1269
ZOOM and enhance: ZOnally magnified Oblique Multi-slice for cardiac DTI with ultra-strong gradients1Leeds Institute of Cardiovascular and Metabolic Medicine, University of Leeds, Leeds, United Kingdom, 2These Authors contributed equally to this work, Leeds, United Kingdom, 3Cardiff University Brain Research Imaging Centre (CUBRIC), School of Psychology, Cardiff University, Cardiff, United Kingdom, 4CIBM Center for Biomedical Imaging, EPFL CIBM-AIT, EPFL Lausanne, Lausanne, Switzerland, 5Siemens Healthcare Ltd, Camberly, United Kingdom, 6Siemens Healthcare GmbH, Erlangen, Germany, 7Medical Radiation Physics, Clinical Sciences Lund, Lund University, Lund, Sweden
Synopsis
Keywords: Diffusion Acquisition, Diffusion Tensor Imaging, Cardiac diffusion MRI, strong gradients, ZOOM, reduced field of view, non co-planar rf
Motivation: Cardiac diffusion tensor imaging (cDTI) with echo-planar imaging (EPI) requires long readouts to avoid aliasing artefacts if 2D-selective rf-pulses are not available. These prolong the echo time (TE) and increasing sensitivity to off-resonance artefacts.
Goal(s): The reduction of the excited and refocused field of view in the phase direction to reduce TE and sensitivity to image artefacts in cDTI.
Approach: We combine ZOnally-magnified Oblique Multi-slice (ZOOM) EPI (i.e. tilting the slice orientation of the refocussing rf-pulse) with ultra-strong gradients.
Results: We were able to reduce TE (from ~70 ms to 59 ms) in cDTI considerably by reducing the FoV and using strong gradients.
Impact: We reduced the echo time in cDTI with ultra-strong gradients which will allow us to use more advanced diffusion acquisitions (higher b-values and/or different gradient waveforms) in the heart in vivo.
Introduction
Cardiac diffusion tensor imaging (cDTI) was recently combined with ultra-strong gradients1. Although this work demonstrated the potential for higher order motion compensation and / or higher b-values in cDTI, it failed to reduce the echo time (TE) considerably, even for more standard diffusion weightings. This was largely attributable to the need to acquire a larger field of view (FoV), and thus longer readouts, to avoid image artefacts.This can be ameliorated with reduced FoV acquisitions, which can be achieved in different ways2, like the use of 2-dimensional spatially selective rf-pulses3,4 (not readily available on the MRI used here), or by angulating one of the slice directions of the rf-pulses relative to the phase encoding direction of the EPI. This angulation can be 90° 5–7, or <90° (ZOnally magnified Oblique Multi-slice, ZOOM)8–10, whereas the latter approach gives the opportunity for multi-slice acquisitions without further modifications to the sequence. This approach was used previously in cDTI6,10, but was not investigated further.
Here we present the combination of ZOOM with ultra-strong gradients to achieve shorter TE for typical b-values in cDTI with a spin-echo EPI sequence, while keeping the ability to acquire multiple slices.
Methods
Data were acquired with a prototype EPI sequence 11 for a 3T MRI Connectom (Siemens Healthineers) with maximum gradient amplitude 300 mT/s and maximum slew rate 200 T/m/s, using free gradient waveforms (FWF) for diffusion encoding. We modified the sequence to be ablePossible angles and slice thicknesses were examined in a spherical water phantom with b-values 100 and 500 s/mm2 and 6 directions each.
Additionally, 3 volunteers who had given informed written consent were scanned. The diffusion weightings consisted of 3 directions with b = 100 s/mm2 (12 repetitions) and 30 directions with b = 500 s/mm2 (6 repetitions). The tilting angle was 15° and the refocusing slice thickness 20 mm. We added saturation bands to further suppress signal from outside the volume of interest. TE was 59 ms, and TR 3-RR-intervals.
Other imaging parameters were (for phantom and in vivo): FoV (acquired) = 320$$$\times$$$120 mm2, in-plane resolution = 2.3$$$\times$$$ 2.3 mm2, bandwidth = 2012 Hz/pixel, partial Fourier 7/8, 3 slices with 8 mm thickness (excitation) and 8 mm gap.
