1279
An MRF approach for Simultaneous T1- and PRFS-based 3D MR-Thermometry1Department of Diagnostic and Interventional Radiology, Hannover Medical School, Hannover, Germany
Synopsis
Keywords: Thermometry/Thermotherapy, Thermometry
Motivation: The classical PRFS-based approach to MR-thermometry cannot be used in adipose tissue and is vulnerable to susceptibility artifacts. Nonetheless, the PRFS-based method is quite accurate in aqueous tissue when no severe susceptibility artifacts occur.
Goal(s): A simultaneous measurement of T1 could be used to account for susceptibility artifacts and perform thermometry in adipose tissue.
Approach: An MRF sequence was designed to measure T1 and the PRF at the same time. It was tested during a microwave ablation on a liver phantom.
Results: The PRFS-based temperature maps had a higher temperature accuracy while the T1-based temperature maps performed better in predicting the ablation zone.
Impact: It was shown that simultaneous T1- and PRFS-based 3D-Thermometry is possible using MRF. While the T1 proved to be more robust to susceptibility-induced errors, the PRF had a better temperature accuracy. A combined approach could provide a more accurate MR-thermometry.
Introduction
MRI offers the unique ability of measuring temperature changes in tissue and can therefore be used as guidance during minimally invasive thermal tumor ablations. This is only possible because there are multiple MR-related tissue parameters that are temperature dependent1. Examples are the proton resonance frequency (PRF) or the T1 relaxation time. In practice, mostly the PRF is used for MR-Thermometry. However, the PRF shift with temperature only occurs in aqueous tissue, making it impossible to monitor temperature changes in adipose tissue. Another issue is that PRFS-based methods are highly sensitive to susceptibility artifacts which can severely reduce the quality of the thermometry2. It might therefore be beneficial to have information on other additional parameters like T1. T1 and PRF both vary linearly with temperature in the relevant range for tumor ablations. The PRF change has the advantage of being tissue independent while the T1 change depends on the underlying tissue1. In this work, Magnetic Resonance Fingerprinting (MRF) was used to simultaneously detect temperature-induced changes in T1 and in the PRF.Methods
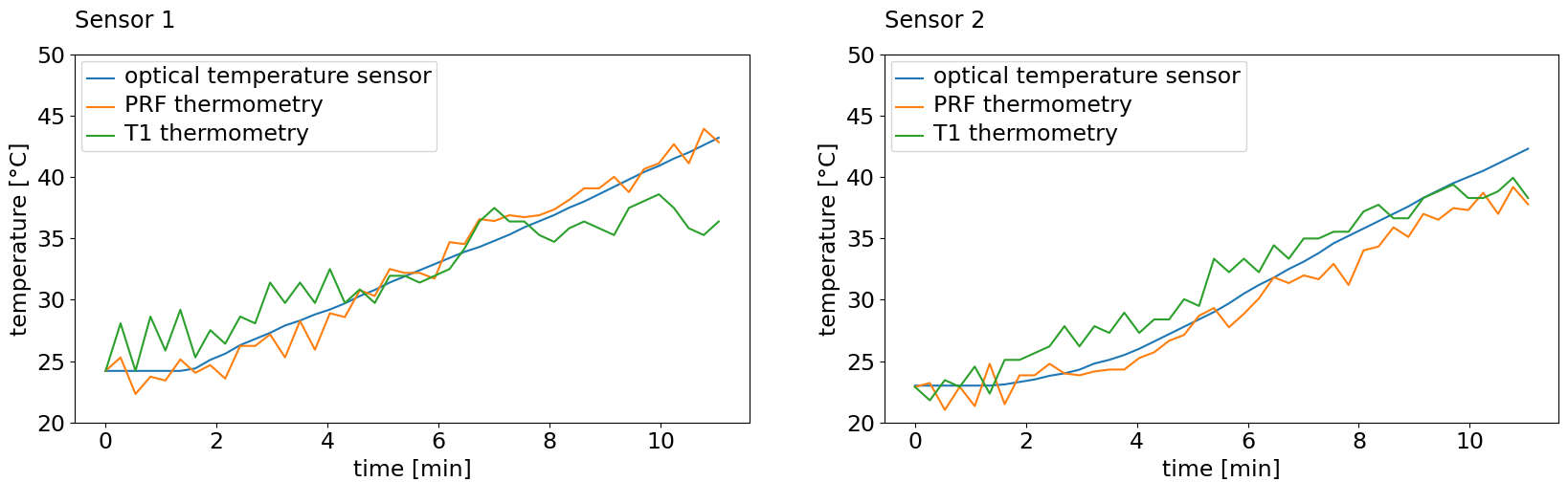
