1267
Quantifying microscopic anisotropy in the human heart in vivo using ultra-strong gradients1Leeds Institute of Cardiovascular and Metabolic Medicine, University of Leeds, Leeds, United Kingdom, 2Cardiff University Brain Research Imaging Centre (CUBRIC), School of Psychology, Cardiff University, Cardiff, United Kingdom, 3These authors contributed equally to this work, University of Leeds, Leeds, United Kingdom, 4Siemens Healthcare Ltd, Camberly, United Kingdom, 5Siemens Healthcare GmbH, Erlangen, Germany, 6Medical Radiation Physics, Clinical Sciences Lund, Lund University, Lund, Sweden
Synopsis
Keywords: DWI/DTI/DKI, Diffusion/other diffusion imaging techniques, Cardiac diffusion MRI, microscopic anisotropy, strong gradients, tensor-valued diffusion encoding, Diffusion Kurtosis imaging
Motivation: Tensor-valued diffusion encoding has been shown to provide more information on tissue microstructure than conventional diffusion weighting/tensor imaging.
Goal(s): Quantifying microscopic anisotropy, isotropic and anisotropic kurtosis in a human heart in vivo with a TE commonly used for DTI.
Approach: We used strong gradients ($$$\mathrm{G_{max}=300\,mT/m}$$$) in combination with linear, planar, and spherical tensor encoding with up to second-order motion compensation to achieve $$$\mathrm{b_{max} = 1500\,s/mm^2}$$$ with a TE of 74 ms.