Both magnitude and phase images were acquired and combined to remove phase variations15, afterwards the images were rigidly registered, and outliers were removed16,17. A diffusion tensor was estimated in each voxel with a weighted least-squares approach.
Results
The phantom measurements show clear aliasing artefacts in the images and intensity profiles for low angles which are not present for larger angles (Figure 2a and 2b). The profiles for 15° \ 20 mm acquisitions align well for the different directions at the same b-value (Figure 2c).The reduction of aliasing artefacts due to ZOOM can also be seen in vivo (Figure 3).
Figure 4 shows orientationally averaged images and the corresponding cDTI results (I.e. MD, FA, HA, E2A) for one volunteer.
In Table 1, the average MD, FA and absolute E2A are listed for all volunteers and slices.
Discussion and Conclusion
We present the combination of ZOOM with ultra-strong gradients to demonstrate in vivo multi-slice cDTI at shorter TE (59 ms instead of ~70 ms) than usually possible for free breathing spin-echo acquisitions. The SNR gain from the shorter TE (T2=50 ms) is roughly the same as the SNR loss due to shorter readout durations (26 ms instead of 41 ms), leading to similar expected SNR.Tilted slice approaches were shown to be useful in different organs8,18–20. In the heart lower tilt angles were used before6,10. For spin echo cDTI, rf based approaches21–25 or 90° angulation7,26–31 are more common.
The slice tilting angle used here is lower than in the original ZOOM publications8,9. This is due to the smaller slice gap compared to slice thickness. Comparing the setup to other implementations is difficult, as they are not always reported. The phantom results suggested that our settings were suitable.
The in vivo results show a clear reduction in image artefacts when using ZOOM. The cDTI results are in the same range as previously reported6,7,32,33.
We demonstrate that ZOOM is a viable alternative to 2D selective rf-pulses to achieve a reduced FoV acquisition in cDTI which allows us to leverage the ultra-strong gradient system to a larger extent and reduce TE.
Acknowledgements
We thank Siemens Healthcare for the pulse sequence development environment. This work was supported by Wellcome Trust Investigator Award (219536/Z/19/Z), EPSRC (EP/M029778/1), The Wolfson Foundation, the British Heart Foundation (PG/19/1/34076), and the Swiss National Science Foundation (#202962).
References
1. Afzali M, Mueller L, Coveney S, et al. Cardiac diffusion MRI using Connectom scanner. In: Proc. Intl. Soc. Mag. Reson. Med. 31 . Toronto; 2023:4284.
2. Wargo CJ, Moore J, Gore JC. A comparison and evaluation of reduced-FOV methods for multi-slice 7 T human imaging. Magn Reson Imaging. 2013;31(8):1349-1359.
3. Rieseberg S, Frahm J, Finsterbusch J. Two-dimensional spatially-selective RF excitation pulses in echo-planar imaging. Magn Reson Med. 2002;47(6):1186-1193.
4. Bottomley PA, Hardy CJ. Two‐dimensional spatially selective spin inversion and spin‐echo refocusing with a single nuclear magnetic resonance pulse. J Appl Phys. 1987;62(10):4284-4290.
5. Feinberg DA, Hoenninger JC, Crooks LE, Kaufman L, Watts JC, Arakawa M. Inner volume MR imaging: technical concepts and their application. https://doi.org/101148/radiology15634023236. 1985;156(3):743-747.
6. Stoeck CT, Von Deuster C, GeneT M, Atkinson D, Kozerke S. Second-order motion-compensated spin echo diffusion tensor imaging of the human heart. Magn Reson Med. 2016;75(4):1669-1676.
7. Aliotta E, Moulin K, Magrath P, Ennis DB. Quantifying precision in cardiac diffusion tensor imaging with second-order motion-compensated convex optimized diffusion encoding. Magn Reson Med. 2018;80(3):1074-1087.