The MRF sequence was designed as a spiral FLASH sequence with varying flip angle (between 5 and 40 °) and TR (between 10 and 20 ms). The flip angle and TR patterns were optimized by minimizing the Cramer-Rao lower bound3. For additional T1 sensitivity, an inversion pulse was played out before the flip angle and TR pattern. The Field of View was 320 x 320 x 40 mm with an isotropic resolution of 2.5 mm and the temporal resolution was 16.17 s. With every TR, the maximum number of echoes were acquired. The sequence was thus sensitive to T1 and the PRF. A dictionary was generated for off-resonance quantification and another dictionary was generated for T1 quantification. The T1 dictionary also accounted for variations in the B1 field as an additional dimension. The dictionaries were compressed in the time domain with a singular value decomposition4. Image reconstruction was done with the BART5 toolbox using parallel imaging and compressed sensing in the linear subspaces of the two dictionaries. Afterwards, dictionary matching was performed by taking the highest inner product between the reconstructed subspace images and the compressed dictionary entries.The temperature accuracy was tested by performing a 10-minute microwave ablation (ECO-100, 80 W) on a liver phantom (bovine liver cast in gelatin, see Fig. 2) while running the MRF sequence on a 1.5 T scanner (Siemens Avanto). Two optical temperature sensors were inserted into the liver in order to get a reference on the temperature. 5 minutes of baseline data were collected before starting the ablation. As suggested in 6, 3.5 minutes of the baseline data were reconstructed together in order to get images with less undersampling. Afterwards, each reconstruction was started with the previous time point as an initial guess. The ablation zone was calculated from the T1- and PRFS-based thermometry with the CEM437 model. For comparison, the ground truth ablation zone was acquired through an inversion recovery sequence (TI 100 ms) and manual segmentation.
Results
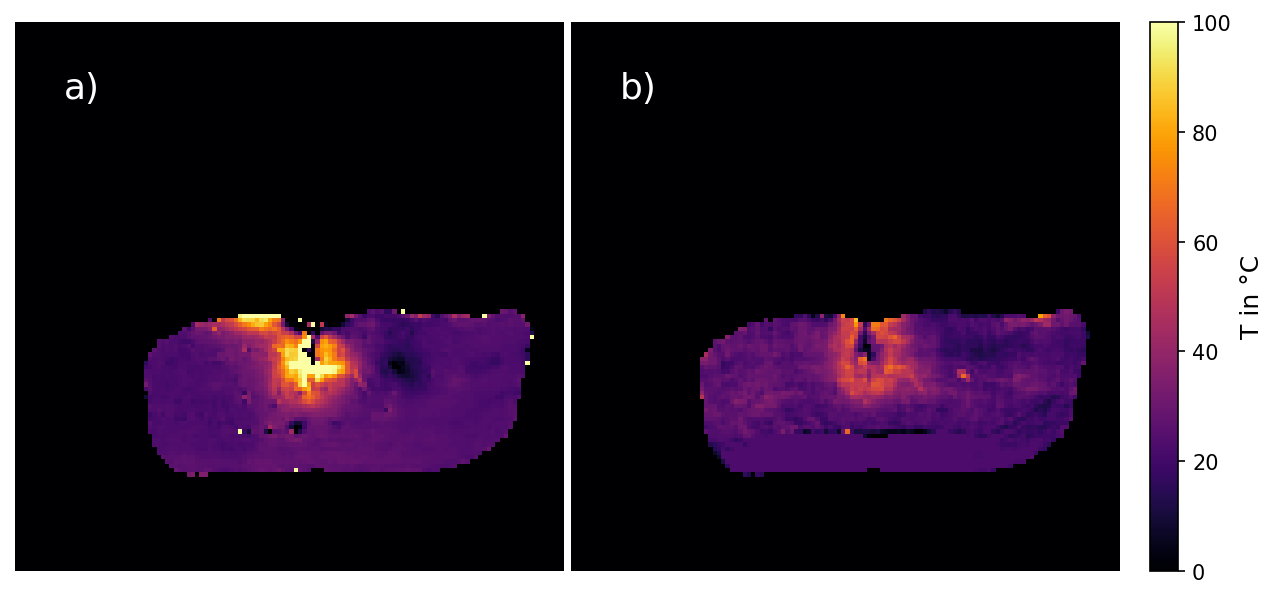
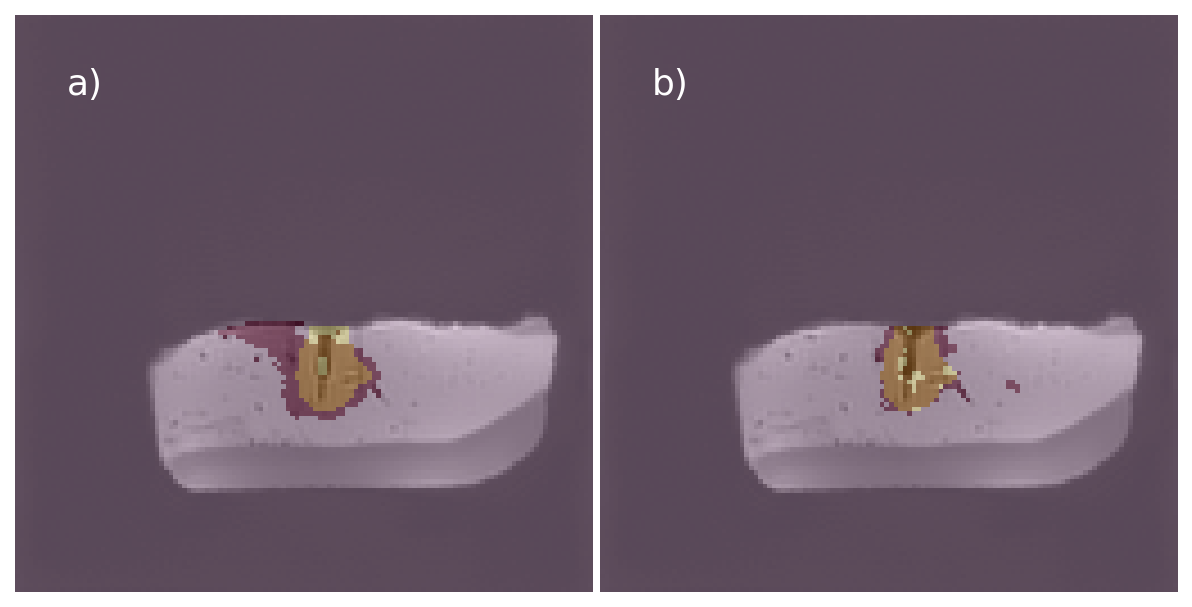
The temperature accuracy of the PRFS-based thermometry compared to the optical temperature sensors was 1.42 ± 1.08 °C and 0.88 ± 0.68 °C. A T1 change of about 1.2% per degree celsius occurred which is in good agreement with literature values1 and the temperature accuracy of the T1-based thermometry was 1.98 ± 1.18 °C and 2.13 ± 1.73 °C. The temperature curves are shown in Fig. 3. The dice score of the ground truth versus the calculated ablation zone was 77.79% for the T1- and 66.27% for the PRFS-based thermometry (see Fig. 4).Discussion
