1271
Axonal Diameter Mapping as a biomarker for mTBI as detected by ultrahigh-bvalue DWI in a high performance Head-only gradient system, MAGNUS.1Radiology, Uniformed Services University of the Health Sciences, Bethesda, MD, United States, 2GE Healthcare, Niskayuna, NY, United States, 3Radiology, Walter Reed National Military Medical Center, Bethesda, MD, United States
Synopsis
Keywords: Microstructure, Diffusion/other diffusion imaging techniques, High-performance head-only Gradient
Motivation: Detect a mild traumatic brain injury with a reliable diagnostic for staging disease state and the testing therapies for treating the malady in acute and long term phase.
Goal(s): Develop a MRI biomarker that can be repeated used on patients especially in the warfighter population which have more that 500,000 diagnosed mTBI over the past 30 year.
Approach: Use of diffusion MRI to determine the white matter microstructural state namely the axon diameter.
Results: MAGNUS SE-DWI high-B can detect changes in axon diameter and follow these changes in single subject over time.
Impact: High B-value diffusion imaging (b > 30000 mm2/sec) can detect changes in mild TBI subjects that can be seen to progress through the recovery process. The high-performance gradient system, MAGNUS, (200mT/m, 500T/m/s) scanning without peripheral nerve stimulation in the subject.
Introduction.
Using diffusion weighted MRI to determine integrity and connectivity of white matter fibers in the functioning brain is a robust method of interrogating the microstructure below the resolution of the MR scan. This has been used to excellent effect for examining white matter disease in humans and pre-clinical animal models. Traumatic brain injury is a prevalent problem in the warfighter at the US Department of Defense and a hazard in normal civilian life in accidents such a falls and automobile crashes. For moderate and severe TBI the physiological effects can be seen on most clinical images such as FLAIR, MPRAGE, and DWI. The most common version of TBI is mild TBI which is quite evident from ocular, motor, and behavior testing but does not have a definitive MRI signature that can be detected by neuroradiologists. Looking beyond the standard limits of clinical MRI to underlying microstructure requires a better scanner. The MAGNUS scanner was built to investigate this level of detail for conditions such as mild TBI. The high performance gradient (200 mT/m, 500 mT/m/s) encodes diffusion in a substantially shorter TE preserving SNR and interrogating shorter diffusion lengths. 