8. Wheeler-Kingshott CAM, Parker GJM, Symms MR, et al. ADC mapping of the human optic nerve: Increased resolution, coverage, and reliability with CSF-suppressed ZOOM-EPI. Magn Reson Med. 2002;47(1):24-31.
9. Symms M, Wheeler-Kingshott C, Parker G, Barker G. ZOnally-magnified Oblique Multislice (ZOOM) EPI. Proc Intl Soc Mag Reson Med 8. 2000:160.
10. Stoeck CT, Kalinowska A, Von Deuster C, et al. Dual-Phase Cardiac Diffusion Tensor Imaging with Strain Correction. PLoS One. 2014;9(9):e107159.
11. Szczepankiewicz F, Sjölund J, Ståhlberg F, Lätt J, Nilsson M. Tensor-valued diffusion encoding for diffusional variance decomposition (DIVIDE): Technical feasibility in clinical MRI systems. PLoS One. 2019;14(3):e0214238.
12. Sjölund J, Szczepankiewicz F, Nilsson M, Topgaard D, Westin CF, Knutsson H. Constrained optimization of gradient waveforms for generalized diffusion encoding. Journal of Magnetic Resonance. 2015;261:157-168.
13. Szczepankiewicz F, Westin CF, Nilsson M. Maxwell-compensated design of asymmetric gradient waveforms for tensor-valued diffusion encoding. Magn Reson Med. 2019;82(4):1424-1437.
14. Szczepankiewicz F, Sjölund J, Dall’Armellina E, et al. Motion-compensated gradient waveforms for tensor-valued diffusion encoding by constrained numerical optimization. Magn Reson Med. 2021;85(4):2117-2126.
15. Eichner C, Cauley SF, Cohen-Adad J, et al. Real diffusion-weighted MRI enabling true signal averaging and increased diffusion contrast. Neuroimage. 2015;122:373-384.
16. Marstal K, Berendsen F, Staring M, Klein S. SimpleElastix: A User-Friendly, Multi-lingual Library for Medical Image Registration. IEEE Computer Society Conference on Computer Vision and Pattern Recognition Workshops. December 2016:574-582.
17. Coveney S, Kelly C, Teh I, et al. Semi-Automated Rejection of Corrupted Images in Cardiac Diffusion Tensor Imaging. In: Proc. Intl. Soc. Mag. Reson. Med. 31. Toronto; 2023.
18. Sartoretti E, Sartoretti-Schefer S, van Smoorenburg L, et al. Single shot zonal oblique multislice SE-EPI diffusion-weighted imaging with low to ultra-high b-values for the differentiation of benign and malignant vertebral spinal fractures. Eur J Radiol Open. 2021;8:100377.
19. Reischauer C, Wilm BJ, Froehlich JM, et al. High-resolution diffusion tensor imaging of prostate cancer using a reduced FOV technique. Eur J Radiol. 2011;80(2):e34-e41.
20. Reischauer SS, Czell D, Wyss M, et al. Diffusion-Weighted Zonal Oblique Multislice–EPI Enhances the Detection of Small Lesions with Diffusion Restriction in the Brain Stem and Hippocampus: A Clinical Report of Selected Cases. American Journal of Neuroradiology. 2018;39(7):1255-1259.
21. Gorkum RJH van, Guenthner C, Koethe A, Stoeck CT, Kozerke S. Characterization and Correction of Diffusion Gradient-Induced Eddy Currents in Second-Order Motion-Compensated Echo-Planar and Spiral Cardiac DTI. Magn Reson Med. August 2022. doi:10.1002/MRM.29378
22. Nguyen CT, Christodoulou AG, Coll-Font J, et al. Free-breathing diffusion tensor MRI of the whole left ventricle using second-order motion compensation and multitasking respiratory motion correction. Magn Reson Med. 2021;85(5):2634-2648.
23. Lasič S, Szczepankiewicz F, Dall’Armellina E, et al. Motion-compensated b-tensor encoding for in vivo cardiac diffusion-weighted imaging. NMR Biomed. 2020;33(2):e4213.