This study has shown that simultaneous T1- and PRFS-based 3D-Thermometry is possible using MRF. Compared to other methods like a variable flip angle8 it does not need a B1 map in advance since the B1 inhomogeneity can be encoded directly in the MRF framework. The PRFS-based temperature maps exhibited a high false positive rate in the calculated ablation zone near larger vessels and the insertion hole of one of the temperature sensors which is probably caused by susceptibility artifacts. The T1-based temperature maps showed to be quite robust to those susceptibility artifacts and could predict the ablation zone significantly better. However, the PRFS-based temperature maps performed better regarding the temperature accuracy in areas without severe susceptibility artifacts and were more stable in non-heated areas. A combined approach could potentially provide a good way of mitigating susceptibility artifacts whilst maintaining a good temperature accuracy.Acknowledgements
This work is funded by the Federal Ministry of Education and Research within the research campus STIMULATE under the grant numbers '13GW0473A' and '13GW0473B'.References
[1] RIEKE, V et al; “MR thermometry; JMRI 2008 27(2) 376–390
[2] SPRINKHUIZEN, S.M. et al; “Temperature-induced tissue susceptibility changes lead to significant temperature errors in PRFS-based MR thermometry during thermal interventions”; Magn. Reson. Med., 64: 1360-1372.
[3] VAN RIEL, M et al.; “Free-breathing abdominal T1 mapping using an optimized MR fingerprinting sequence”; NMR in Biomedicine. 2021
[4] ZHAO, B et al; “Improved magnetic resonance fingerprinting reconstruction with low-rank and subspace modeling”; Magn Reson Med 2018;79(2):933-942
[5] UECKER, M et al; “Berkeley Advanced Reconstruction Toolbox”; Proc. Intl. Soc. Mag. Reson. Med. 23 (2015), S. 2486
[6] GUTT, M et al; “Mitigating undersampling artifacts in magnetic resonance fingerprinting for proton resonance frequency shift based temperature monitoring of microwave ablation”; 2023. Magn. Reson. Mater Phy. 36 (Suppl 1), (2023), S. 233.
[7] PEARCE, JA et al; “Comparative analysis of mathematical models of cell death and thermal damage processes”; International Journal of Hyperthermia 29 (2013), Nr. 4, S. 262–280
[8] SVEDIN, BT et al; “Simultaneous Proton Resonance Frequency Shift Thermometry and T1 Measurements Using a Single Reference Variable Flip Angle T1 Method”; Magn. Reson. Med. 2019; 81: 3138–3152.
Figures