1326
Preliminary investigation of BOLD dependence on EEG-TMS using a closed-loop TMS-EEG-fMRI setup1A.I. Virtanen Institute for Molecular Sciences, University of Eastern Finland, HELSINKI, Finland, 2Dept. of Neuroscience and Biomed. Engineering, Aalto University, Espoo, Finland, 3Department of Psychiatry & Behavioral Sciences, Stanford University, Stanford, CA, United States, 4Sunnybrook Research Institute, University of Toronto, Toronto, ON, Canada, 5Centre of Addiction and Mental Health, University of Toronto, Toronto, ON, Canada, 6A.I. Virtanen Institute for Molecular Sciences, University of Eastern Finland, Kuopio, Finland
Synopsis
Keywords: Hybrid & Novel Systems Technology, Multimodal, TMS, EEG, fMRI
Motivation: The motivation for this research study is to improve the efficacy of transcranial magnetic stimulation.
Goal(s): The specific goals of this study are to establish a closed-loop TMS-EEG-fMRI system and to investigate brain state-dependent EEG-TMS responses in relation to concurrent fMRI measurements.
Approach: 150 single TMS pulses are delivered while monitoring TMS-elicited network activity using interleaved fMRI acquisition. Data processing involves extracting EEG phase information, preprocessing of fMRI data, and statistical analysis using SPM12.
Results: Significantly increased fMRI signal was detected in the M1 and SMA under specific EEG phase conditions. These results illustrate the relationship between TMS, EEG phases, and BOLD responses
Impact: The results of this study have important implications for the field of non-invasive brain stimulation and neuroimaging. The development of a closed-loop TMS-EEG-fMRI system holds the potential to revolutionize the treatment of various brain disorders by personalizing TMS interventions.
Introduction
Transcranial magnetic stimulation (TMS) is a powerful tool for non-invasive brain stimulation, with applications ranging from research to diagnostics to treatment of psychiatric and neurological disorders. Currently, TMS is applied the same way to all individuals without personalization, leading to inconsistent treatment outcomes [1]. One way to personalize the treatment and increase its effectiveness is to use concurrent neuroimaging techniques to guide the procedure. By combining TMS with real-time neuroimaging modalities such as functional magnetic resonance imaging (fMRI) and electroencephalography (EEG), we aim to customize TMS treatment by optimizing stimulation timing, targeting, and intensity uniquely for each individual. In this abstract, we present our experimental setup toward closed-loop TMS–EEG–fMRI, as well as our signal-processing pipeline. We also show our preliminary results for studying brain state-dependent TMS–EEG responses and how they relate to the BOLD activity measured concurrently with fMRI.Methods
EXPERIMENTAL SETUPOur setup (Figure 1) consists of MRI-compatible EEG amplifiers (NeurOne Tesla, Bittium, Finland), TMS stimulator (MagPro R30, MagVenture Inc., Alpharetta, GA, USA) and TMS coil (MagVenture MRi-B91). The EEG amplifiers and TMS coil are positioned within the MRI scanner (3T Siemens MAGNETOM Skyra) bore. The TMS coil is attached to a specially designed coil holder arm [2] and is integrated with a slightly curved custom-made 8-channel MRI surface head coil array [3]. The TMS stimulator is placed inside the MRI technical room and is connected to the TMS coil via an extended power cable. The subject is equipped with a 64-channel EEG cap (Easycap GmbH, Germany) that features seven custom-made carbon-wire-loops (CWLs) leveraged in EEG artifact suppression [6]. The EEG cap is connected to the amplifiers, which then transmit the signal from the MRI room to the EEG main unit. Unprocessed EEG is streamed to a real-time processing unit (BOSS device) [4] operating on a modified firmware capable of suppressing MRI-induced artifacts and timing TMS to a predefined oscillatory brain state of EEG [5].