24. Coll-Font J, Chen S, Eder RA, Nguyen CT. Directions or Averages? An Ablation Study for in vivo Cardiac DTI. In: Proc. Intl. Soc. Mag. Reson. Med. 29. ; 2021:3650.
25. Teh I, Nguyen C, Kelly C, et al. Optimisation of diffusion encoding schemes for in vivo cardiac DTI. In: Proc. Intl. Soc. Mag. Reson. Med. 27. Montreal; 2019:2034.
26. Coll-Font J, Chen S, Eder R, et al. Manifold-based respiratory phase estimation enables motion and distortion correction of free-breathing cardiac diffusion tensor MRI. Magn Reson Med. 2022;87(1):474-487.
27. Moulin K, Croisille P, Viallon M, Verzhbinsky IA, Perotti LE, Ennis DB. Myofiber strain in healthy humans using DENSE and cDTI. Magn Reson Med. 2021;86(1):277-292.
28. Scott AD, Nielles-Vallespin S, Ferreira PF, et al. An in-vivo comparison of stimulated-echo and motion compensated spin-echo sequences for 3 T diffusion tensor cardiovascular magnetic resonance at multiple cardiac phases. Journal of Cardiovascular Magnetic Resonance. 2018;20(1):1-15.
29. Khalique Z, Scott AD, Ferreira PF, Nielles-Vallespin S, Firmin DN, Pennell DJ. Diffusion tensor cardiovascular magnetic resonance in hypertrophic cardiomyopathy: a comparison of motion-compensated spin echo and stimulated echo techniques. Magnetic Resonance Materials in Physics, Biology and Medicine. 2020;33(3):331-342.