Results: Estimated diffusion metrics matched the values reported in the literature while a shorter echo time was achieved due to the strong gradients used resulting in increased SNR and therefore image quality.
Impact: We implemented tensor-valued diffusion encoding with ultra-strong gradients for in vivo cardiac diffusion MRI in humans. This allows us to quantify microscopic anisotropy and kurtosis.
Introduction
Cardiac diffusion MRI (dMRI) is a non-invasive technique for characterization of the myocardial tissue. Currently, diffusion tensor imaging (DTI)1 is the most common method in cardiac dMRI studies. DTI characterizes the diffusion process using a single diffusion tensor in each voxel. It cannot account for non-Gaussian diffusion resulting from restrictions, or heterogeneous tissue density2,3. Furthermore, for a heterogeneous or complex tissue, DTI has poor sensitivity and specificity4,5. Quantifying microscopic anisotropy and multi-Gaussian diffusion offers the potential for greater insights into tissue than methods described previously. This can be achieved by performing tensor-valued diffusion encoding at high b-values. Previously, Teh et al.6 used linear, planar, and spherical b-tensor encoding (LTE, PTE, and STE), and analyzed data using the q-space trajectory imaging (QTI) framework7 on a clinical system with $$$\mathrm{G_{max} = 80 mT/m}$$$. We extend this approach to the Connectom scanner, to capitalise on ultra-strong 300 mT/m gradients for shortening TE. By using multiple b-tensor shapes, parameters such as mean diffusivity (MD), fractional anisotropy (FA), microscopic FA ($$$\mathrm{\mu}$$$FA), and the isotropic, anisotropic, and total kurtosis ($$$\mathrm{K_{iso}, \, K_{aniso}, \, and \, K_{total}}$$$) can be estimated3,6-13.Methods
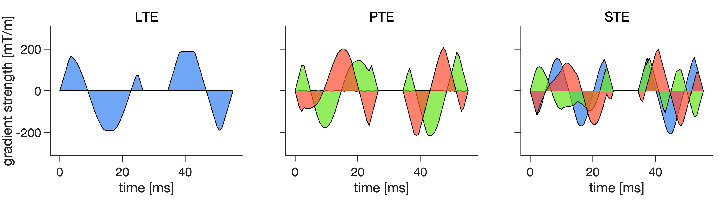
Cardiac diffusion-weighted images (cDWI) were acquired in two healthy volunteers with written consent on a Connectom 3T MR imaging system ($$$\mathrm{G_{max} = 300 \, mT/m}$$$). cDWI was performed with a prototype pulse sequence14 using an EPI readout and user-defined gradient waveforms designed using the NOW toolbox15-17 (https://github.com/jsjol/NOW) to provide Maxwell- and second-order motion-compensated waveforms for LTE, PTE, and STE (Figure 1). Acquisition parameters were: TR=3RR-intervals, TE=74 ms, field‐of‐view=$$$320 \times 144 \,\mathrm{mm^2}$$$, resolution=$$$2.7 \times 2.7 \, \times 8 \mathrm{mm^3}$$$, slice gap=8 mm, 3 short axis slices, partial Fourier=7/8, no parallel imaging, bandwidth=2084 Hz/pixel. LTE and PTE data sets comprised 4 b-values [b = 100, 500, 1000, 1500 $$$\mathrm{s/mm^2}$$$] in 30 directions per shell with 3 repetitions, except for the lowest b-value which only