1285
Acute versus chronic ventral lateral thalamus intrinsic connectivity after MR-guided focused ultrasound thalamotomy for essential tremor1Departments of Radiology and Clinical Neurosciences, University of Calgary, Calgary, AB, Canada, 2Department of Surgery, University of Alberta, Edmonton, AB, Canada, 3Department of Clinical Neurosciences, University of Calgary, Calgary, AB, Canada, 4Departments of Community Health Sciences and Clinical Neurosciences, University of Calgary, Calgary, AB, Canada
Synopsis
Keywords: Functional Connectivity, Focused Ultrasound, Essential Tremor, fMRI, Longitudinal
Motivation: To address the gap in understanding the longitudinal impact of MR-guided focused ultrasound (MRgFUS)-thalamotomy on motor network connectivity in essential tremor (ET).
Goal(s): To elucidate the changes in functional connectivity within the motor network following MRgFUS thalamotomy, distinguishing between acute and chronic phases.
Approach: Connectivity changes in the ventrolateral (VL) thalamus of 19 ET patients were tracked using fMRI at three intervals—pre-operation, one day, and three months post-MRgFUS.
Results: Initially, both VLs showed diminished connectivity with sensorimotor regions. By three months, left VL had enhanced connections with associative and visual areas, while right VL demonstrated sustained reduced sensorimotor connectivity, reflecting hemisphere-specific functional reorganization.
Impact: Mapping evolving connectivity of ventrolateral thalamus after MR-guided focused ultrasound (MRgFUS) thalamotomy enables tailored essential tremor treatments, potentially yielding better outcomes and informing treatment parameters, while also providing putative biomarkers for treatment efficacy and broader insights into neurological network management.
Introduction
Essential tremor (ET) is characterized by involuntary, rhythmic oscillations1. While medication is the preferred initial treatment, individuals with medication-resistant severe tremors may opt for surgical interventions. Among these, magnetic resonance-guided focused ultrasound (MRgFUS) thalamotomy of the ventrolateral (VL) thalamus offers a less invasive alternative that ameliorates tremor2,3. However, the longitudinal effects of MRgFUS thalamotomy on functional connectivity within the motor network remain poorly understood. Current research4–6 has predominantly concentrated on postoperative changes at singular time points, without comprehensive analysis distinguishing between the immediate and prolonged alterations in network connectivity.Methods
Participants19 ET patients (age range 53-97; 13M/6F) who underwent MRgFUS lesioning of the left ventrolateral (VL) thalamus were included in this study. Patients were chosen from a larger pool based upon MRI quality and completeness of follow-up data.
Clinical Measures
Tremor severity was assessed using the Clinical Rating Scale for Tremor (CRST)7 at baseline (PRE) and 3-months following thalamotomy (3M). Higher scores indicate more severe tremor.
MRI
All data were collected with a 3T Discovery 750 (GE Healthcare) and a 32-channel (Nova Medical) or 12-channel (GE Healthcare) head coil. T1-weighted anatomical images (3D FSPGR (BRAVO), TR/TE/TI: 8.156/3.172/650ms, flip angle=10°, 256x256matrix, 256mm FOV, 188 slices., 1mm3 voxel) and BOLD contrast T2*-weighted gradient-echo echo planar imaging (EPI) functional images (TR = 3000 ms, TE = 28 ms, flip angle = 90°, voxel size = 1.75x1.75x3 mm3, matrix size = 128x128) were analyzed for this study. MR data were collected prior to surgery (Pre), one day following surgery (Day1) and three months following surgery (3M).
Functional MRI Preprocessing
Standard preprocessing of functional images used FMRIB's FSL8 and included motion correction, slice timing correction, spatial smoothing (4mm), high-pass temporal filtering and registration to structural, functional and standard space. Additional physiological, scanner and movement-related noise was removed using FMRIB's ICA-based Xnoiseifier (FIX, FSL).