DATA ACQUISITION
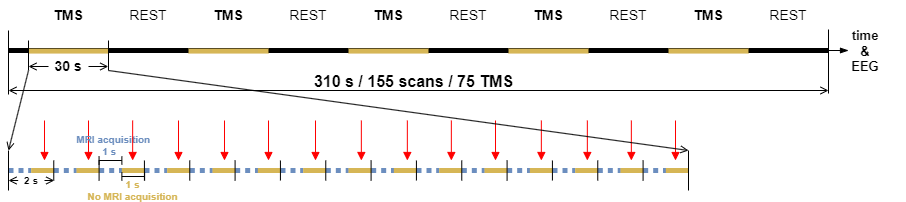
150 single TMS pulses were delivered to the left primary motor cortex (M1) of a right-handed healthy volunteer while the TMS-elicited network activity was monitored with interleaved fMRI acquisition. Functional images were acquired with a gradient-echo echo-planar-imaging (GE-EPI) sequence (TR = 2000 ms; TE = 26.0 ms; voxel resolution 2×2×2 mm3; flip angle 90°). Each TMS–fMRI run consisted of five 30-second “TMS” and “REST” blocks. Each TR included a silent 1-second gap during which a TMS pulse was delivered. 64-channel EEG was recorded at 20 kHz throughout the experiment. TMS delivery with fMRI acquisition is demonstrated in Figure 2.Figure 2: TMS delivery with fMRI acquisition.
DATA PROCESSING
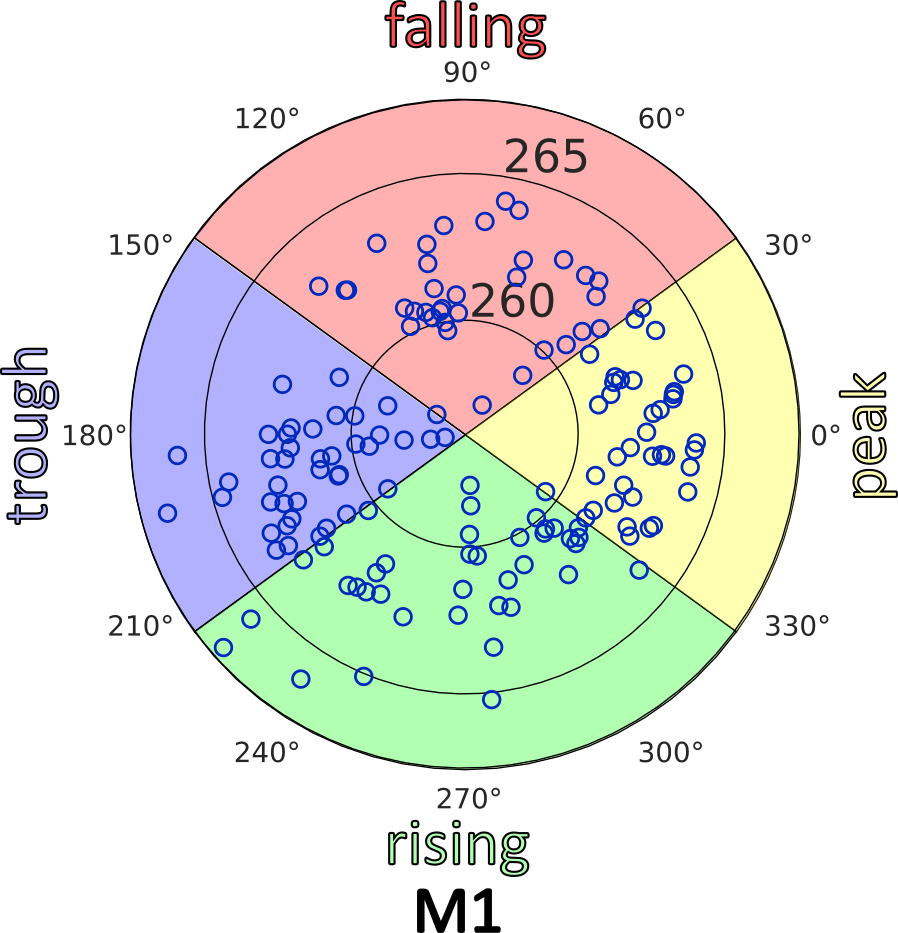
The phase of spatially filtered (surface Laplacian centered on C3 electrode) sensorimotor mu rhythm at each TMS onset was extracted and divided into four parts: peak, trough, falling, and rising (see Figure 4). fMRI images were slice-time and motion corrected, spatially smoothed, coregistrated with anatomical T1 images, and analyzed with SPM12 [7]. The design matrix included four regressors, each corresponding to a different EEG phase condition. Additionally, realignment parameters were included in the model as nuisance regressors.
