1282
Patient-specific targeting of VIM using THOMAS segmentation predicts post-MRgFUS side effects: a retrospective evaluation1UCLA Brain Tumor Imaging Laboratory (BTIL), Center for Computer Vision and Imaging Biomarkers, University of California, Los Angeles, Los Angeles, CA, United States, 2Department of Radiological Sciences, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States, 3Department of Bioengineering, Henry Samueli School of Engineering and Applied Science, University of California, Los Angeles, Los Angeles, CA, United States, 4Department of Neurosurgery, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States, 5Department of Neurology, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States, 6Department of Psychiatry and Biobehavioral Sciences, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, United States
Synopsis
Keywords: MR-Guided Focused Ultrasound, MR-Guided Interventions
Motivation: Precise and personalized targeting for MR-guided focused ultrasound (MRgFUS) is desired to ensure treatment efficacy and avoid side effect.
Goal(s): To assess THalamus Optimized Multi Atlas Segmentation (THOMAS) on white-matter nulled MRI for targeting of the ventral intermediate (VIM) thalamic nucleus in MRgFUS for tremor patients.
Approach: We retrospectively assessed the relationships of standard indirectly targeted coordinates, post-FUS lesions, and THOMAS segmentation with post-FUS side effects and tremor scores in patients who underwent VIM-MRgFUS.
Results: In patients who exhibited side effects, FUS lesions had a smaller overlap with THOMAS-based VIM segmentation and were located more inferiorly.
Impact: THOMAS is a novel automated thalamic segmentation tool which may aide in the targeting of the VIM nucleus, potentially reducing side effects and improving treatment outcomes in MRgFUS for patients with tremor.
Introduction
Magnetic resonance-guided focused ultrasound (MRgFUS) ablation of the ventral intermediate (VIM) thalamic nucleus is an incisionless lesioning therapy for essential tremor (ET) and tremor-dominant Parkinson’s disease (PD). Indirect targeting of VIM using AC-PC line lacks patient specificity. Recently, an automated pipeline for thalamic nucleus segmentation, named THalamus Optimized Multi Atlas Segmentation (THOMAS), has been developed.1 We aim to assess the relationship between intra-procedural standard indirectly-targeted coordinates during the procedure, post-FUS lesions, and VIM segmented by THOMAS, and examine their correlations with post-operative side effects and tremor scores.Methods
Patients and image acquisitionWe retrospectively analyzed 30 patients (ET, n = 26; PD, n = 4) who underwent unilateral VIM-MRgFUS. MR images were acquired using 3T scanners. Pre-operative images included Fast Gray Matter Acquisition T1 Inversion Recovery (FGATIR)2, a white matter-nulled MPRAGE for better visualization of the deep gray matter (TE/TR/TI, 2.79–3.52/3000/409ms; FA, 8–9degrees; resolution, 0.8x0.8x1.0mm), 3D T1-MPRAGE, and 3D T2-SPACE or 2D axial T2-weighted TSE. For intra-operative imaging, 3D T1-FSPGR or 3D T2-FIESTA was acquired. Post-operative images including T1-weighted MPRAGE and T2-weighted SPACE were acquired the day after FUS.