1 This is used in ultra-high B-value diffusion scans for visualizing only intra-axonal water limited to short radial motions.2 The preserved SNR enables b=30000 DWI scans with sufficent signal to fit the exponential decay model to determine axonal diameter.3,4Experimental
90 subjects were recruited for the study with normal control, acute mild TBI, or chronic TBI status. The recruits were scanned under WRNMMC IRB protocol approval with medical supervision on all subjects. A 3.0 T MRI (GE Healthcare, Waukesha, WI, USA) was used and fitted with a head-only 200 mT/m and 500 T/m/s MAGNUS gradient (GE Research, Niskayuna, NY, USA).1 A 32-channel phased array head coil (NOVA Medical, Wilmington, MA, USA) was used for all experiments. A multi-shell diffusion acquisition was used with total of 4x60=240 encoding directions with b=7,18,25, and 30 ms/μm (echo-spacing=538 ms, Δ/δ=33/19 ms, TE/TR=63/5500 ms, 2.2-mm isotropic resolution, NEX=1, in-plane R=2, scan-time:20 mins). Diffusion encoding directions were uniformly sampled on each shell by enforcing antipodal symmetry. A T1-weighted MPRAGE was also acquired for joint spatial normalization and white matter segmentation.Signal processing: Due to intrinsically low SNR at ultra-high b-values, magnitude reconstruction of dMRI images results in a rectification of the noise floor resulting in inaccurate estimation for model fitting.4 We adopt DCPF which utilizes filter kernels optimized via spatial noise correlation patterns. The output is real-valued data (RVD) that maintains a Gaussian noise distribution. RVD was further corrected for distortion, eddy currents, bulk motion and non-linearity of diffusion-encoding gradients, implemented via a custom reconstruction pipeline.5 Whole brain white matter, gray matter, and CSF segmentations along with registration of the Johns Hopkins University (JHU) ICBM-DTI-81 White-Matter Labeled Atlas to subject space.6
Results
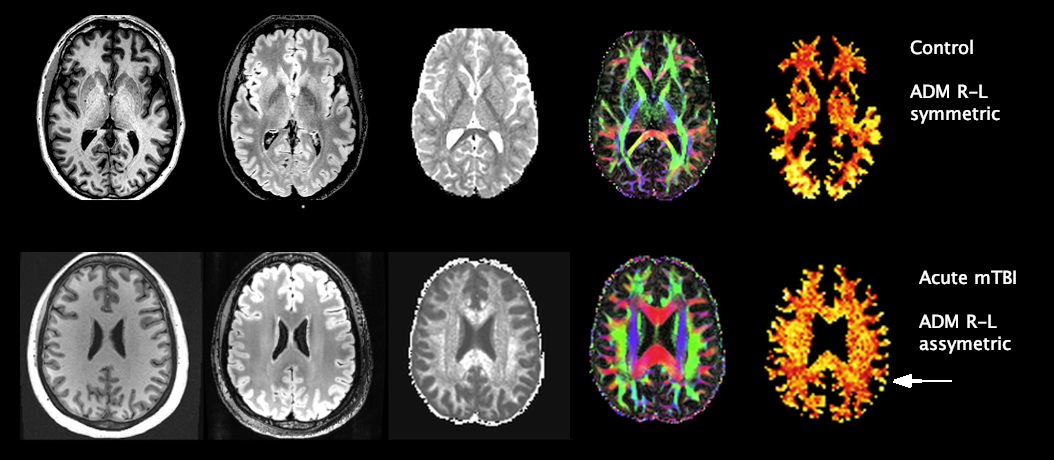
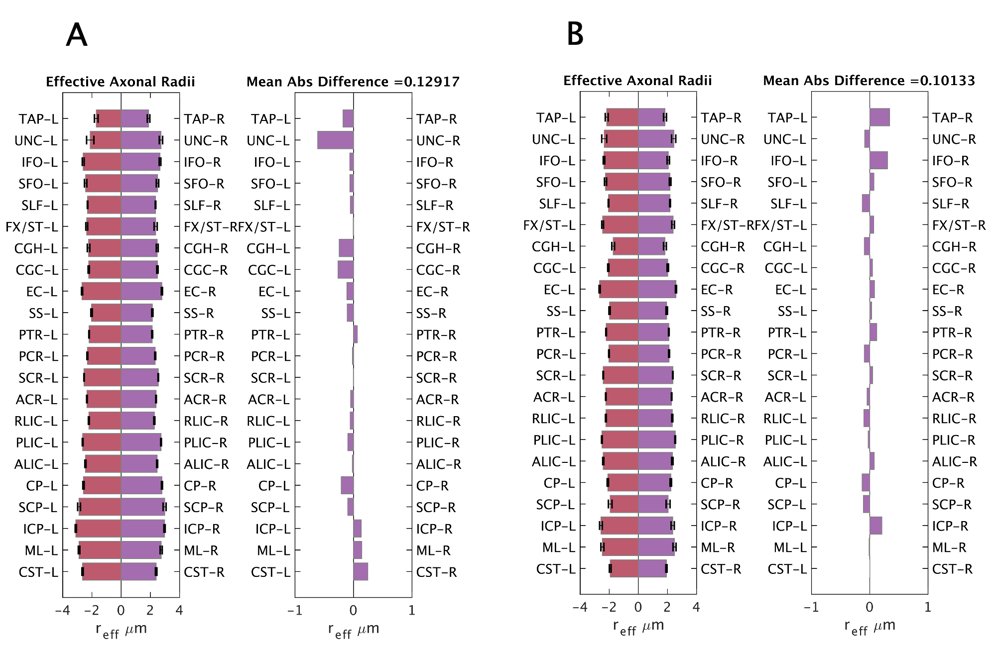
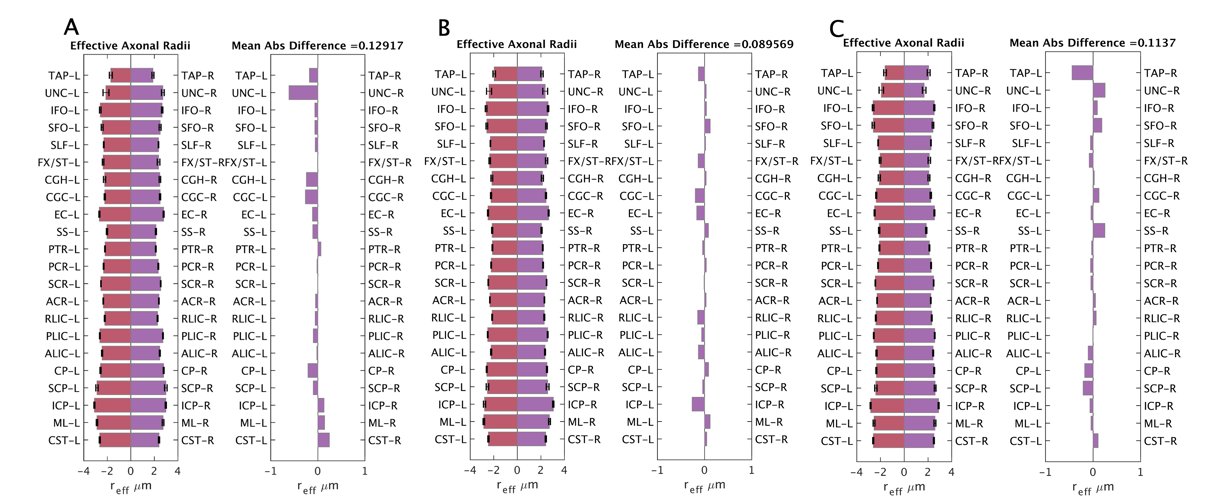
