1304
Quantification of extravascular lung water using a dual contrast extracellular volume approach1Cardiovascular Branch, Division of Intramural Research, National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, MD, United States, 2Department of Radiology, Case Western Reserve University and University Hospitals, Cleveland, OH, United States
Synopsis
Keywords: Novel Contrast Mechanisms, Multi-Contrast, Lung water, Heart failure, Translational studies
Motivation: Extravascular lung water is a feature in heart failure. Current lung water MRI methods cannot distinguish between intravascular and extravascular fluid, and therefore cannot fully isolate the pathology.
Goal(s): To isolate and quantify extravascular lung water by developing a dual-contrast extracellular volume (ECV) method, leveraging different extracellular compartmentalization of gadolinium and ferumoxytol.
Approach: We calculated ECVextravascular=ECVgadolinium-ECVferumoxytol from lung T1-maps with native, gadolinium and ferumoxytol contrast. Validation was performed in porcine models of increased extravascular and intravascular lung water.
Results: As expected, ECVextravascular differed between baseline and the extravascular intervention (27±4.1% vs 32±1.6%, p=0.005), but not for the intravascular model (22±4.7% vs 22±4.4%, p=0.91).
Impact: Dual contrast extracellular volume measurements, leveraging the different compartment uptakes of gadolinium and ferumoxytol contrasts, is a promising method for extravascular lung water quantification, and may enable mechanistic studies of lung water accumulation in patients with dyspnea.
Introduction
Dyspnea caused by cardiogenic pulmonary edema, also known as lung water, is a key feature in heart failure. The lung water accumulates due to a pressure-driven fluid leakage from the intravascular space into the extravascular pulmonary interstitium. Proton density weighted (PDw) MRI has recently emerged as a technique to quantify lung water, and is a promising method to monitor and predict outcomes in heart failure1–6. PDw MRI is, however, not capable of distinguishing between intravascular and extravascular lung water compartments1–3,6.Therefore, we aim to develop a method to isolate and quantify