Image post-processing
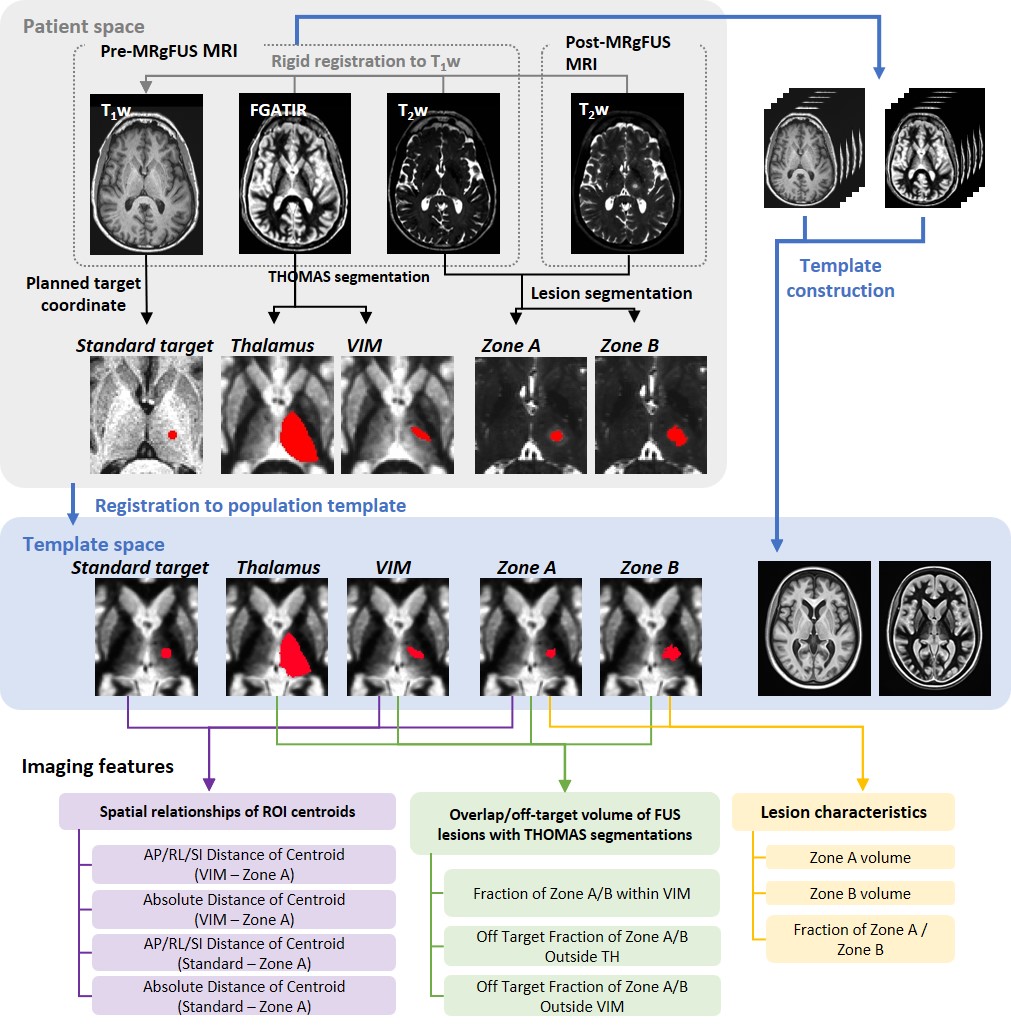
The following ROIs were created (Figure 1): a) Standard VIM targets from the coordinates of the first sonication of the procedure, which were indirectly targeted based on the AC-PC line, b) FUS-induced lesion Zone A, which corresponds to the strongly hyperintense cytotoxic edema and center hypointense area representing coagulation necrosis, and Zone B including Zone A and the slightly hyperintense vasogenic edema, which were delineated on post-operative T2-weighted images using a thresholding method, and c) the thalamus (TH) and VIM segmentation by applying THOMAS to the pre-operative FGATIR images. These ROIs were nonlinearly aligned to the population-specific template created from pre-operative T1-weighted and FGATIR images using the Advanced Normalization Tools (ANTs) algorithm. We computed imaging features in the template space including 1) FUS-treated lesion volumes, 2) overlap between FUS lesions and TH/VIM segmentations, 3) distance between FUS lesions and VIM segmentation and 4) distance between FUS lesions and the standard target.
