1283
First Evidence of sustained reduction of Essential Tremor with MR-Guided Low-Energy Ultrasound Neuromodulation1MOVIT team, Sorbonne Université, Inserm U1127, CNRS 7225, Hôpital Pitié-Salpêtriere, ICM, Paris, France, 2Neuroradiology, APHP, Sorbonne universite, Paris, France, 3Inserm U1273, ESPCI Paris, CNRS UMR8361, PSL University, Physics for Medicine Paris, Paris, France, 4Centre de NeuroImagerie de Recherche – CENIR, Sorbonne Université, Inserm U1127, CNRS 7225, Hôpital Pitié-Salpêtriere, ICM, Paris, France, 5Insightec, Tirat Carmel, Israel, 6Sorbonne Université, Inserm U1127, CNRS 7225, Hôpital Pitié-Salpêtriere, ICM, Paris, France
Synopsis
Keywords: MR-Guided Focused Ultrasound, Focused Ultrasound, MRgFUS, neuromodulation, essential tremor, thermometry
Motivation: Transcranial Ultrasound Stimulation (TUS) is a non-invasive technology for brain stimulation, particularly suited for the neuromodulation of deep brain structures.
Goal(s): We investigated the behavioral effects of low-energy TUS in the thalamus in Essential Tremor patients scheduled for MR-guided ultrasound treatment.
Approach: Two targets were tested: the ventral intermediate nucleus of the thalamus (VIM) and the dentato-rubro-thalamic tract (DRT). MRI was used for procedure guidance and monitoring. The effect was recorded using MR-compatible accelerometers.
Results: VIM low-energy neuromodulation induced transient change in tremor power (p-value< 0.001). DRT neuromodulation reduced tremor power (p-value<0.001) with a sustained post-effect, without MR-thermometry exhibiting any significant thermal rise.
Impact: High precision focusing enhanced by state of the art transcranial aberration correction allowed unprecedent transient tremor reduction in Essential Tremor patients following low-energy thalamic ultrasound stimulation under MRI guidance.
INTRODUCTION
Brain stimulation is crucial in the treatment of neurological and psychiatric disorders. The two primary modalities are deep-brain stimulation (DBS) and transcranial magnetic stimulation (TMS)1. DBS, while invasive, effectively manages conditions such as essential tremor (ET). On the other hand, TMS, a non-invasive approach has limited spatial resolution and depth penetration.A promising non-invasive alternative is transcranial ultrasonic stimulation (TUS)2, offering millimetric precision. Previous studies have demonstrated its potential to modulate neural activity3-4, but mainly mild effects were reported. Most of these studies used single-element transducers with high f-numbers and lacked aberration correction to compensate for skull-related effects.
The Exablate Neuro 4000 clinical system (Insightec, Israel) uses aberration-corrected focused ultrasound (FUS) technology for non-invasive brain treatment under MRI guidance5. However its potential for neuromodulation has not been explored yet. In this study we have used the Exablate Neuro's high precision ultrasound targeting to investigate the behavioral effects of low-energy TUS in the thalamus of ET patients scheduled for MR-guided FUS (MRgFUS) treatment.
MATERIALS AND METHODS
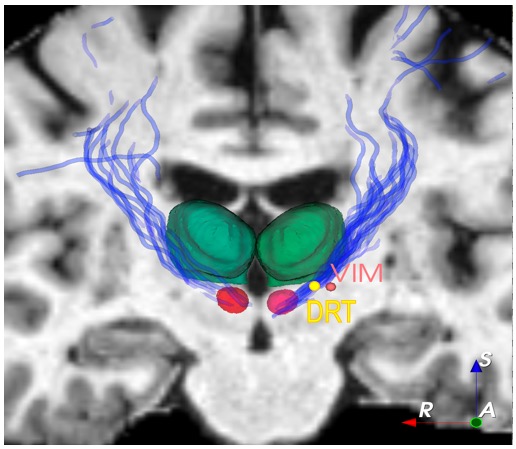
Population: This study included four ET patients unresponsive to medical treatments and scheduled for FUS thalamotomy. Baseline tremor assessments were conducted using the Clinical Scale for Rating Tremor (CSRT)6 and MRI-compatible accelerometers.Anatomical Targeting: For precise targeting, anatomical T1-weighted MP2RAGE sequences and diffusion tensor imaging fiber tracking (DTI-FT) were obtained during the inclusion visit using a Siemens Prisma 3T scanner with a 64-channel head coil. Two targets were selected: the ventral intermediate nucleus of the thalamus (VIM) and the dentato-rubro-thalamic tract (DRT). The VIM location was determined using the Guiot diagram and the deformable anatomical YeB atlas7, while DRT8 was located using tractography and local anatomical atlas, while DRT was located using tractography.