had 1 repetition. The STE data set had b = 100, 500, and 1000 $$$\mathrm{s/mm^2}$$$. The total acquisition time was around one hour. Both magnitude and phase data were collected and used to generate the complex-valued images. Phase variations was removed18 and real-valued diffusion-weighted images were then corrected for motion by a 2D rigid image registration and the outlier images were removed19,20. MD, FA, $$$\mathrm{\mu FA}$$$, isotropic and anisotropic kurtosis ($$$\mathrm{K_{iso}}$$$ and $$$\mathrm{K_{aniso}}$$$) and total kurtosis ($$$\mathrm{K_{total}}$$$) were calculated21.Results
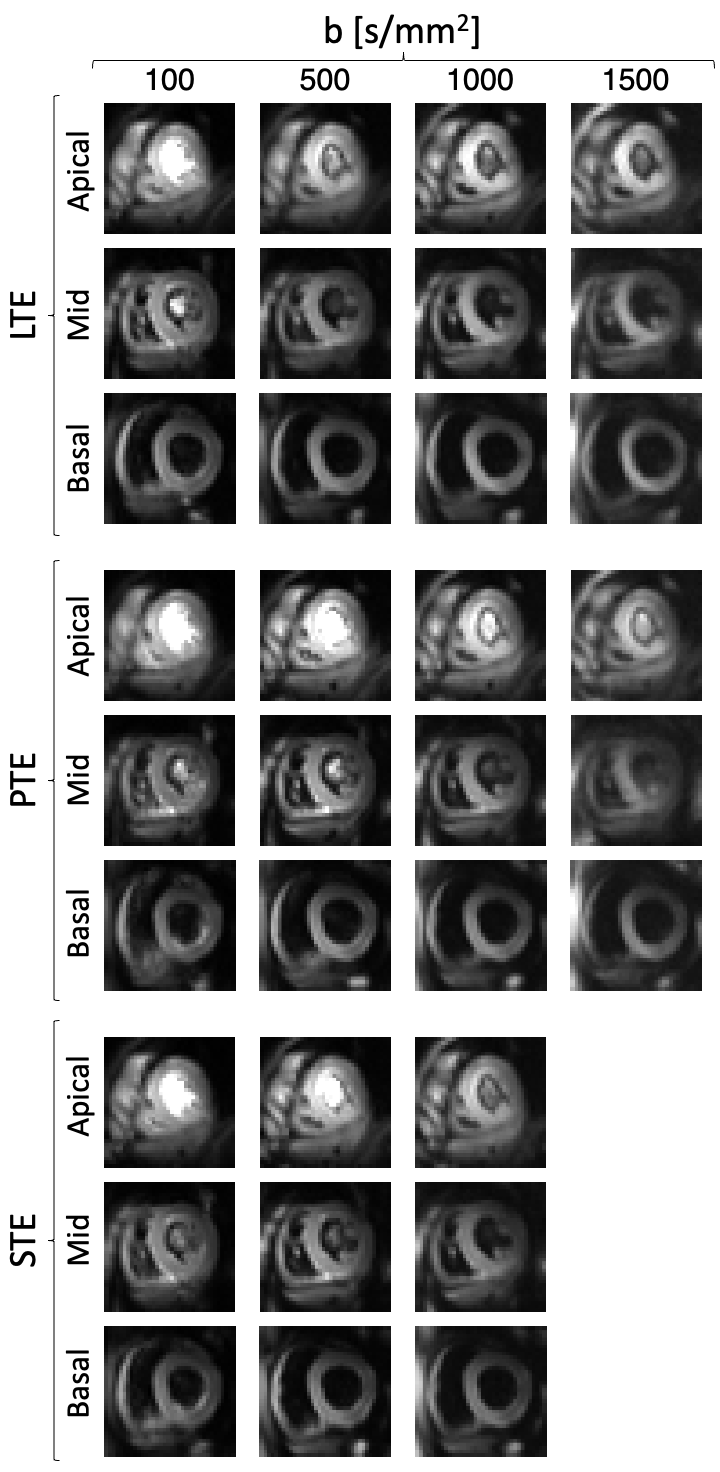
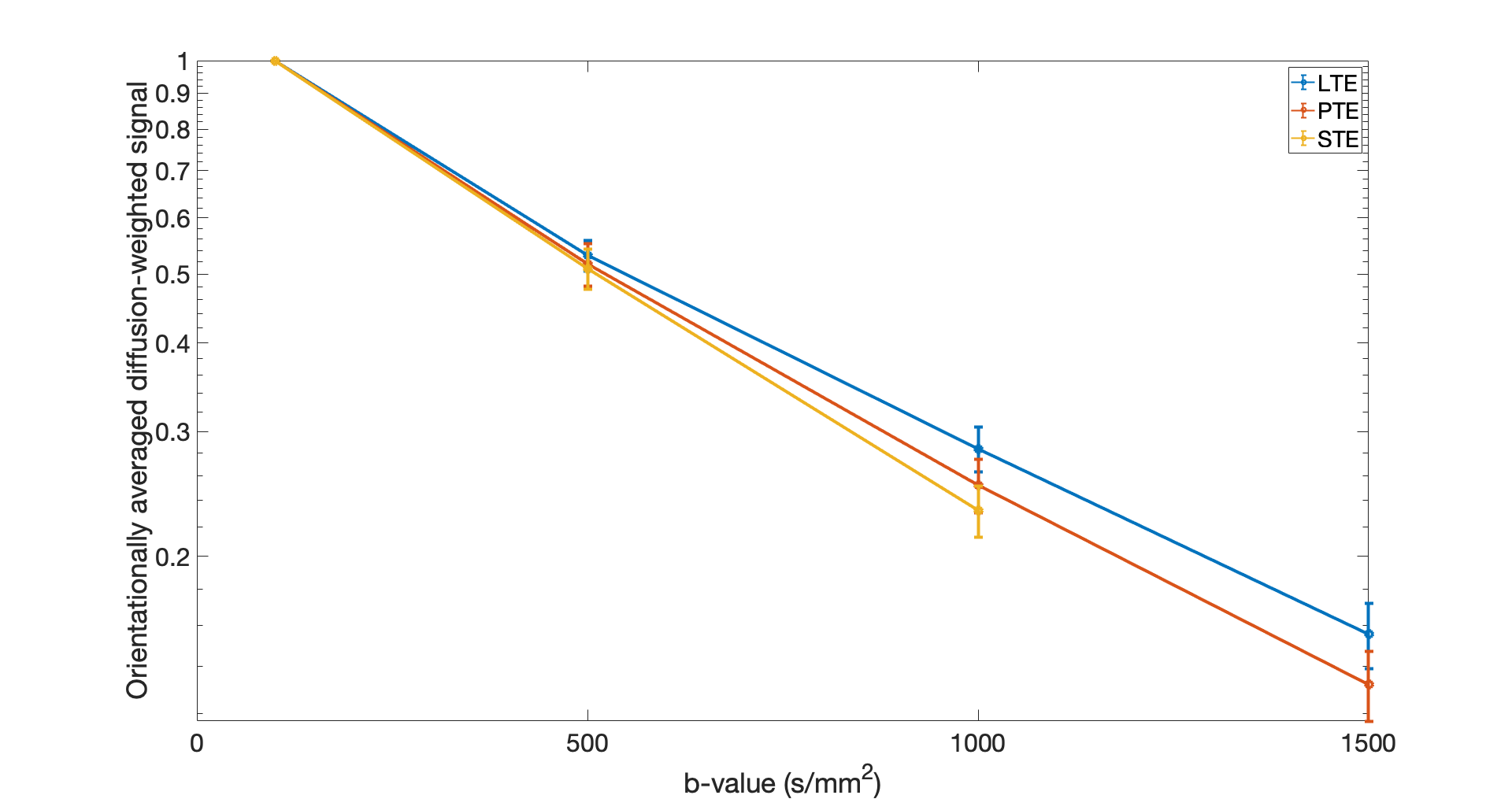
Figure 2 shows orientationally-averaged diffusion-weighted images from LTE, PTE, and STE acquisitions with different b-values.The signal decay curves for LTE, PTE, and STE, averaged over the myocardium of the left ventricle (LV) (Figure 3) are completely separated at b = 1000 $$$\mathrm{s/mm^2}$$$. The difference between PTE and LTE signal is increased for b = 1500 $$$\mathrm{s/mm^2}$$$.
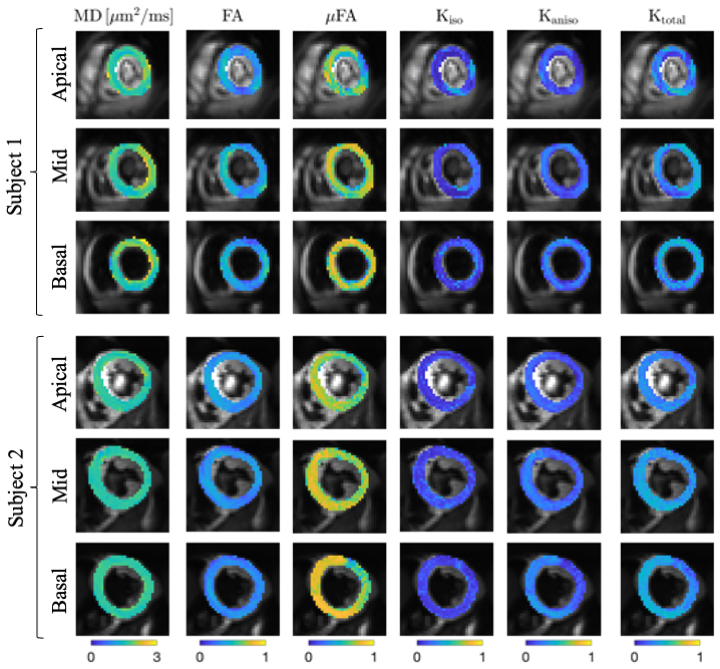
The parameter maps (MD, FA, $$$\mathrm{\mu FA}$$$, $$$\mathrm{K_{iso}}$$$, $$$\mathrm{K_{aniso}}$$$, and $$$\mathrm{K_{total}}$$$) from the voxel-wise diffusion fit are shown in Figure 4 for Subject 1 (three first rows) and Subject 2 (three last rows).