Statistical analysis
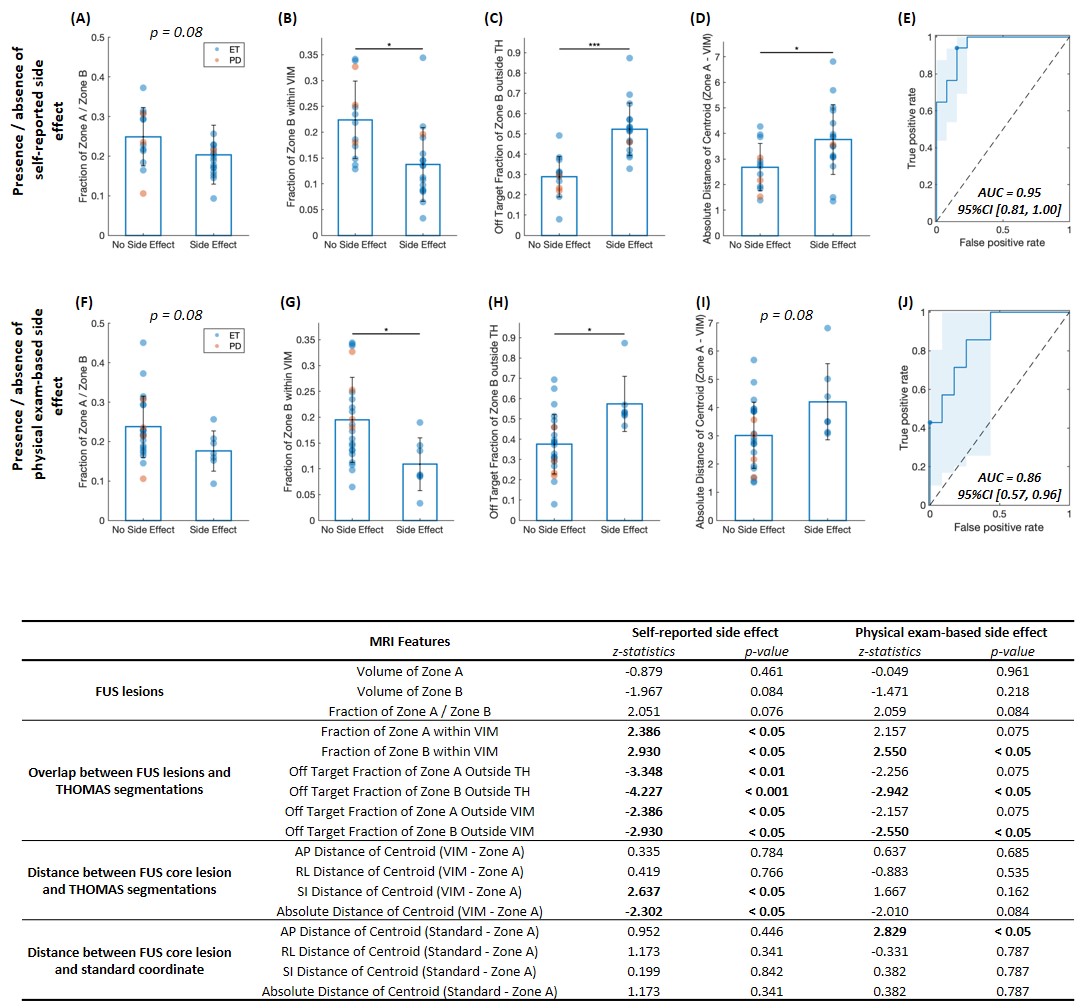
Imaging features were compared between patients with gait/balance side effects (self-reported and physical exam-based) and those without, using Wilcoxon rank-sum test. We also assessed correlations between imaging features and post-operative Fahn-Tolosa-Marin (FTM) scores of the sum of tremor severity and drawing test (maximum score 24) using Spearman’s rank correlation. Handwriting and pouring scores were not included for the analysis due to the insufficient records. Benjamini–Hochberg (BH) correction was performed for multiple comparison and correlation tests. In addition, we built multi-variate prediction models of side effects using imaging features that showed significant differences in cross-sectional comparisons. The two logistic models were evaluated using the ROC analyses and the AUCs were calculated. P<0.05 was considered statistically significant.