the extravascular lung water compartment through a dual contrast extracellular volume (ECV) approach, where we leverage the different inherent extracellular compartment uptakes of gadolinium, a chelate which accumulates in both the intravascular and extravascular spaces7, and ferumoxytol, an iron-oxide nanoparticle which accumulates solely within the intravascular space8. We test our hypothesis, that the extravascular lung ECV component can be derived in porcine models with experimentally induced increases in extravascular and intravascular pulmonary fluid.
Methods
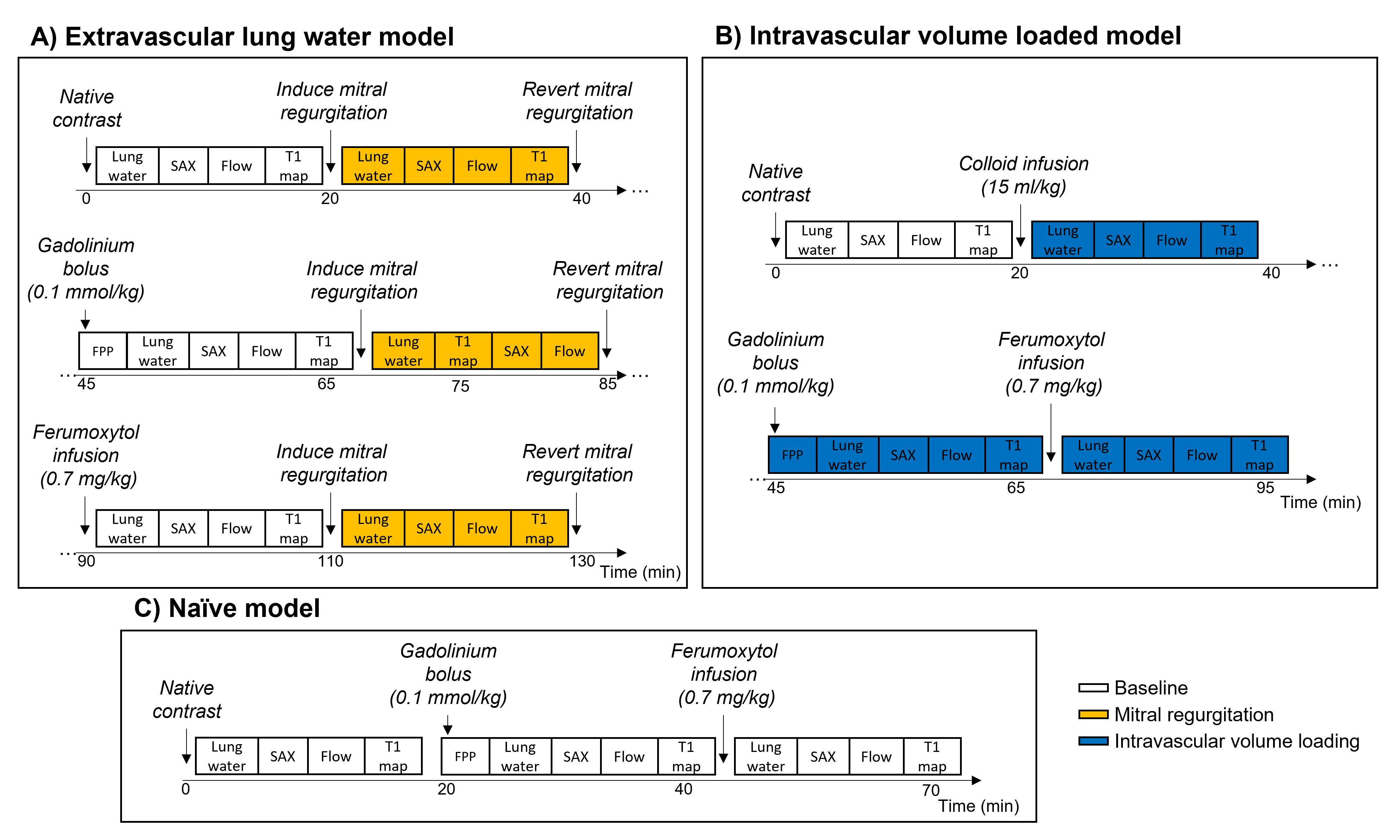
We performed a total of 13 pig experiments; extravascular lung water was induced in 5 animals using a reversible model of mitral regurgitation created by applying tension on a suture across the anterior mitral leaflet6,9 (49±4 kg), intravascular volume was increased in 3 animals through infusion of a colloid fluid with osmotic propensity to remain in the intravascular space (6% hydroxyethyl starch)10 (43±1 kg), and 5 were naïve controls (41±3 kg).Figure 1 illustrates the experimental protocols, where we sequentially acquired T1-maps (SASHA, bSSFP, TE/TR/θ 1.18ms/556ms/31°, TI array 104x8–200x4–374x3 ms, 43 segments, 3.5x3.5x10 mm resolution, 3 axial slices)11, proton density weighted (PDw) ultrashort echo time (UTE)12, short-axis cine, and aortic flow images at 0.55T13 with native, gadolinium, and ferumoxytol contrast. First pass perfusion images were acquired during gadolinium injection, to calculate the pulmonary blood volume14. Pulmonary arterial wedge pressures (PAWP) were measured to corroborate increases in extravascular and intravascular pulmonary fluid.
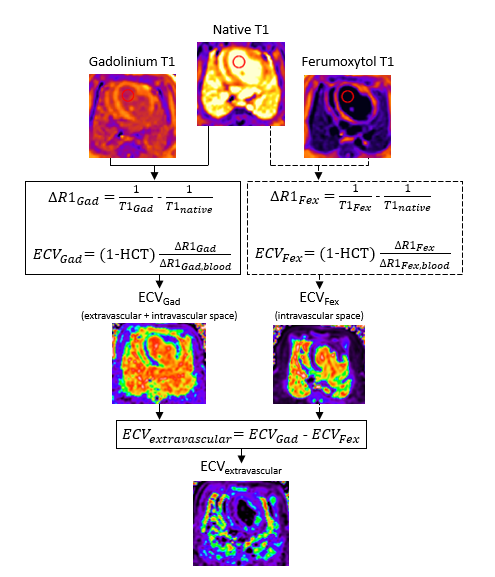
We calculated mean lung ECV across all slices as shown in Figure 215, and defined extravascular ECV as the difference in gadolinium ECV (intravascular + extravascular compartments) and ferumoxytol ECV (intravascular compartment), i.e., ECVextravascular=ECVgadolinium-ECVferumoxytol. Extravascular lung water volumes were calculated as the lung water volume by PDw imaging multiplied with ECVextravascular. Stroke volume, cardiac output, and mitral regurgitant fraction were derived from cine and flow images.