30. Gotschy A, Von Deuster C, Van Gorkum RJH, et al. Characterizing cardiac involvement in amyloidosis using cardiovascular magnetic resonance diffusion tensor imaging. Journal of Cardiovascular Magnetic Resonance. 2019;21(1):1-9.
31. Spinner GR, Von Deuster C, Tezcan KC, Stoeck CT, Kozerke S. Bayesian intravoxel incoherent motion parameter mapping in the human heart. Journal of Cardiovascular Magnetic Resonance. 2017;19(1):1-14.
32. Lasič S, Szczepankiewicz F, Dall’Armellina E, et al. Motion-compensated b-tensor encoding for in vivo cardiac diffusion-weighted imaging. NMR Biomed. 2020;33(2):e4213.
33. Nguyen C, Fan Z, Sharif B, et al. In vivo three-dimensional high resolution cardiac diffusion-weighted MRI: A motion compensated diffusion-prepared balanced steady-state free precession approach. Magn Reson Med. 2014;72(5):1257-1267.
Figures
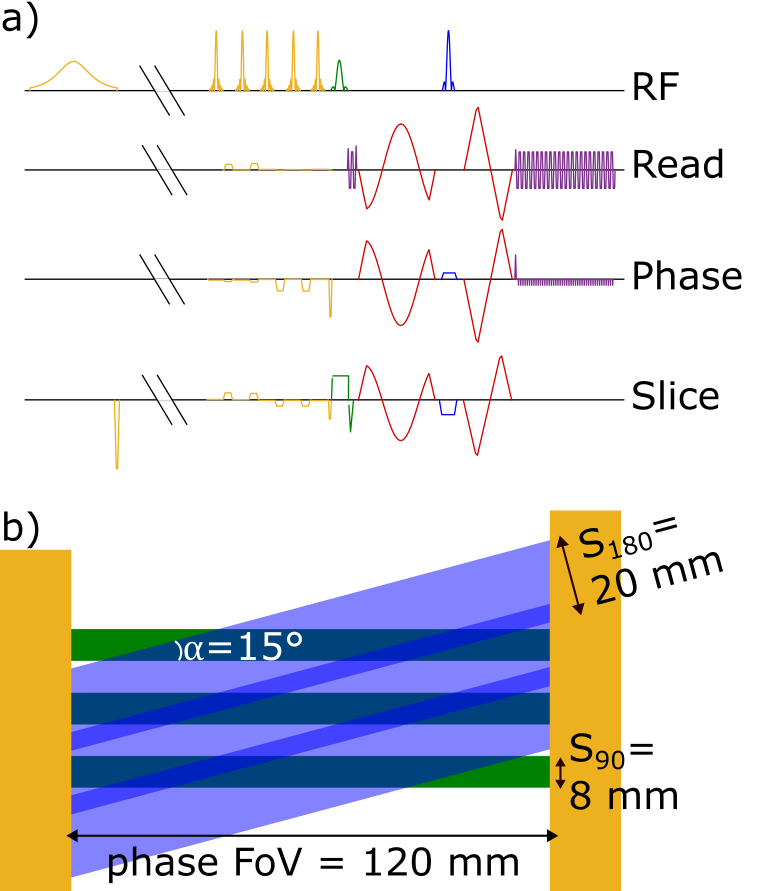
Figure 1: Sequence scheme and slice geometry. a) Spin echo sequence, including fat saturation and spatial saturation bands (yellow), excitation (green), diffusion encoding (red), refocusing (blue) and readout (purple). The SPAIR inversion time is cut from the timeline for a more concise presentation; slice selection gradients are exaggerated for better visibility. b) Slice orientation for excitation (green) and refocusing (blue) including the slice thickness and rotation angle. Saturation bands are shown in yellow and are extending further out to cover the rest of the body.
