1263
MULti-TImepoint VElocity-selective Reconciled with Spatially-sElective (MULTIVERSE) ASL: Pushing the Limit of Arterial Transit Time1The Russell H. Morgan Department of Radiology and Radiological Science, Johns Hopkins University, Baltimore, MD, United States, 2F.M. Kirby Research Center for Functional Brain Imaging, Kennedy Krieger Institute, Baltimore, MD, United States, 3Department of Neurology, Johns Hopkins University, Baltimore, MD, United States, 4Department of Biostatistics, Johns Hopkins University, Baltimore, MD, United States
Synopsis
Keywords: Arterial Spin Labelling, Perfusion, Cerebral blood flow, arterial transit time, multi time point, arterial spin labeling
Motivation: Existing multi-timepoint arterial spin labeling (ASL) methods can only estimate cerebral blood flow (CBF) and arterial transit time (ATT) with a limited range of ATT (<2000ms).
Goal(s): Improve quantification of CBF and ATT for a wide range of ATT.
Approach: MULTIVERSE ASL applies combined fitting of multi-PLD pseudo-continuous (PC) ASL and multi-PLD velocity-selective (VS) ASL to measure CBF and ATT.
Results: With the same scan time, MULTIVERSE ASL improved the accuracy and precision and reduced uncertainty in CBF and ATT quantification across an extended range of ATT (500-4000ms).
Impact: This novel and straightforward approach improves perfusion measurement over the extended range of arterial transit time which was not possible with existing ASL methods. It highlights the clinical potential of ASL-based perfusion mapping in various altered physiological and pathological conditions.
Introduction
It is desirable for arterial spin labeling (ASL) to quantify both cerebral blood flow (CBF) and arterial transit time (ATT) among various clinical populations. Pseudo-continuous ASL (PCASL) underestimates CBF when ATT is longer than the recommended post-labeling delay (PLD) of 2000ms1. Multi-timepoint PCASL methods were largely optimized for ATT<1800ms2. While velocity-selective ASL (VSASL) mitigates the susceptibility to prolonged ATT, it was recently shown to underestimate CBF when trailing-edge-ATT is shorter than the applied PLD3,4. A new technique termed (VESPA) was developed that added PC labeling during the PLD after the VS labeling in one sequence to allow improved CBF and ATT estimation for ATT<1800ms5. Here we propose a novel and straightforward approach, dubbed MULti-TImepoint VElocity-selective Reconciled with Spatially-sElective or “MULTIVERSE” ASL, through combined fitting of multi-PLD PCASL and VSASL to compensate for their respective ATT sensitivity and measure CBF and ATT for a wide range of ATT (500-4000ms).Methods
Similar to VESPA ASL method5, the key concept of MULTIVERSE ASL is also to establish the ATT from the trailing edge of the VSASL bolus equal to the ATT of the leading edge of the PCASL bolus. Instead of using a modified spatially selective VS module as in VESPA ASL5, MULTIVERSE ASL inserts several inferior saturation pulses (ISP) following the VS module to crush the inflow of blood below the labeling plane of PCASL.Monte Carlo simulation was performed using PLD of 500ms, 1000ms, 1500ms, 2000ms, and 2500ms. The noise was added to match the SNR efficiency for multi-PLD ASL and the combined method. Bias was defined by the difference between the mean of estimates and the ground truth and then normalized by the ground truth. Precision was defined by the coefficients of variation (CoV) of estimates.
Experiments were conducted on a 3T Philips scanner using a 32-channel head-only receive coil with 7 healthy volunteers (5F, 27-68yo) enrolled. PCASL used a labeling duration of 1800ms. VS inversion-based VSASL6,7 used a cut-off velocity of 2.0cm/s. 3D GRASE acquisition covered the whole brain with FOV: 220x220x120mm3, voxel size: 3.4x3.4x5.0mm3. PCASL and VSASL were acquired with 5 PLDs described above with 4 repeats and 13min scan duration respectively.