Results
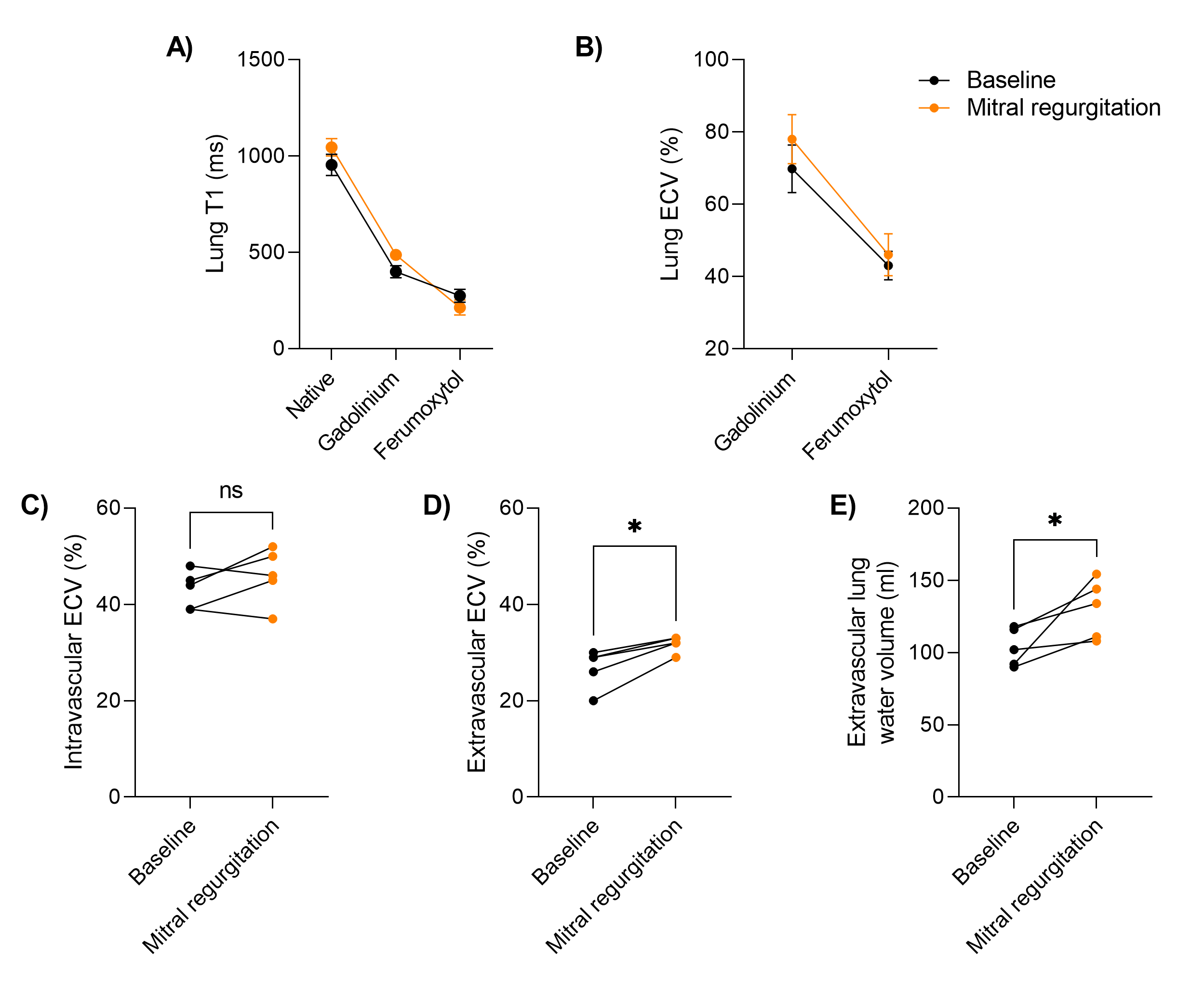
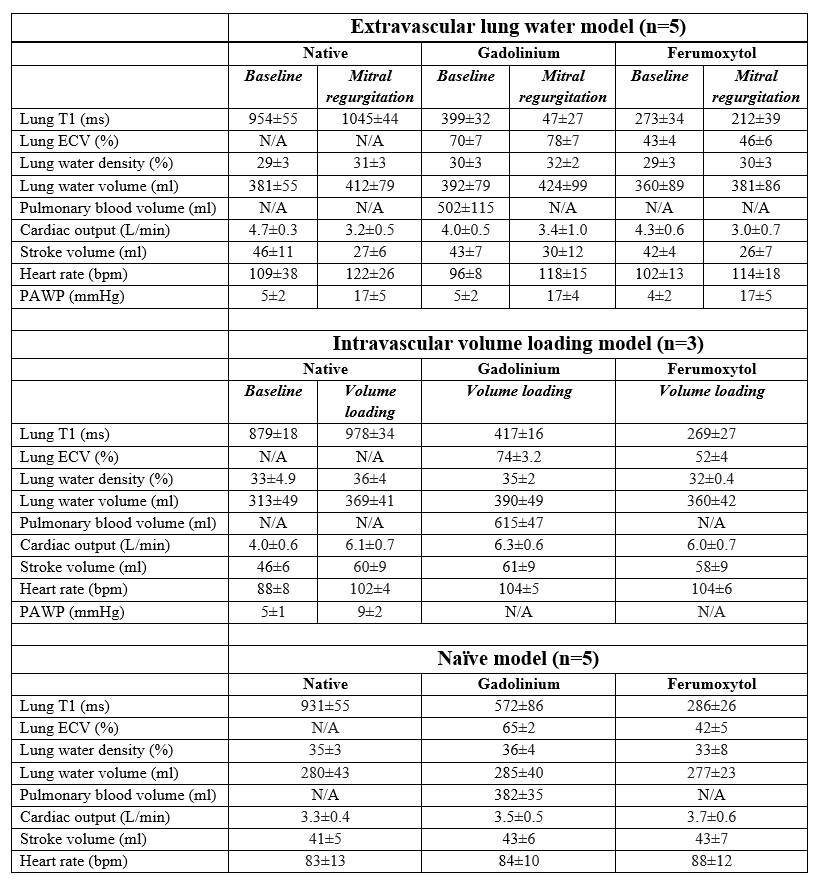
Table 1 summarizes T1 values, ECV, extravascular lung water volume, and cardiac parameters for each porcine model.Extravascular lung water model. We measured differences in baseline vs mitral regurgitation ECVextravascular of 27±4.1 vs 32±1.6% (p=0.005), respectively, and an extravascular lung water volume of 104±13ml vs 130±20ml (p=0.05) (Figure 3). The mitral regurgitation intervention was reproducible, verified through similarly achieved mitral regurgitant fractions (native 49±17%, gadolinium 48±19%, ferumoxytol 48±21%, p>0.05) and a consistent increase in PAWP (native 244±80%, gadolinium 241±76%, ferumoxytol 318±144%, p>0.05) for each contrast (Table 1). The similar ferumoxytol ECV at baseline and mitral regurgitation (43±4 vs 46±6%, p=0.23) was expected, given that it reflects the unchanged intravascular ECV component.
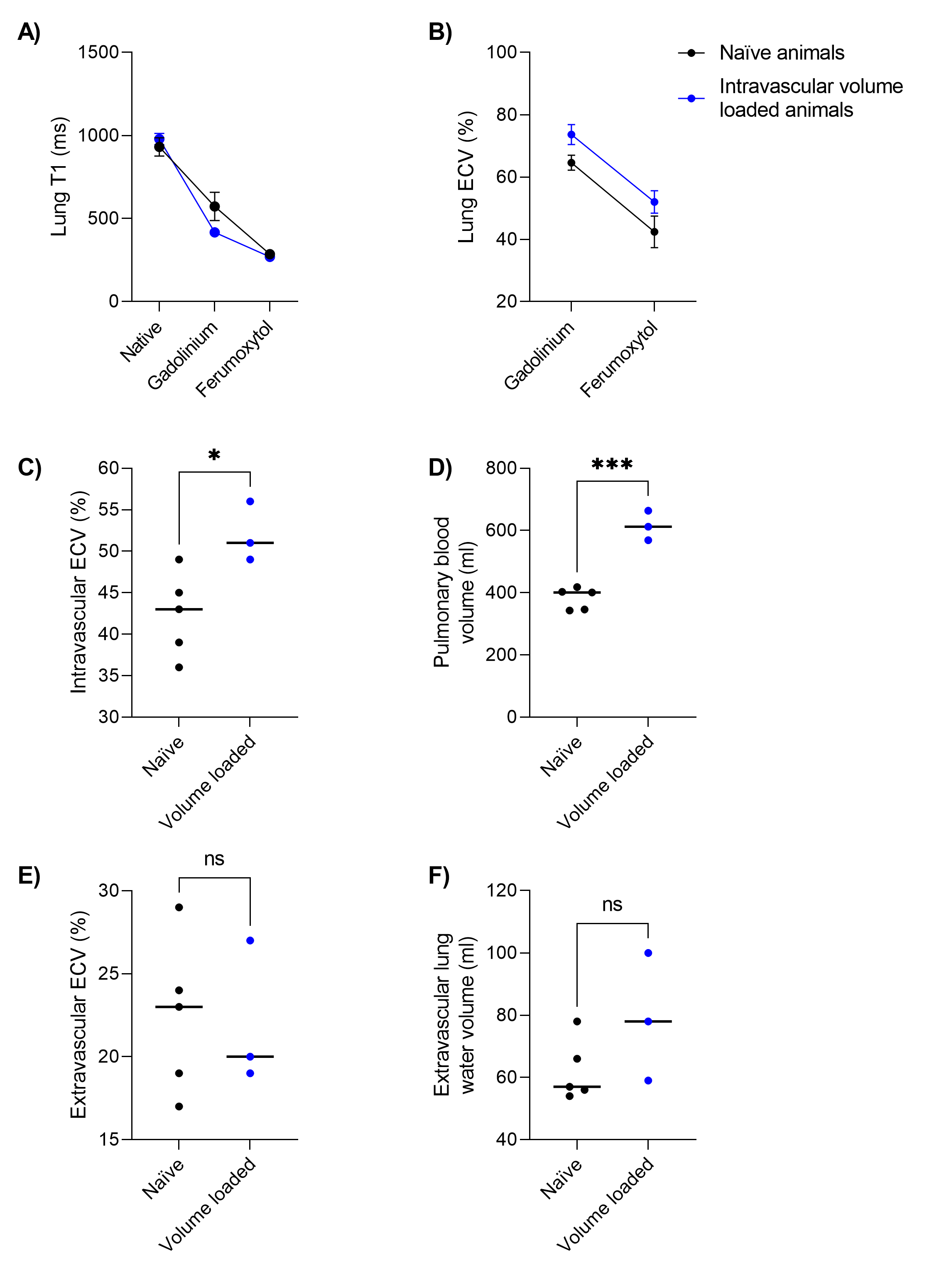
Intravascular volume loaded vs naïve model. Compared to naïve pigs, we measured a higher intravascular ECVferumoxytol in the volume loaded model (42±5.1% vs 52±3.6%, p=0.03), but no differences