In the acute phase mTBI patients we see changes in the intra-axonal water images or axonal diameter map (ADM) indicating focal changes in the diameter of axons up to 3.5 micrometers in Figure 1 compared to the uninjured control subject. This can be tracked globally by parcellating the ADM volume using the JHI WM atlas.6 As injury sites don’t have a specific locus on all patients we used R-L hemispheric difference between parcels as an indicator of small volume ADM changes. Figure 2 shows the differences between a control subject and acute mTBI subject by assessing the axon diameter differences in R-L paired parcels. This Hemispheric Asymmetric Index (HAI) varies more in acute mTBI subjects as their recovery progresses over time. Three time points are shown in Figure 3 over a time window of approximately 80 days. The HAI shows changes over the time course.Conclusion
Axonal diameter measurements can detect the subtle changes in axon geometry with a mild traumatic brain injury. The utility of this measurement will be further explored in mTBI subjects with other factors such as PTSD and depression. We will be expanding the technique to 3D and higher acquisition rate to reduce patient scanner time and related motion artifacts. The use of multiple time points of axonal diameter imaging may provide a technique to assess the progression of mTBI in some patients.Acknowledgements
Grant funding from NIH U01EB028976, NIH U01EB024450, CDMRP W81XWH-16-2-0054.References
- Foo, T. K. F. et al. Highly efficient head-only magnetic field insert gradient coil for achieving simultaneous high gradient amplitude and slew rate at 3.0T (MAGNUS) for brain microstructure imaging. Magnetic Resonance in Medicine 83, 2356–2369(2020).
- Veraart, J. et al. Noninvasive quantification of axon radii using diffusion MRI. eLife 9, e49855 (2020).
- Assaf, Y., Blumenfeld-Katzir, T., Yovel, Y. & Basser, P. J. Axcaliber: A method for measuring axon diameter distribution from diffusion MRI. Magnetic Resonance in Medicine 59, 1347–1354 (2008)
- Abad, N. et. al. Axonal Diameter Mapping using High Performance Gradients: Feasibility study and Repeatability off Estimates. In Proceedings of the 31st Annual Meeting of the ISMRM, Toronto, CA, 2023. Abstract 760.
- Sprenger, T., Sperl, J. I., Fernandez, B., Haase, A. & Menzel, M. I. Real valued diffusion-weighted imaging using decorrelated phase filtering. Magnetic Resonance in Medicine 77, 559–570 (2017).
- Quachtran, B., Joshi, A.A., Bhushan, C., Leahy, R.M. and Shattuck, D.W., Combined T1-Diffusion MRI Registration, OHBM, pp2506, 2018.
- Oishi, K. et al. Human brain white matter atlas: Identification and assignment of common anatomical structures in superficial white matter. NeuroImage 43, 447–457 (2008).
Figures