ROI Selection and Individual Seed-based Map Generation
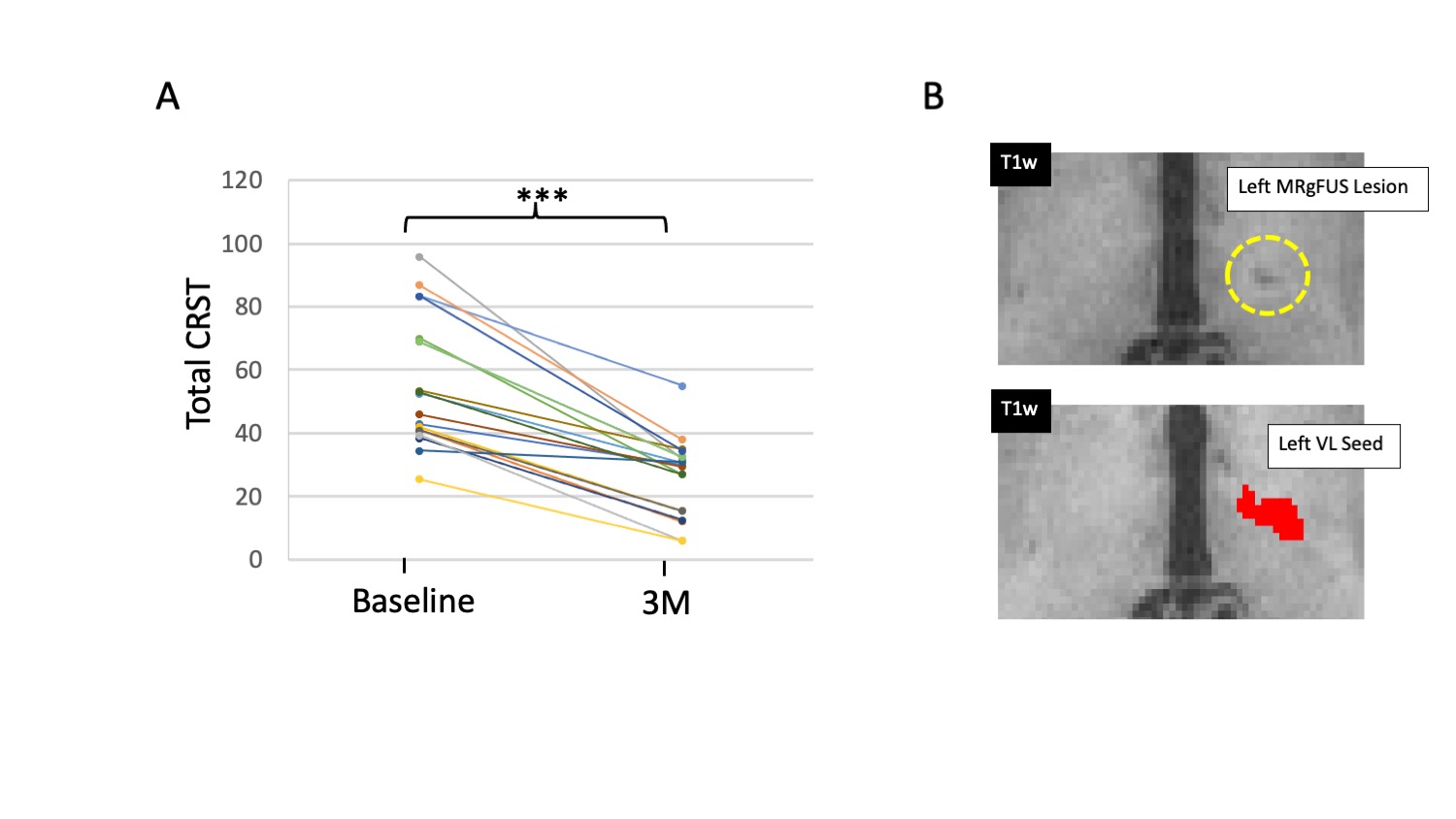
The VL thalamus was defined in standard space based on the Morel digital atlas9 (Figure 1), then transformed into native functional space using affine registration and nearest neighbour interpolation (FSL-FLIRT). Cerebral spinal fluid (CSF) and whole-brain masks were also created. Individual seed-based functional maps were generated using the BOLD time course of the left and right VL seed as a regressor of interest and CSF and global signal time courses as nuisance regressors.
