1320
A Dynamic PVA Cryogel based Cardiac Phantom for 3D Temperature Validation of Radiofrequency Ablation1Magnetic Detection and Imaging group, TechMed Centre, University of Twente, Enschede, Netherlands, 2Cardiovascular and Respiratory Physiology group, TechMed Centre, University of Twente, Enschede, Netherlands, 3Multi-Modality Medical Imaging group, TechMed Centre, University of Twente, Enschede, Netherlands, 4Robotics and Mechatronics group, University of Twente, Enschede, Netherlands, 5Department of Cardiology, Amsterdam University Medical Centers, Amsterdam, Netherlands
Synopsis
Keywords: Phantoms, Phantoms, Validation, Temperature mapping, Dynamic
Motivation: MRI-guided radiofrequency ablation of cardiac arrhythmias holds promise to monitor the lesion formation process, however lacks validation tools.
Goal(s): To develop a phantom for quantitative validation of catheter ablation procedures.
Approach: In this study, a phantom composed of polyvinyl alcohol (PVA) with temperature sensitive properties has been developed for validation of the attained ablation temperature.
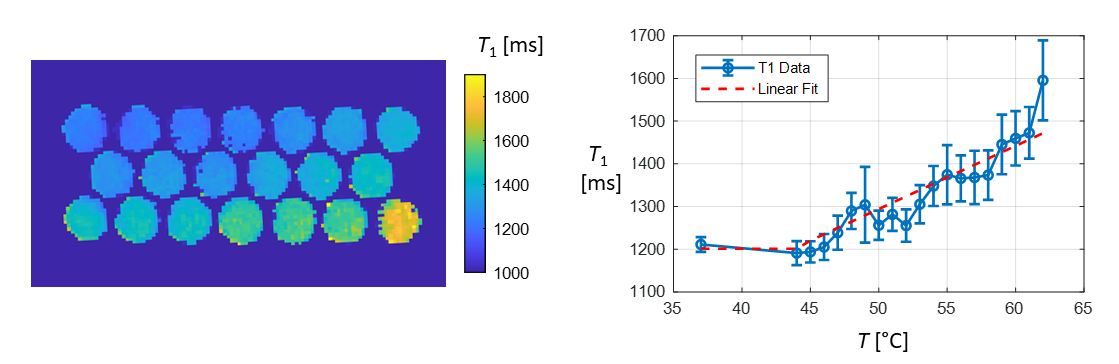
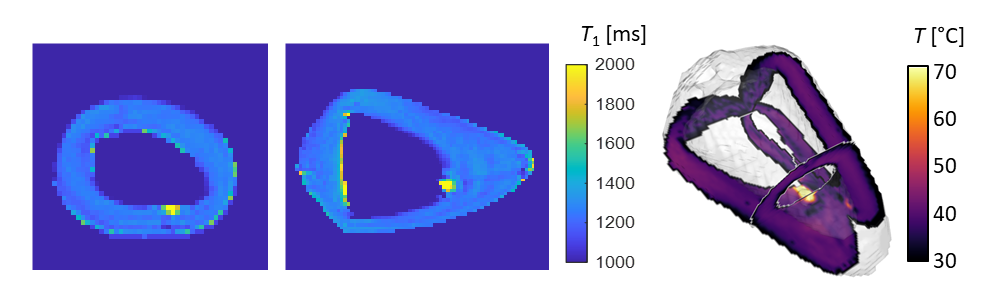
Results: Post-ablation T1 maps were acquired and converted into temperature maps, based on the characterization of the reference phantoms.
Impact: This work demonstrates a validation phantom for temperature validation after radiofrequency ablation procedures. This can offer an effective tool for MR methods development as well as procedural training, shortening procedural times and improving patient outcomes.
Introduction
A cornerstone for the treatment of cardiac arrhythmias is radiofrequency (RF) catheter ablation, although recurrence rates remain relatively high.1 Interventional cardiac MR (iCMR) shows promise to provide real-time intra/periprocedural feedback on the lesion formation process.2 Validation is however limited to either static models or relatively complex in vivo animal studies, which become increasingly more limiting due to increasing costs as well as regulatory and ethical implications.In this work, we introduce a dynamic cardiac phantom that allows quantitative validation of RF ablation procedures. By leveraging the temperature-sensitive MR relaxation properties of polyvinyl alcohol (PVA) cyrogel, which change permanently after heating,3 the attained ablation temperature is imprinted into the phantom material and can be quantified post-ablation by means of basic T1 mapping.
Methods
A simple ventricle phantom was designed in the shape of a paraboloid with 1 cm wall thickness and the corresponding mold was 3D printed using polylactic acid (PLA).4 A 10 wt% mixture of fully hydrolized PVA (CAS number 9002-89-5, Sigma Aldrich, The Netherlands) in water was heated to 90°C with continuous stirring. NaCl was added up to 0.15 wt% to adjust the electrical conductivity of the phantom. The solution was cooled down to room temperature and poured into the ventricle mold. A separate set of 20 reference spheres were cast to characterize the relation between temperature and T1. All phantoms were subjected to two freeze-thaw cycles (-20°C/+20°C) with transitions every 24 hours to initiate the cryogel cross-linking process.Each of the sphere phantoms was individually heated to a temperature ranging from 37 °C to 62 °C using a temperature-controlled water bath and a thermo-couple to record the final temperature. An RF ablation lesion was created using a conventional RF ablation catheter (Biosense Webster Inc., Irvine, USA) after placing the ventricle phantom in saline.