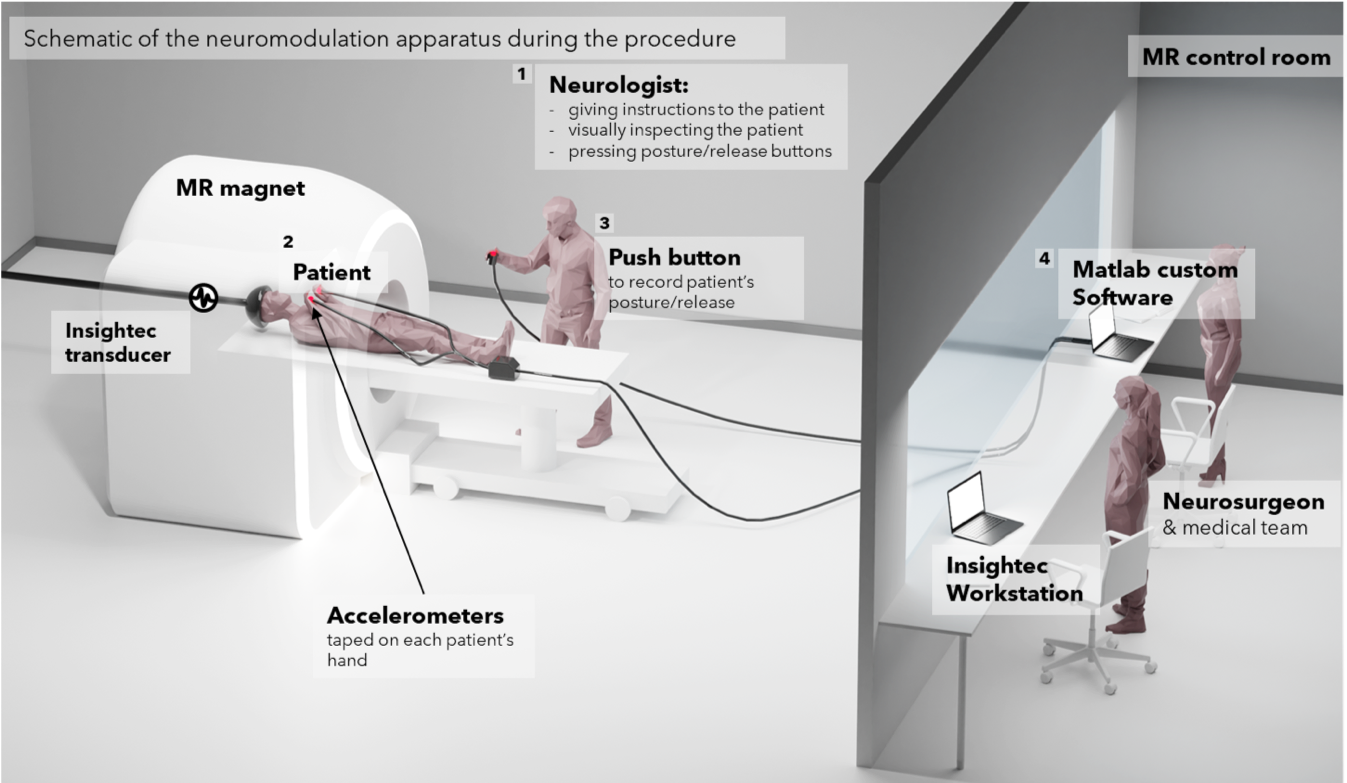
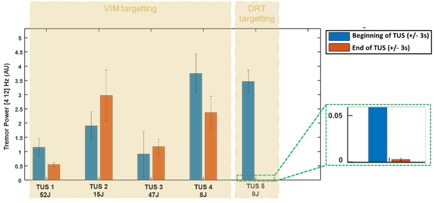
Neuromodulation Protocol: All sonications were performed using the Exablate Neuro 4000 device (Insightec Ltd, Israel), which features a transducer with 1024 distributed elements operating at a 650kHz transmit frequency. Following standard alignment procedures to confirm the target with thermal MRI, patients underwent non-thermal low-power sonications, targeting either the VIM or the DRT with four different sonication patterns. Patients maintained postures inside the MRI bore during transcranial ultrasound stimulation (TUS), and their posture-related tremor was monitored using two MR-compatible accelerometers on each hand (Fig 1). TUS efficacy was assessed by the change in average tremor power between two 6-second windows at the start and end of the TUS stimulation. TUS stimulations consisted of 3 bursts of 5 seconds each, followed by a 10-second pause, with varying duty cycles. Initially, four stimulations were performed in the VIM with total acoustic energies of [52; 15; 47; 8] J, respectively, and one in the DRT with 8 J.