Group-level Statistical Analysis
Higher level analyses were accomplished using the General Linear Model in FEAT (FSL). Subject-level seed-based maps were analyzed using a within subjects, repeated-measures design for each comparison: Pre<Day1, Pre<3M, Day1<3M. Resulting statistical maps were thresholded (a priori) at the voxel level (p<0.01), and FDR cluster-level corrected at p<0.05 (Bonferroni corrected to p<0.0125 to account for 4 seed ROIs).
Results
Clinical MeasuresRelated-Samples Wilcoxon Signed Rank Test revealed tremor (CRST score) was significantly reduced across patients from PRE to 3M (p<0.001, Figure 1).
Intrinsic Connectivity Analysis
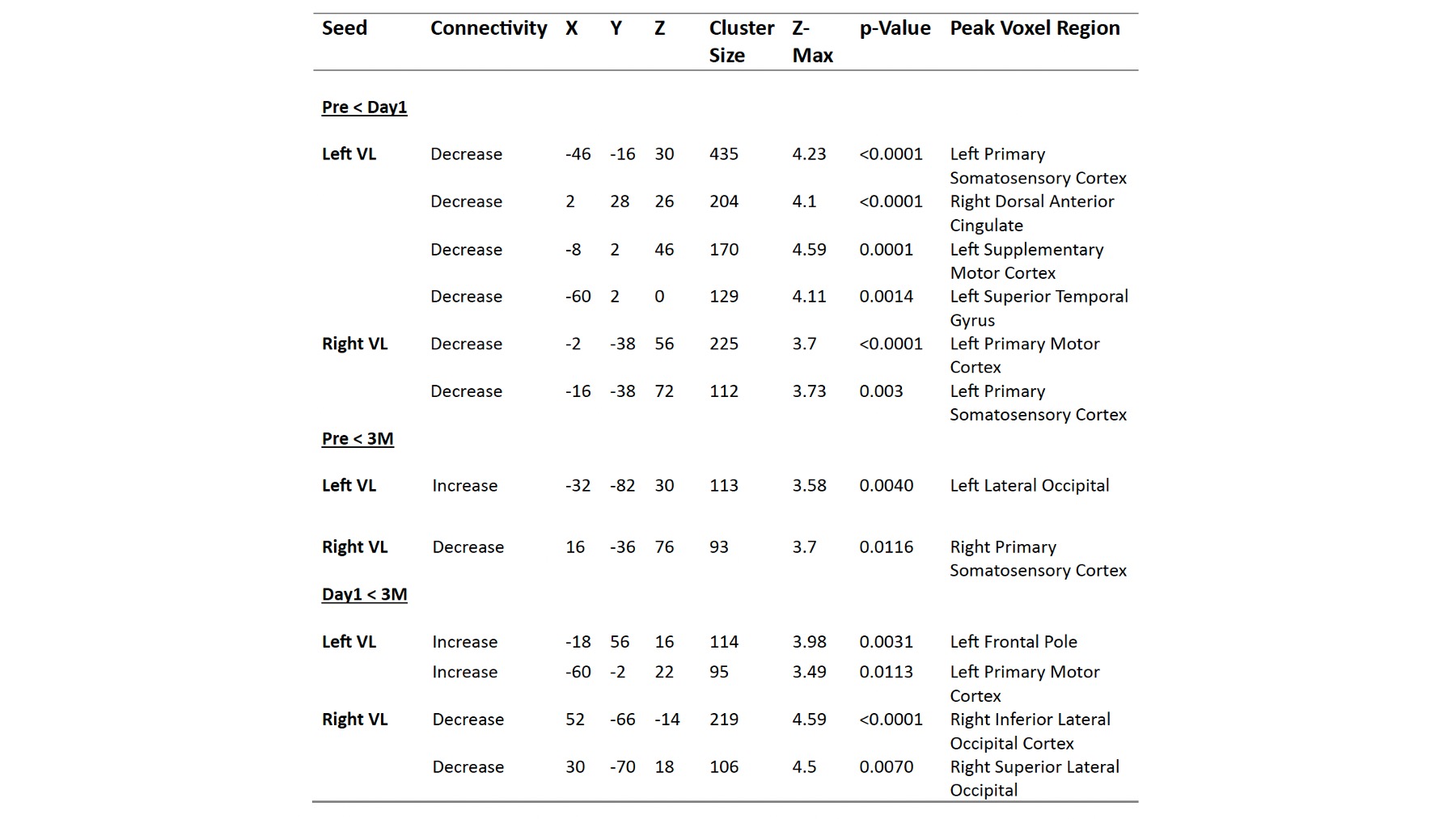
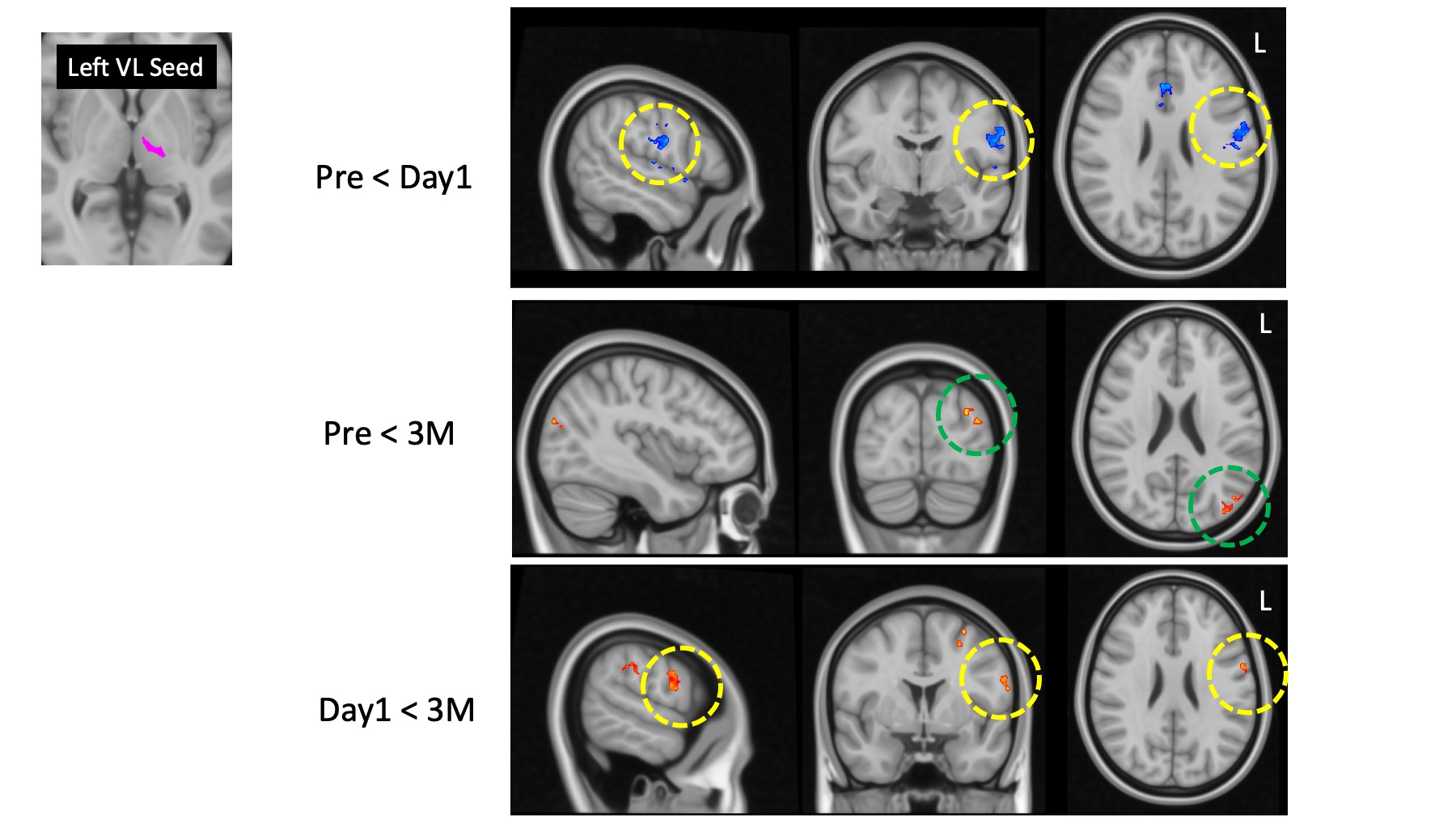
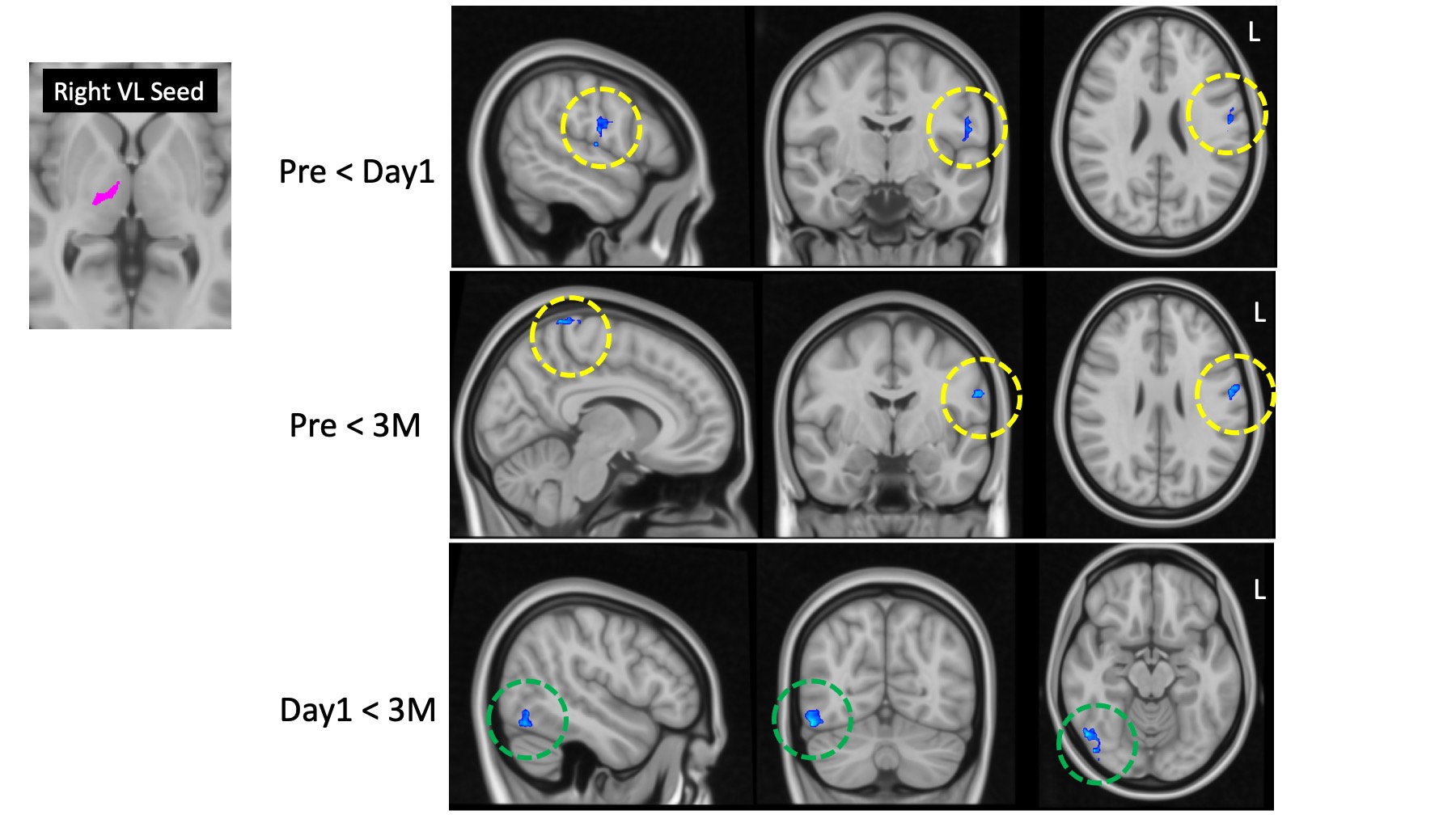
Pre<Day1: Both left and right VL demonstrated reduced connectivity with left motor and somatosensory regions on Day1 following left MRgFUS thalamotomy. (Table 1, Figure 2,3)
