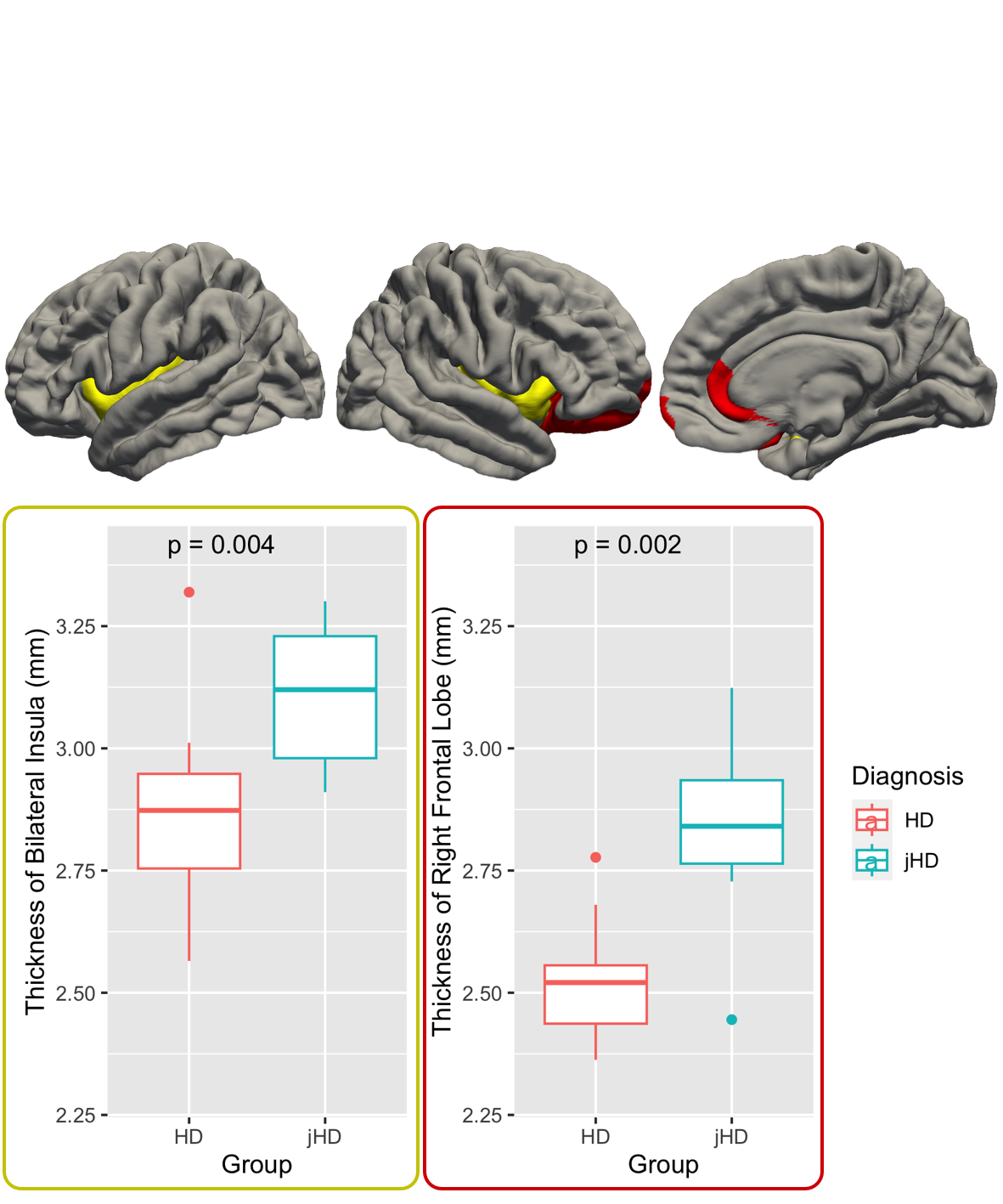
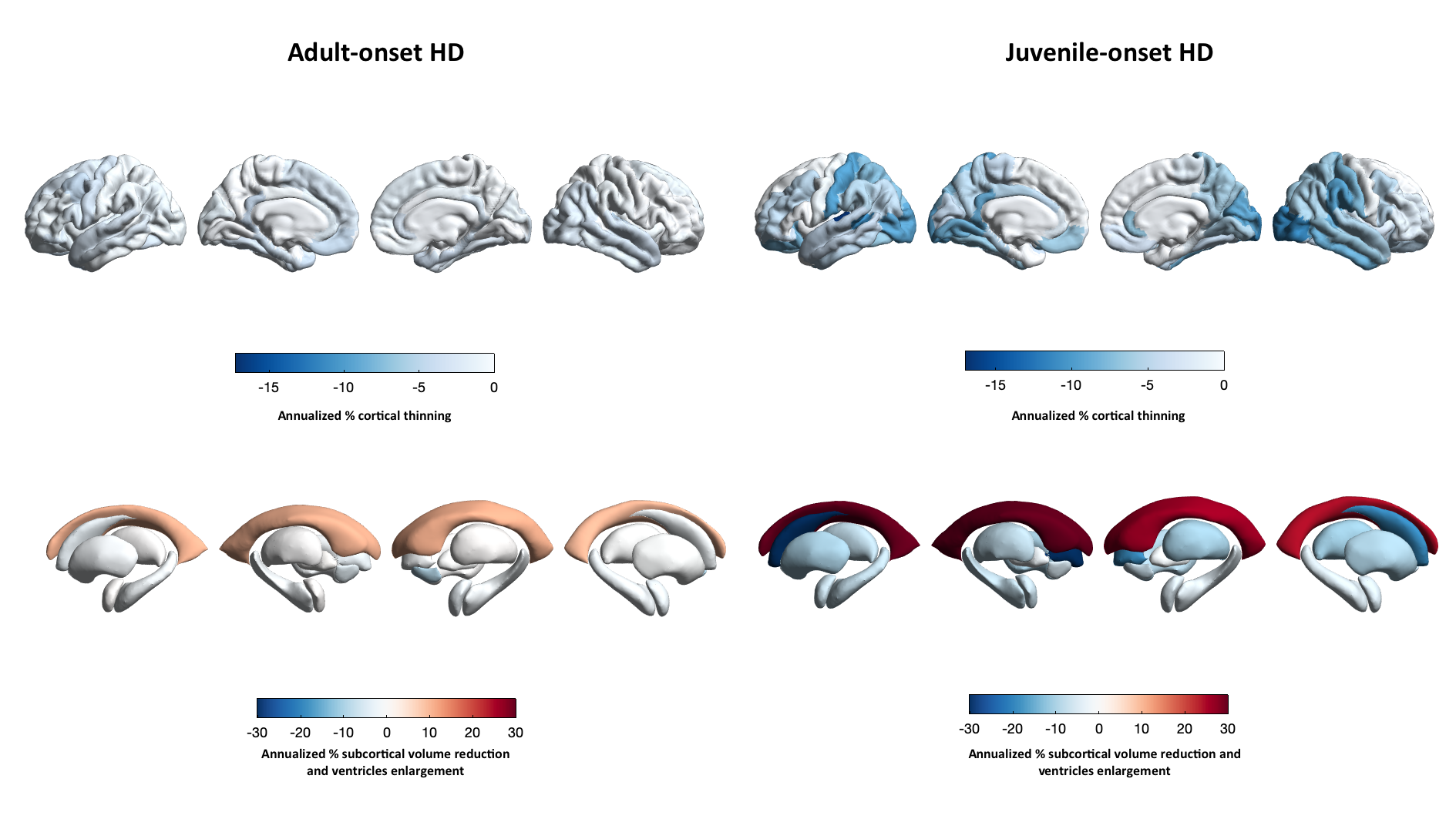
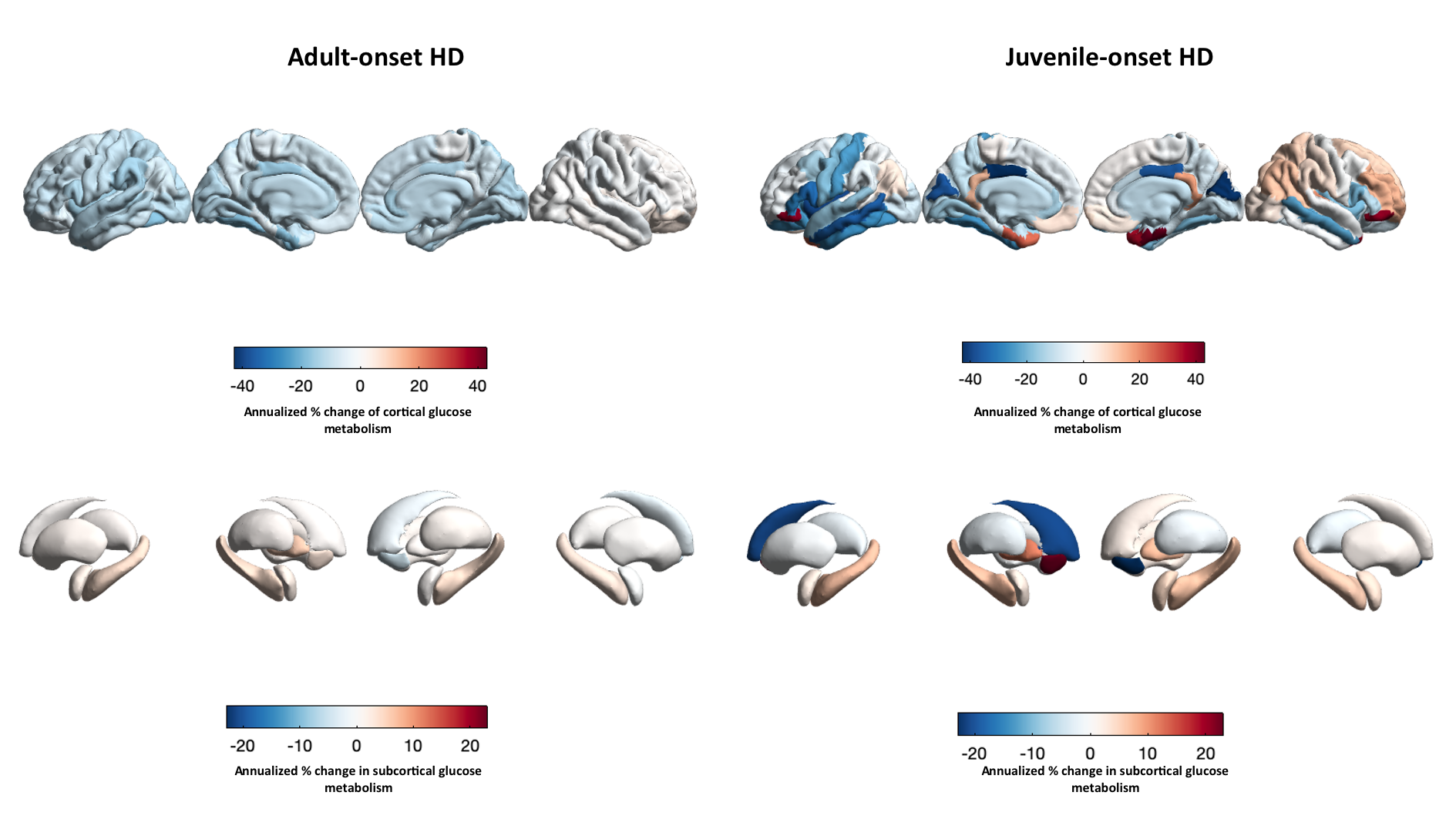
At baseline, no significant difference was detected in total intracranial volume or whole brain FDG-uptake. JoHD showed significant subcortical atrophy compared to adult-onset HD in bilateral striatum and in bilateral globus pallidus (Figure 1). Structural damage in the striatum was paralleled by significant decrease in FDG-uptake values. On the other hand, higher uptake values were found in bilateral thalamus of patients with JoHD compared to AoHD. (Figure 2). When comparing cortical thickness values, patients with AoHD showed significantly decreased values compared to