in ECVextravascular (22±4.7% vs 22±4.4%, p=0.91) (Figure 4). The intravascular volume loading through colloid infusion was corroborated by pulmonary blood volume measurements (382±35ml in naïve vs 615±47ml in the volume loaded model, p=0.0002).
As a control, we measured the left ventricular blood pool ECVextravascular, which was ~0% for each animal model (extravascular model -0.8±0.46%, intravascular volume loaded model -0.53±0.26%, naïve -0.62±0.80%), indicating that enough time was allowed for gadolinium contrast decay before acquiring ferumoxytol T1-maps.
Discussion
In this study we expand the established cardiac MRI method of quantifying myocardial ECV using gadolinium to the lungs15,16, where we demonstrate a novel method to derive both intravascular and extravascular ECV through a dual contrast approach in three different porcine models. It is important to note that the air volume is not reflected in the lung ECV, as MRI does not measure volume contributions from air. Gadolinium-based lung ECV should therefore not be interpreted as if the lungs are composed of ~70% fluid, but rather that 70% of the non-air volume is extracellular. Future work may explore dual contrast ECV in humans at rest and exercise stress, which may provide pathophysiological insight in exercise-induced dyspnea in heart failure.Conclusion
Dual contrast extravascular lung ECV measurements corresponded well with predicted increases in extravascular and intravascular pulmonary fluid interventions, and may, along with lung water MRI, comprise a promising method for extravascular lung water quantification.Acknowledgements
This work was funded by NHLBI DIR (Z01-HL006257, Z01-HL006213, Z01-HL006039). The authors would like to acknowledge the assistance of Siemens Healthcare in the modification of the MRI system for operation at 0.55T, and the stack-of-spirals UTE sequence, under an existing cooperative research agreement (CRADA) between NHLBI and Siemens Healthcare. We would also like to acknowledge the contributions of Victoria Frasier and Katherine Lucas.References
1. Thompson RB, Chow K, Pagano JJ, Sekowski V, Michelakis ED, Tymchak W, et al. Quantification of lung water in heart failure using cardiovascular magnetic resonance imaging. J Cardiovasc Magn Reson 2019;21:58. doi:10.1186/s12968-019-0567-y.