Pre<3M: The left VL demonstrated increased connectivity to the left lateral occipital cortex, whereas the right VL showed decreased connectivity with the right primary somatosensory cortex, 3 months following MRgFUS thalamotomy. (Table 1, Figure 2,3)
Day1<3M: Connectivity increased between left VL and left primary motor cortex, as well as with the left frontal pole, from Day1 following surgery to 3M. Conversely, connectivity decreased between right VL and regions of the right occipital cortex. (Table 1, Figure 2,3)
Discussion
Our findings reveal a pronounced temporal evolution in connectivity patterns of the VL thalamus subsequent to MRgFUS thalamotomy. Initially, there is a marked decrease in connectivity of the left VL within primary sensorimotor areas on the side of the lesion (left), but these alterations dissipate within three months post-operation. Long-term changes within the lesioned hemisphere, remain only between the left ventrolateral (VL) thalamus and occipital regions. We also note a reinstatement of some connectivity between the left VL and the left primary motor cortex, progressing from the immediate postoperative stage to the chronic phase, supporting transient interruption. In contrast, the contralesional VL (right) maintains decreased connectivity with the sensorimotor cortex on the lesion side, at three months.Conclusions
The transition of left VL thalamus connectivity from reduced local sensorimotor to enhanced associative and visual from Day 1 to 3 months post-surgery, together with increased cross-hemisphere sensorimotor connectivity of the contralesional VL, indicates significant functional reorganization in response to the thalamic intervention over time.Acknowledgements
No acknowledgement found.References
1. Gövert, F., Becktepe, J. S. & Deuschl, G. Current concepts of essential tremor. Rev Neurol (Paris) 172, 416–422 (2016).
2. Elias, W. J. et al. A pilot study of focused ultrasound thalamotomy for essential tremor. N Engl J Med 369, 640–648 (2013).
3. Wintermark, M. et al. Imaging findings in MR imaging-guided focused ultrasound treatment for patients with essential tremor. AJNR Am J Neuroradiol 35, 891–896 (2014).
4. Kato, S. et al. Magnetic resonance-guided focused ultrasound thalamotomy restored distinctive resting-state networks in patients with essential tremor. J Neurosurg 138, 306–317 (2023).
5. Tuleasca, C. et al. Normalization of aberrant pretherapeutic dynamic functional connectivity of extrastriate visual system in patients who underwent thalamotomy with stereotactic radiosurgery for essential tremor: a resting-state functional MRI study. J Neurosurg 132, 1792–1801 (2019).
6. Lu, H. et al. Assessing the impact of MR-guided focused ultrasound thalamotomy on brain activity and connectivity in patients with essential tremor. Neurosurg Focus 53, E5 (2022).
8. Fahn S, Tolosa E, Marin C. Clinical rating Scale for Tremor. In: Jankovik J and Tolosa E. Parkinson’s Disease and Movement Disorders. Baltimore-Munich:Urban & Scharzenberg, p. 225-234 (1988).
8. Smith, S. M. et al. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage 23 Suppl 1, S208-219 (2004).
9. Niemann, K., Mennicken, V. R., Jeanmonod, D. & Morel, A. The Morel stereotactic atlas of the human thalamus: atlas-to-MR registration of internally consistent canonical model. Neuroimage 12, 601–616 (2000).
Figures