JoHD in bilateral insula, as well as in regions of the frontal lobe, including right rostral-anterior cingulate, frontal pole and lateral orbitofrontal cortex. From the comparison of regional PVC-corrected uptake, we found significantly lower glucose metabolism in patients with AoHD compared to JoHD in left inferior parietal gyrus and left cingulate gyrus, while JoHD showed lower uptake in bilateral enthorinal cortex (Figure 3). Annualized percentage changes over the whole brain are reported below for the two groups of patients separately (Figures 4-5).Discussion
Taken together, these results suggest that disease-related degeneration in JoHD first affects subcortical regions, where atrophy is more severe at baseline but also in longitudinal observations compared to the adult form, and ultimately spreads to the cortex, with faster rates of thinning and glucose metabolism changes compared to adult-onset HD. Due to the small sample size of the longitudinal cohort, however, these results must be considered exploratory.Acknowledgements
No acknowledgement found.References
[1] Ghosh R., Tabrizi S.J. Clinical Features of Huntington's Disease. Adv Exp Med Biol, 2018, 1049, 1-28. doi:10.1007/978-3-319-71779-1_1
[2] Quarrell, O.W.J., Brewer, H.M,, Squitieri, F., Barker, R.A., Nance, M.A., Landwehrmeyer G.B., eds. Juvenile Huntington’s disease. Oxford: Oxford University Press, 2009
Figures