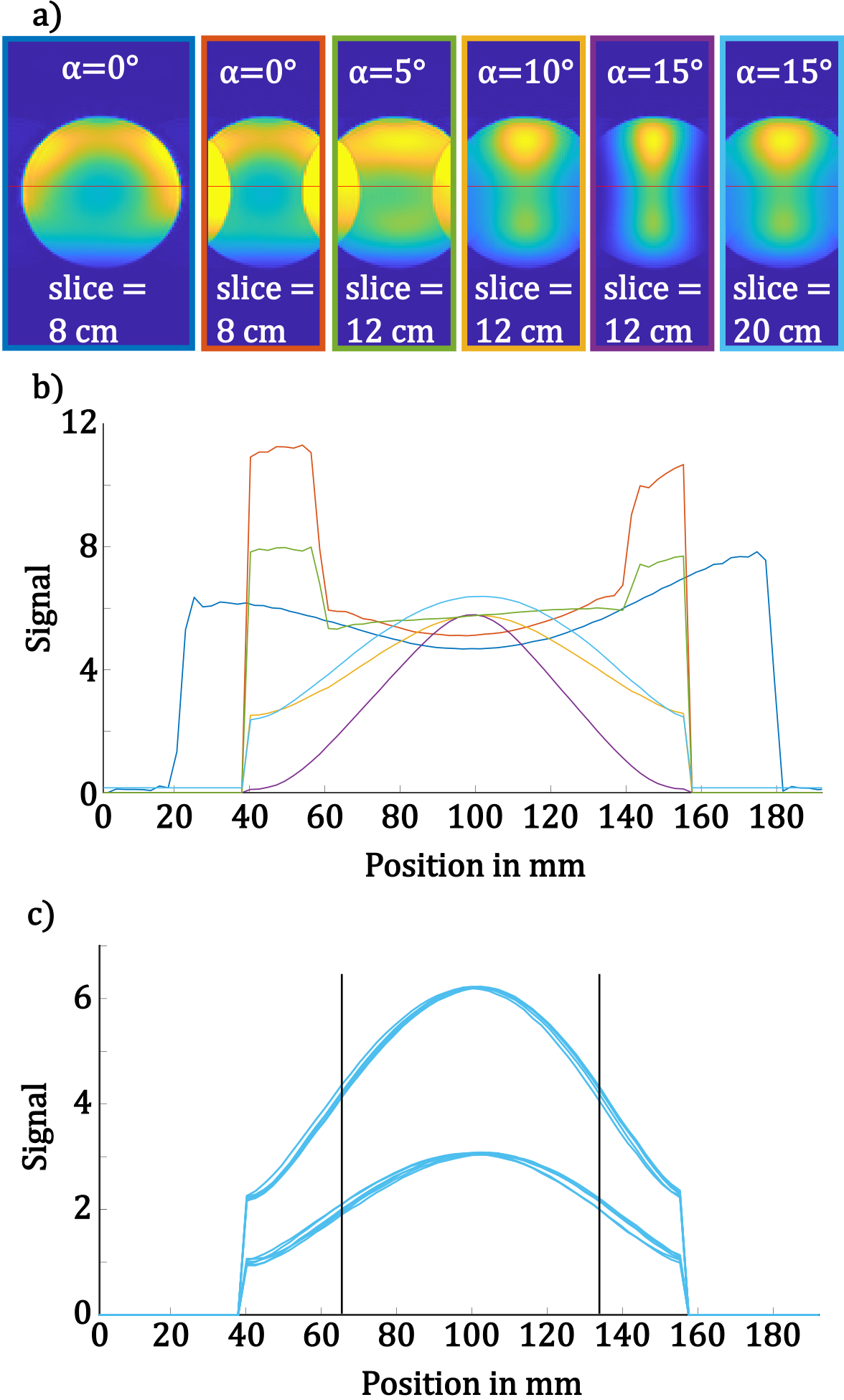
Figure 2: Phantom Results. a) Example images for a full FoV acquisition and multiple tilting angles and slice thicknesses of the refocusing rf-pulse. b) Signal profiles for the images in a) along the red line. The signals were scaled according to the mean over standard deviation (SNR surrogate) in the centre of the image. The line colours match the borders in a). c) Signal profiles for the 6 low and 6 high b-value acquisitions with a tilting angle of 15° and slice thickness of the refocusing rf-pulse of 20 mm (rightmost in a)). The vertical lines indicate the typical size of the left ventricle.
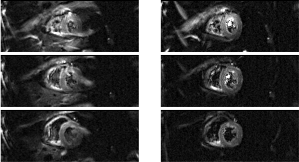
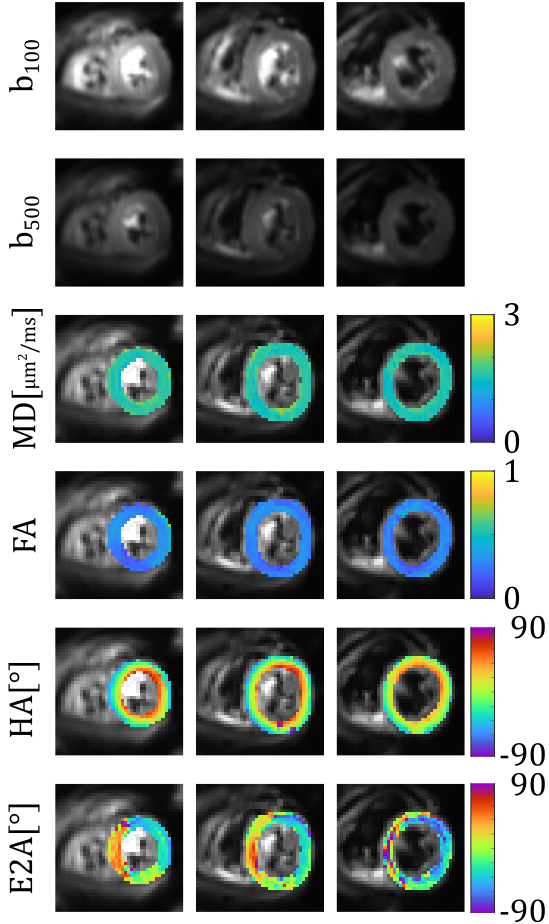
Figure 4: Diffusion weighted images and fitting results for 1 volunteer. The top two rows show the directional averaged diffusion weighted images for b = 100 and 500 s/mm2. The bottom four rows show maps of different DTI parameters for the same volunteer, i.e. mean diffusivity (MD), fractional anisotropy (FA), helix angle (HA), secondary eigenvector angle (E2A).

Table 1: Mean $$$\pm$$$ standard deviation of DTI parameters, mean diffusivity (MD), fractional anisotropy (FA), and absolute value of the secondary eigenvector angle (abs(E2A)), over the myocardium of the left ventricle.