Results
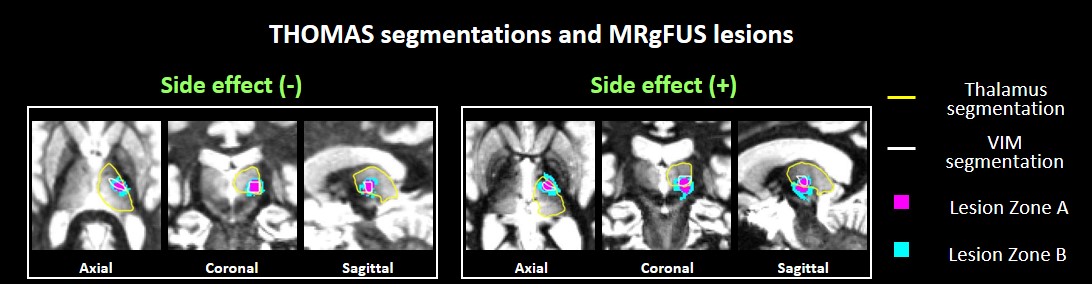
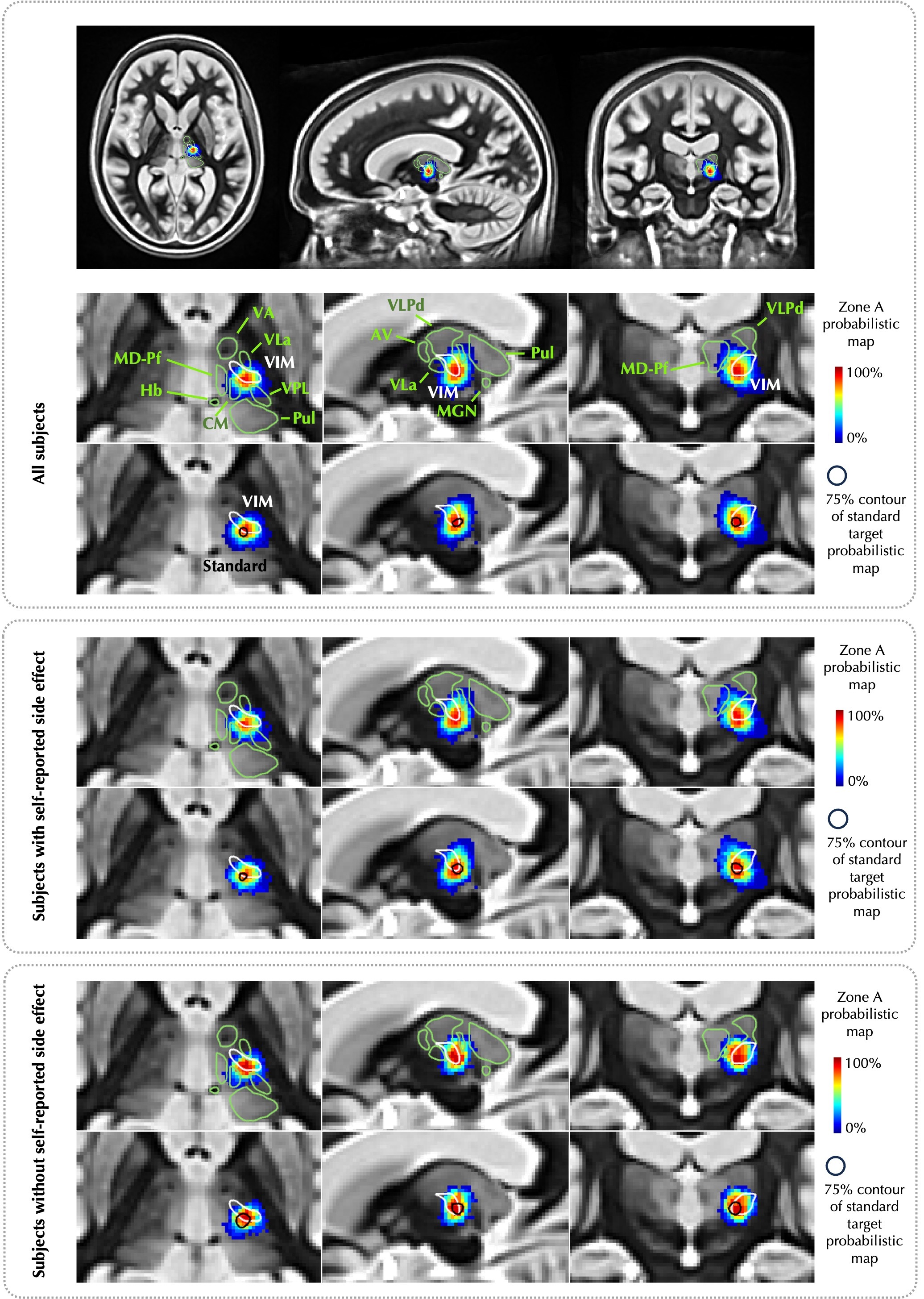
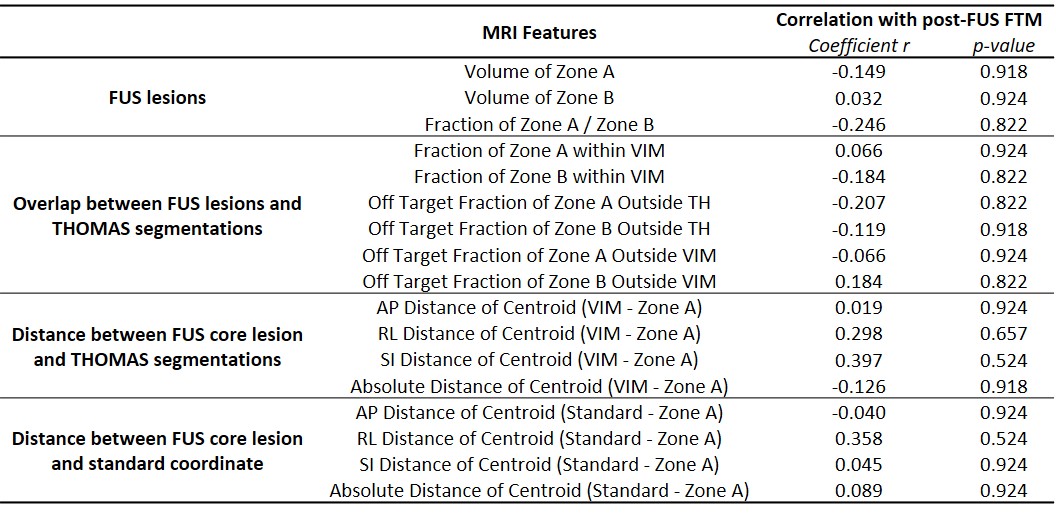
All patients demonstrated tremor improvement. Seventeen and five patients experienced self-reported and exam-based gait/balance disturbance, respectively. Figure 2 illustrates the THOMAS segmentations and FUS lesions in two example patients. Patients with self-reported side effects had a significantly smaller fraction of Zone A or B within TH or VIM, larger fraction of Zone A or B outside TH or VIM, more inferior centroid of Zone A from the VIM, and larger distance between the centroid of Zone A and VIM (p<0.05; Figure 3). The probabilistic maps of Zone A in the study-specific template space are illustrated in Figure 4. As for exam-based side effects, the fractions of Zone B within or outside TH/VIM showed significant differences. Multi-variate regression models based on imaging features achieved AUCs of 0.95 and 0.96 for predicting self-reported and exam-based side effects, respectively. No significant correlation was observed between imaging features and post-treatment FTM scores (Table 1).Discussion
Our results indicate that VIM segmentation using THOMAS in planning FUS targets may reduce side effects. The observed correlation between more inferior and larger post-FUS lesions with presence of gait/balance side effects are