T1 mapping was performed using a 1.5T MRI system (Aera, Siemens Healthineers, Erlangen, Germany) using a 3D inversion-recovery FSE sequence (TR/TE = 1500/80 ms, TI = 200-1400 ms in steps of 300 ms, Field-of-View (FoV) = 288×288×48 mm, isotropic voxel size = 1.5 mm). The data obtained in the phantom spheres were fitted to a linearized relation between T1 and temperature. Finally, cine MRI data were obtained while the ventricle phantom underwent cyclic deformation, driven by a pulsatile pump (SuperPump, Vivitro, Victoria, Canada) using a retrospectively triggered bSSFP sequence (TR/TE = 2.2/1.1 ms, FoV = 340×340 mm, voxel size = 1.7×1.7 mm, slice thickness = 8 mm, flip angle = 58°).
Results
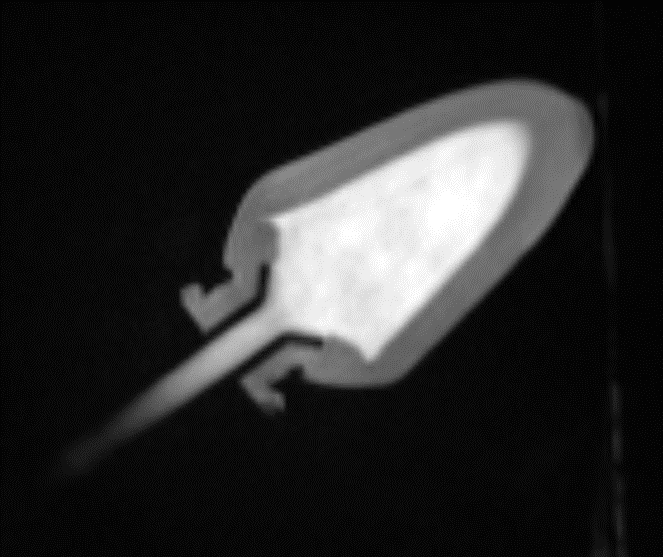
Figure 1 shows the geometrical design of the ventricle model. The material characterization results are shown in figure 2 where an increase in T1 relaxation time can be observed from approximately 1200-1600 ms corresponding to temperatures between ~45 °C and 62 °C.Figure 3 shows the post-ablation T1 map and corresponding temperature results in 3D, showing the localized ablation lesion. A bSSFP image without pulsatile deformation is shown in Figure 4, showing realistic contrast between the lumen and phantom wall. Finally, dynamic cine imaging is illustrated in Figure 5 showing realistic flow artefacts within the lumen of the model.
Discussion
In the current work, the temperature-sensitive T1 properties of PVA have been exploited as a permanent marker for the attained ablation temperature in RF ablation procedures. PVA offers desirable mechanical properties such as durability and elasticity for constructing cardiovascular phantoms.5 As the native T1 (~1100 ms) is close to physiological values, the proposed phantom material offers a suitable model for MR sequence development.The presented approach offers full control over the model and design parameters, allowing for reproducibility studies and the inclusion of patient-specific features such as cardiac arrythmias or anatomical geometries.6 Future studies include performing the RF ablation procedure under MR guidance to corroborate the temperature maps directly with real-time MR thermometry data.
Conclusion
A unique dynamic cardiac phantom has been developed and evaluated for quantitative temperature validation after RF ablation procedures. This offers a testbed for the development of new treatment strategies and peri-procedural monitoring, as well as providing a tool for training programs aimed at iCMR procedures.Acknowledgements
The authors would like to acknowledge the support of prof.dr. C.P. Allaart and the AmsterdamUMC cath lab team with performing the RF ablation procedure.References
1. Calkins H, Hindricks G, Cappato R, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm 2017;14:e275–e444. doi: 10.1016/J.HRTHM.2017.05.012.
2. Toupin S, Bour P, Lepetit-Coiffé M, et al. Feasibility of real-time MR thermal dose mapping for predicting radiofrequency ablation outcome in the myocardium in vivo. Journal of Cardiovascular Magnetic Resonance 2017;19:1–12. doi: 10.1186/S12968-017-0323-0/FIGURES/6.
3. Lukas LA, Surry KJM, Peters TM. Temperature dosimetry using MR relaxation characteristics of poly(vinyl alcohol) cryogel (PVA-C). Magn Reson Med 2001;46:1006–1013. doi: 10.1002/MRM.1288.
4. Dieringer MA, Hentschel J, De Quadros T, Von Knobelsdorff-Brenkenhoff F, Hoffmann W, Niendorf T, Schulz-Menger J. Design, construction, and evaluation of a dynamic MR compatible cardiac left ventricle model. Med Phys 2012;39:4800–4806. doi: 10.1118/1.4736954.
5. Tibamoso-Pedraza G, Navarro I, Dion P, Raboisson MJ, Lapierre C, Miró J, Ratté S, Duong L. Design of heart phantoms for ultrasound imaging of ventricular septal defects. Int J Comput Assist Radiol Surg 2022;17:177–184. doi: 10.1007/S11548-021-02406-0/TABLES/2.
6. Morais P, Tavares JMRS, Queirós S, Veloso F, D’Hooge J, Vilaça JL. Development of a patient-specific atrial phantom model for planning and training of inter-atrial interventions. Med Phys 2017;44:5638–5649. doi: 10.1002/MP.12559.
Figures