2. Meadus WQ, Stobbe RW, Grenier JG, Beaulieu C, Thompson RB. Quantification of lung water density with UTE Yarnball MRI. Magn Reson Med 2021;86:1330–1344. doi:10.1002/mrm.28800.
3. Seemann F, Javed A, Chae R, Ramasawmy R, O’Brien K, Baute S, et al. Imaging gravity-induced lung water redistribution with automated inline processing at 0.55 T cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2022;24:35. doi:10.1186/s12968-022-00862-4.
4. Rocha BML, Cunha GJL, Freitas P, Lopes PMD, Santos AC, Guerreiro S, et al. Measuring lung water adds prognostic value in heart failure patients undergoing cardiac magnetic resonance. Sci Rep 2021;11:20162. doi:10.1038/s41598-021-99816-6.
5. Burrage MK, Hundertmark M, Valkovič L, Watson WD, Rayner J, Sabharwal N, et al. Energetic Basis for Exercise-Induced Pulmonary Congestion in Heart Failure With Preserved Ejection Fraction. Circulation 2021;144:1664–1678. doi:10.1161/CIRCULATIONAHA.121.054858.
6. Seemann F, Javed A, Khan J, Bruce C, Chae R, Yildirim K, et al. Dynamic lung water magnetic resonance imaging during exercise stress. Magn Reason Med 2023:1–18. doi:10.1002/mrm.29716.
7. Schelbert EB, Testa SM, Meier CG, Ceyrolles WJ, Levenson JE, Blair AJ, et al. Myocardial extravascular extracellular volume fraction measurement by gadolinium cardiovascular magnetic resonance in humans: slow infusion versus bolus. J Cardiovasc Magn Reson 2011;13:16. doi:10.1186/1532-429X-13-16.
8. Landry R, Jacobs PM, Davis R, Shenouda M, Bolton WK. Pharmacokinetic Study of Ferumoxytol: A New Iron Replacement Therapy in Normal Subjects and Hemodialysis Patients. Am J Nephrol 2005;25:400–410. doi:10.1159/000087212.
9. Babaliaros VC, Greenbaum AB, Khan JM, Rogers T, Wang DD, Eng MH, et al. Intentional Percutaneous Laceration of the Anterior Mitral Leaflet to Prevent Outflow Obstruction During Transcatheter Mitral Valve Replacement: First-in-Human Experience. JACC Cardiovasc Interv 2017;10:798–809. doi:10.1016/j.jcin.2017.01.035.
10. Wieslander B, Seemann F, Javed A, Bruce CG, Ramasawmy R, Jaimes A, et al. Impact of Vasodilation on Oxygen-Enhanced Functional Lung MRI at 0.55 T. Invest Radiol 2023;58:663–672. doi:10.1097/RLI.0000000000000958.
11. Chow K, Flewitt JA, Green JD, Pagano JJ, Friedrich MG, Thompson RB. Saturation recovery single-shot acquisition (SASHA) for myocardial T 1 mapping. Magn Reson Med 2014;71:2082–2095. doi:10.1002/mrm.24878.
12. Javed A, Ramasawmy R, O’Brien K, Mancini C, Su P, Majeed W, et al. Self-gated 3D stack-of-spirals UTE pulmonary imaging at 0.55T. Magn Reson Med 2022;87:1784–1798. doi:10.1002/mrm.29079.
13. Campbell-Washburn AE, Ramasawmy R, Restivo MC, Bhattacharya I, Basar B, Herzka DA, et al. Opportunities in interventional and diagnostic imaging by using high-performance low-field-strength MRI. Radiology 2019;293:384–393. doi:10.1148/radiol.2019190452.
14. Seraphim A, Knott KD, Menacho K, Augusto JB, Davies R, Pierce I, et al. Prognostic Value of Pulmonary Transit Time and Pulmonary Blood Volume Estimation Using Myocardial Perfusion CMR. JACC Cardiovasc Imaging 2021;14:2107–2119. doi:10.1016/j.jcmg.2021.03.029.
15. Kellman P, Wilson JR, Xue H, Ugander M, Arai AE. Extracellular volume fraction mapping in the myocardium, part 1: evaluation of an automated method. J Cardiovasc Magn Reson 2012;14:63. doi:10.1186/1532-429X-14-63.
16. Kellman P, Wilson JR, Xue H, Bandettini WP, Shanbhag SM, Druey KM, et al. Extracellular volume fraction mapping in the myocardium, part 2: initial clinical experience. J Cardiovasc Magn Reson 2012;14:64. doi:10.1186/1532-429X-14-64.
Figures