consistent with previous studies which showed that lesions inferolateral to the thalamus were associated with increased risk of adverse effects on gait and dysmetria, likely due to corticospinal tract injury.3 Limitations of this study are the small number of patients and the lack of pre-operative tremor scores. Future prospective studies with larger patient numbers and both pre- and post-operative assessments would be required to better evaluate the effectiveness of THOMAS segmentation in improving treatment outcomes.Conclusion
Patient-specific targeting of VIM using THOMAS may be associated with fewer post-MRgFUS side effects, with implications for improved patient outcomes.Acknowledgements
No acknowledgement found.References
1. Su JH, Thomas FT, Kasoff WS, et al. Thalamus Optimized Multi Atlas Segmentation (THOMAS): fast, fully automated segmentation of thalamic nuclei from structural MRI. Neuroimage. 2019 Jul 1;194:272-282.
2. Sudhyadhom A, Haq IU, Foote KD, et al. A high resolution and high contrast MRI for differentiation of subcortical structures for DBS targeting: the Fast Gray Matter Acquisition T1 Inversion Recovery (FGATIR). Neuroimage. 2009 Aug;47 Suppl 2:T44-52.
3. Boutet A, Ranjan M, Zhong J, et al. Focused ultrasound thalamotomy location determines clinical benefits in patients with essential tremor. Brain. 2018 Dec 1;141(12):3405-3414.
Figures