Results
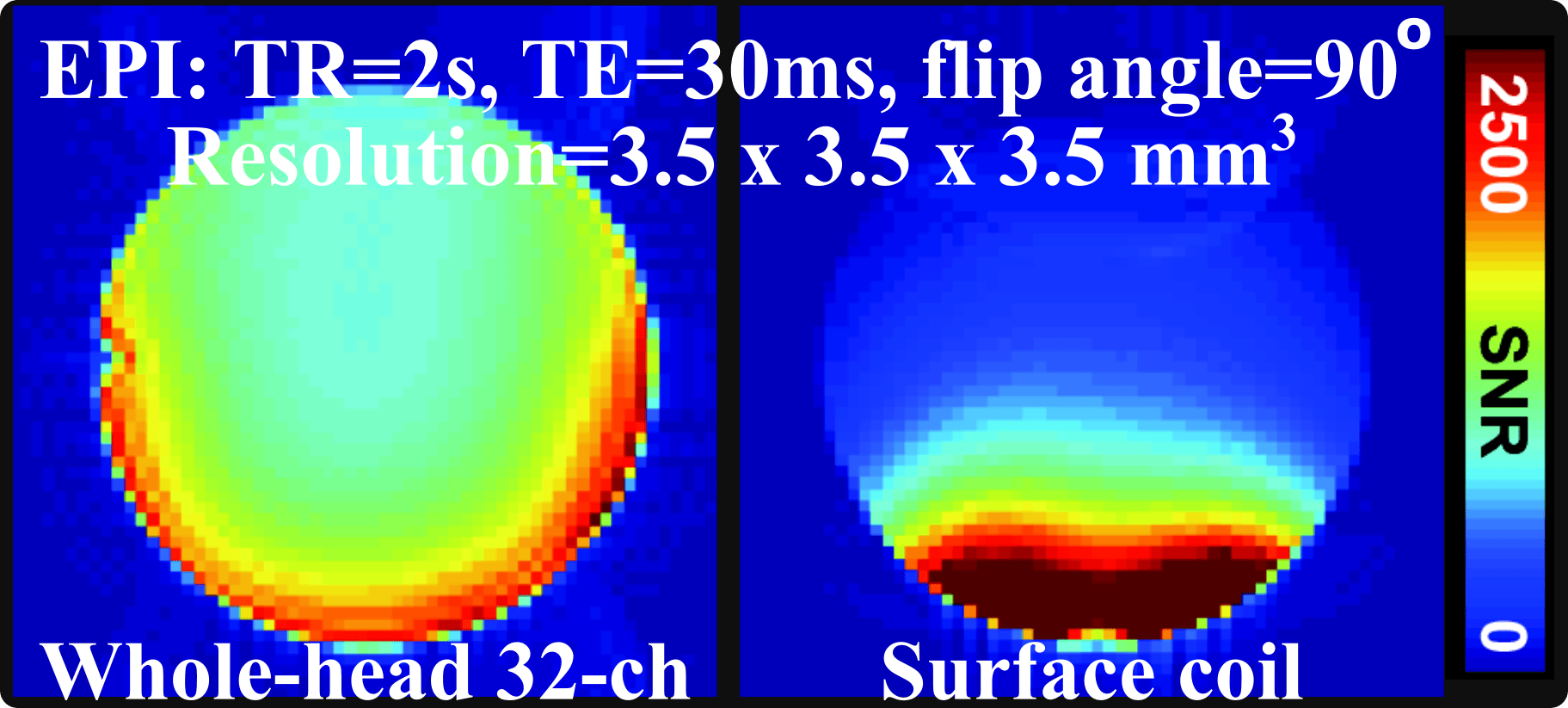
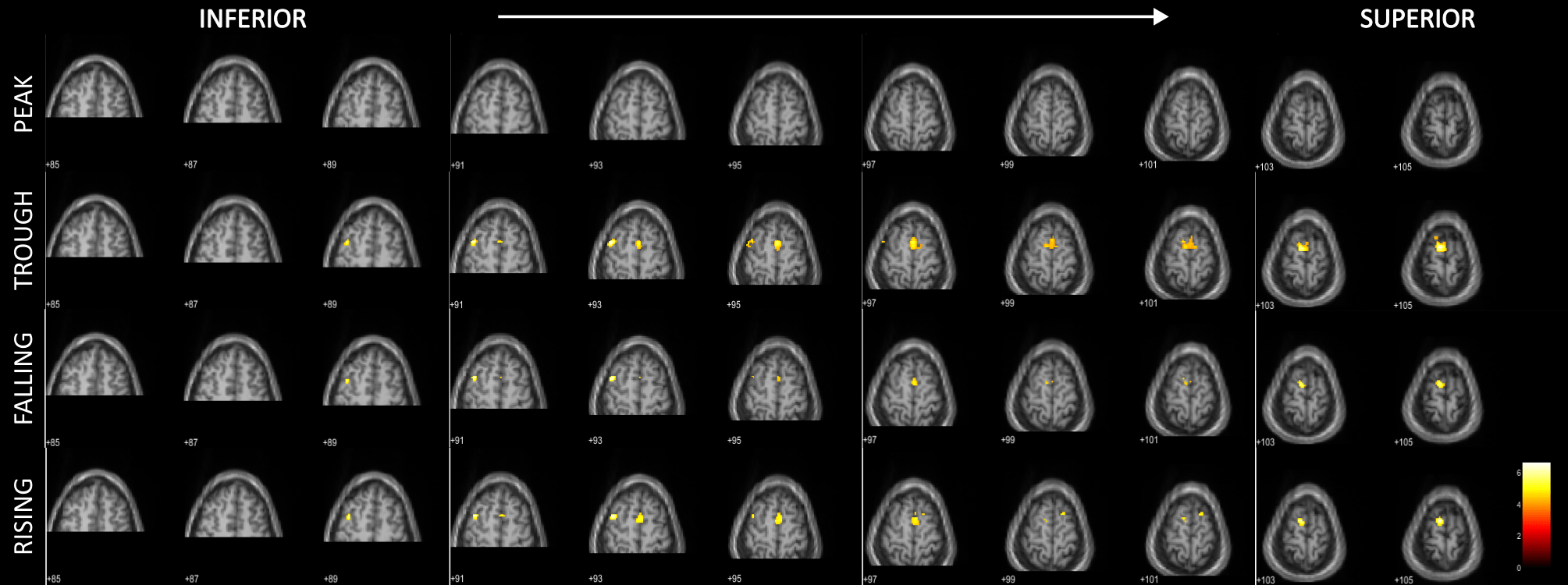
Figure 3 shows that the 8-channel surface coil yielded a superb signal-to-noise ratio (SNR) under the stimulated regions compared to the 32-channel whole-head coil array. The quality of the EEG data collected with CWL was sufficient to study the EEG phase [4]. During TMS, a significantly increased (p < 0.05 FWE) fMRI signal was detected in M1 and supplementary motor area (SMA) under the trough, falling, and rising phase conditions. However, the activation varied in strength (Figure 4) and morphology (Figure 5) across the conditions: TMS applied on the trough of EEG signal elicited broader network activity in SMA and M1 compared to other conditions. TMS applied during the EEG peak condition did not elicit significant activation (p < 0.05 FWE) in M1 nor SMA, which has been reported as a low-excitability state in earlier TMS–EEG studies with motor-evoked potentials (MEP) [4]. The activated regions of M1 and SMA matched the activated sensorimotor network during a voluntary finger-tapping experiment.Conclusion
Despite the challenges in building a concurrent TMS–EEG–fMRI setup, we successfully established a working multimodal system. In the future, we aim for full real-time integration including acquisition and data processing of fMRI and EEG as well as TMS delivery. In addition, we are currently