Temperature Monitoring During Stimulation: Temperature within the patients' brains was continuously monitored using MR thermometry sequences during the sonication9.
RESULTS
The VIM and DRT targets were identified (Fig 2) and an alignment procedure under MRI was performed using their stereotaxic coordinates. Following the TUS sonications, the average tremor power decreased by 83.3% to 99.5% immediately or within the first 3 minutes. DRT and VIM exhibited differential effects. VIM neuromodulation induced a statistically significant but transient change in tremor power (p-value < 0.001). DRT neuromodulation significantly reduced tremor power (p-value < 0.001) (Fig 3). No post-effect occurred after VIM neuromodulation. Short-term post-effects were observed after DRT neuromodulation in all patients whose tremor was measured during this timeframe, with a reduction up to 99.5%. The tremor reduction over 80% persisted for more than 23 minutes after the ultrasound stimulation for 3 patients. No heating was observed in the MR thermometry images for any of the neuromodulation sonications.DISCUSSION
This study demonstrates significant motor responses in humans with low-energy transcranial ultrasound neuromodulation. In ET patients, DRT neuromodulation led to significant tremor reduction that persisted for up to 30 minutes. The neuromodulation effect varied between VIM and DRT, indicating target-specific responses. MR thermometry during neurostimulations did not show a significant thermal rise, supporting a non-thermal mechanism with a probable mechanical effect, in line with the acoustic energies at stake during neuromodulation ranging between 8 J and 52 J. Comparatively, during the high-intensity FUS treatment o the peak temperature in the thalamus was 58.7±2.4°C for averaged acoustic energies of 22300±7700J.While we have explored both targets in neuromodulation, for therapy, we have focused on the VIM as it's the classic lesion site in MRgFUS treatment for ET today. Still in the light of these results DTR target should be considered.CONCLUSION
The tremor reduction observed here after transcranial ultrasound stimulation of the thalamus with low energy is promising for the neuromodulation of deep brain targets under MRI using transcranial ultrasound.Acknowledgements
This work was supported by the Bettencourt Schueller Foundation, the "Agence Nationale de la Recherche" ANR-10-EQPX-15, the FUS Foundation and by APHP-DRCI.References
1. J.-P. Lefaucheur et al., Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS) , Clin. Neurophysiol., vol. 125, no 11, p. 2150‑2206, nov. 2014
2.J. Blackmore, S. Shrivastava, J. Sallet, C. R. Butler, et R. O. Cleveland, Ultrasound Neuromodulation: A Review of Results, Mechanisms and Safety , Ultrasound Med. Biol., vol. 45, no 7, p. 1509‑1536, juill. 2019
3. W. Legon et al., Transcranial focused ultrasound modulates the activity of primary somatosensory cortex in humans , Nat. Neurosci., vol. 17, no 2, p. 322‑329, févr. 2014
4. W. Lee et al., Transcranial focused ultrasound stimulation of human primary visual cortex , Sci. Rep., vol. 6, no 1, p. 34026, sept. 2016
5. W. J. Elias et al., A Randomized Trial of Focused Ultrasound Thalamotomy for Essential Tremor , N. Engl. J. Med., vol. 375, no 8, p. 730‑739, août 2016
6. S. Fahn, E. Tolosa, et C. Marin, Clinical Rating Scale for Tremor », in Parkinson’s Disease and Movement Disorders, 1988
7. Bardinet E, Bhattacharjee M, Dormont D. A three-dimensional histological atlas of the human basal ganglia. II. Atlas deformation strategy and evaluation in deep brain stimulation for Parkinson disease., Neurosurg. 2009 Feb;110(2):208-1
8. H. G. Kwon, J. H. Hong, C. P. Hong, D. H. Lee, S. H. Ahn, et S. H. Jang, «Dentatorubrothalamic tract in human brain: diffusion tensor tractography study , Neuroradiology, vol. 53, no 10, p. 787‑791, oct. 2011
9. V. Rieke et K. Butts Pauly, MR thermometry , J. Magn. Reson. Imaging, vol. 27, no 2, p. 376‑390, févr. 2008
Figures