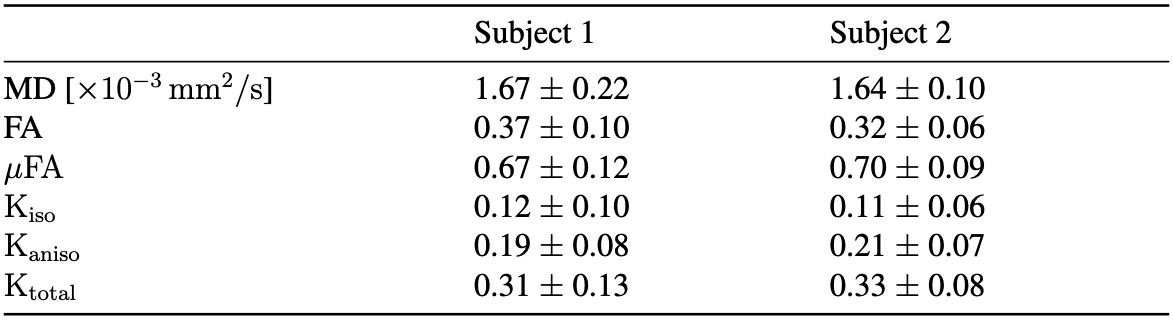
The mean and standard deviation of diffusion metrics over the LV (Table 1) for the two subjects are in good agreement with each other.
Discussion and Conclusion
We quantified $$$\mathrm{\mu FA}$$$, $$$\mathrm{K_{iso}}$$$ and $$$\mathrm{K_{aniso}}$$$ in the human heart in vivo using ultra-strong gradients ($$$\mathrm{G_{max} = 300 \, mT/m}$$$). Our results show that $$$\mathrm{\mu FA > FA}$$$, which indicates the presence of orientation dispersion4,6-8. The relatively small value of $$$\mathrm{K_{iso}}$$$ reflects low variation in isotropic diffusivity3 which is expected for healthy myocardium6.The average value of MD, FA, $$$\mathrm{K_{iso}}$$$, $$$\mathrm{K_{aniso}}$$$, and $$$\mathrm{K_{total}}$$$ in our work are in line with the values reported by Teh, et al.6 while our estimated $$$\mathrm{\mu FA}$$$ is slightly higher ($$$\mathrm{\sim 0.7}$$$ compared to $$$\mathrm{\sim 0.4}$$$). The experiment setup in this study is slightly different than Teh et al.'s6. The results reported here are from a small sample size (two subjects). We have a smaller voxel size $$$\mathrm{2.7 \times 2.7 \times 8 \, mm^3}$$$ compared to $$$\mathrm{3.5 \times 3.5 \times 10 \, mm^3}$$$ in6, and a shorter TE (74 ms vs. 118 ms in6). The gradient non-uniformity and table vibrations are more severe in the Connectom scanner compared to conventional clinical scanners which may affect the estimated parameters.
Future work will expand the investigations to patients with heart disease.
Acknowledgements
We thank Siemens Healthcare for the pulse sequence development environment. This work was supported by Wellcome Trust Investigator Award (219536/Z/19/Z), EPSRC (EP/M029778/1), The Wolfson Foundation, and the British Heart Foundation (PG/19/1/34076).References
1. Basser PJ, Mattiello J, LeBihan D. MR diffusion tensor spectroscopy and imaging. Biophysical journal. 1994;66(1):259-67.
2. Jensen JH, Helpern JA, Ramani A, Lu H, Kaczynski K. Diffusional kurtosis imaging: the quantification of non-gaussian water diffusion by means of magnetic resonance imaging. Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2005;53(6):1432-40.
3. Szczepankiewicz F, van Westen D, Englund E, Westin CF, Ståhlberg F, Lätt J, et al.The link between diffusion MRI and tumor heterogeneity: Mapping cell eccentricity and density by diffusional variance decomposition (DIVIDE). Neuroimage.2016;142:522-32.
4. Szczepankiewicz F, Lasič S, van Westen D, Sundgren PC, Englund E, Westin CF, et al. Quantification of microscopic diffusion anisotropy disentangles effects of orientation dispersion from microstructure: applications in healthy volunteers and in brain tumors. Neuroimage. 2015;104:241-52.
5. Henriques RN, Jespersen SN, Shemesh N. Microscopic anisotropy misestimation in spherical-mean single diffusion encoding MRI. Magnetic resonance in medicine. 2019;81(5):3245-61.
6. Teh I, Shelley D, Boyle JH, Zhou F, Poenar AM, Sharrack N, et al. Cardiac q-space trajectory imaging by motion-compensated tensor-valued diffusion encoding in human heart in vivo. Magnetic Resonance in Medicine. 2023;90(1):150-65.