expanding our study by increasing the number of subjects to explore the influence of EEG features on TMS-elicited BOLD responses thoroughly. This technical endeavor could lead to development of novel diagnostic methods and treatment strategies for a variety of brain disorders.Acknowledgements
This project is funded by Research Council of Finland (grant agreements #348631 and #353798). Additionally, this project received support from ERC-funded ConnectToBrain-project.References
[1] Loo, C. K., & Mitchell, P. B. (2005). ”A review of the efficacy of transcranial magnetic stimulation (TMS) treatment for depression, and current and future strategies to optimize efficacy”. Journal of Affective Disorders, 88(3), 255–267.
[2] Lee, H. J. et al. (2023). “Design of coil holder for the improved maneuvering in concurrent TMS-MRI”. Brain Stimulation.
[3] Wu P.-Y. et al. (2015). “A 10-channel TMS-compatible planar RF coil array for human brain MRI at 3T”. Intl. Soc. Mag. Reson. Med., 625.
[4] https://sync2brain.com/
[5] Zrenner, C. et al. (2018). “Real-time EEG-defined excitability states determine efficacy of TMS-induced plasticity in human motor cortex”. Brain Stimulation, 11(2), 374–389.
[6] Laurinoja, J. et al, (2023). “Accuracy of EEG-phase estimation for closed-loop brain stimulation inside the MRI device”. Brain Stimulation, 16(1), 302–303.[7] http://fil.ion.ucl.ac.uk/spm/
Figures