7. Westin CF, Knutsson H, Pasternak O, Szczepankiewicz F, ̈Ozarslan E, van Westen D, et al. Q-space trajectory imaging for multidimensional diffusion MRI of the human brain. Neuroimage. 2016;135:345-62.
8. Lasič S, Szczepankiewicz F, Eriksson S, Nilsson M, Topgaard D. Microanisotropyimaging: quantification of microscopic diffusion anisotropy and orientational order parameter by diffusion MRI with magic-angle spinning of the q-vector. Frontiers in Physics. 2014;2:11.
9. Teh I, Shelley D, Poenar AM, Dall’Armellina E, Plein S, Schneider JE, et al. Tensor-valued Encoding in the Human Heart In vivo. In: Proceedings of the 31st Annual Meeting of ISMRM, London, UK; 2022. p. 17.
10. Teh I, Lasič S, Lundell H, Wereszczynska B, Budde M, Dall’Armellina E, et al.Multidimensional diffusion MRI in the ex vivo mouse heart. In: Proceedings of the 30th Annual Meeting of ISMRM; 2021.
11. Teh I, Schneider JE, Whittington HJ, Dyrby TB, Lundell H. Temporal diffusion spectroscopy in the heart with oscillating gradients. In: Proc Intl Soc Mag ResonMed. vol. 3114; 2017.
12. Teh I, Lundell H, Whittington HJ, Dyrby TB, Schneider JE. Resolving microscopic fractional anisotropy in the heart. In: Proceedings of the 24th annual meeting of ISMRM, Singapore. vol. 800; 2016.
13. McClymont D, Teh I, Carruth E, Omens J, McCulloch A, Whittington HJ, et al. Evaluation of non-Gaussian diffusion in cardiac MRI. Magnetic resonance in medicine. 2017;78(3):1174-86.
14. Szczepankiewicz F, Sj ̈olund J, Ståhlberg F, Lätt J, Nilsson M. Tensor-valued diffusion encoding for diffusional variance decomposition (DIVIDE): Technical feasibility in clinical MRI systems. PLoS One. 2019;14(3):e0214238.
15. Sjölund J, Szczepankiewicz F, Nilsson M, Topgaard D, Westin CF, Knutsson H.Constrained optimization of gradient waveforms for generalized diffusion encoding. Journal of Magnetic Resonance. 2015;261:157-68.
16. Szczepankiewicz F, Westin CF, Nilsson M. Maxwell-compensated design of asymmetric gradient waveforms for tensor-valued diffusion encoding. Magnetic resonance in medicine. 2019;82(4):1424-37.
17. Szczepankiewicz F, Sjölund J, Dall’Armellina E, Plein S, Schneider JE, Teh I,et al. Motion-compensated gradient waveforms for tensor-valued diffusion en-coding by constrained numerical optimization. Magnetic resonance in medicine. 2021;85(4):2117-26.
18. Eichner C, Cauley SF, Cohen-Adad J, Möller HE, Turner R, Setsompop K, et al. Real diffusion-weighted MRI enabling true signal averaging and increased diffusion contrast. NeuroImage. 2015;122:373-84.
19. Marstal K, Berendsen F, Staring M, Klein S. SimpleElastix: A user-friendly, multi-lingual library for medical image registration. In: Proceedings of the IEEE conference on computer vision and pattern recognition workshops; 2016. p. 134-42.
20. Coveney C, Kelly C, Teh I, Afzali M, Mueller L, Das A, et al. Semi-automated rejection of corrupted images in cardiac diffusion tensor imaging. Proceedings of the Annual Meeting of ISMRM. 2023.
21. Nilsson M, Szczepankiewicz F, Lampinen B, Ahlgren A, de Almeida Martins JP, Lasič S, et al. An open-source framework for analysis of multidimensional diffusion MRI data implemented in MATLAB. In: Proc Intl Soc Mag Reson Med. vol. 26;2018. p. 5355.
Figures