CBF and ATT were fitted using the general kinetic models8 with the least square method. The fitting uncertainty was assessed by the 95% Confidence interval (CI) of the fitted CBF and ATT, and the normalized standard error (nSE=SE/fitted value). Using CBF and ATT fitted from MULTIVERSE ASL with a total of 26min data as the ground truth, the 6.5min multi-PLD PCASL, VSASL, and MULTIVERSE ASL were compared with voxel-wise bias, standard deviation (SD) of the bias, and root mean square error (RMSE).
Results and Discussion
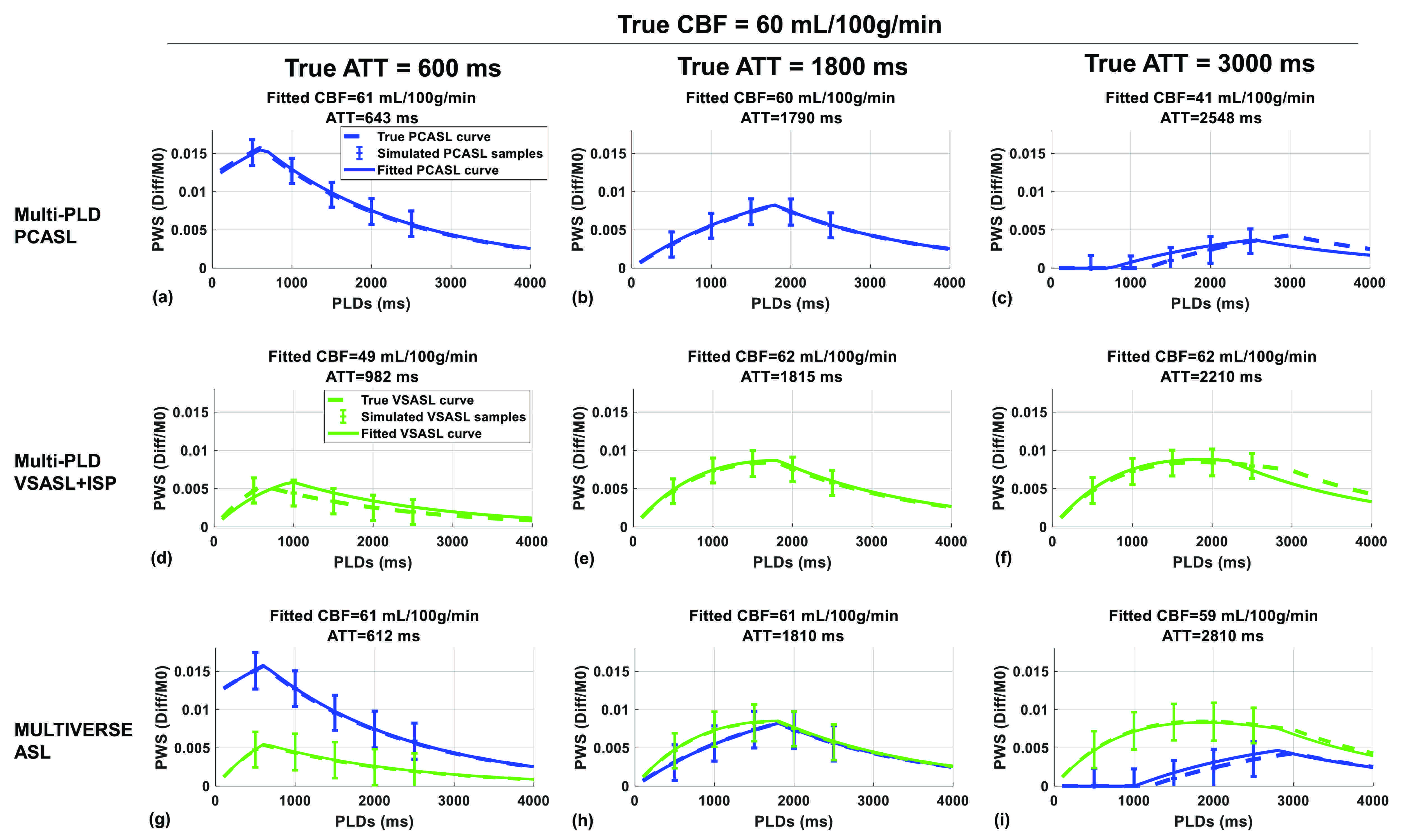
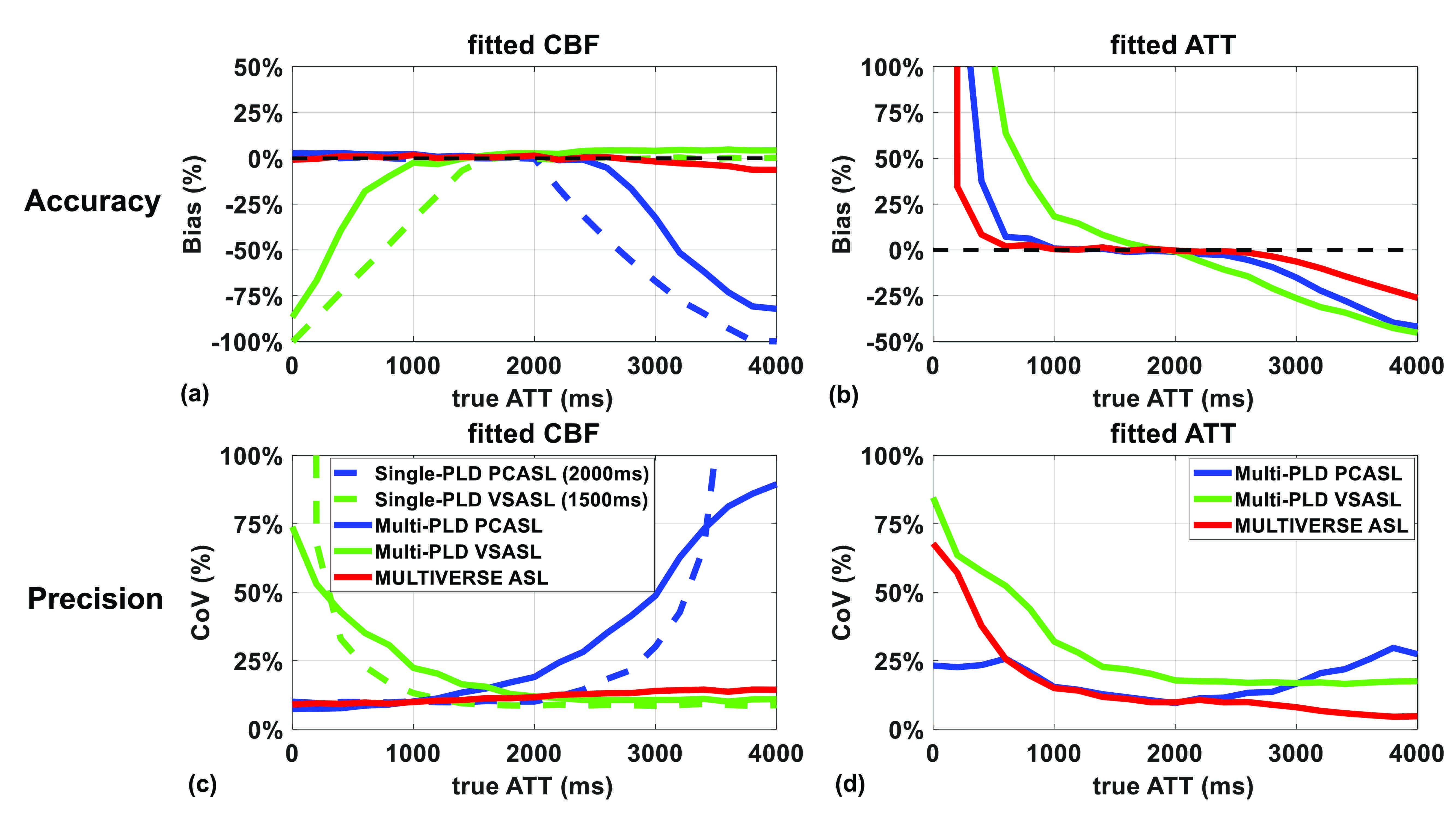
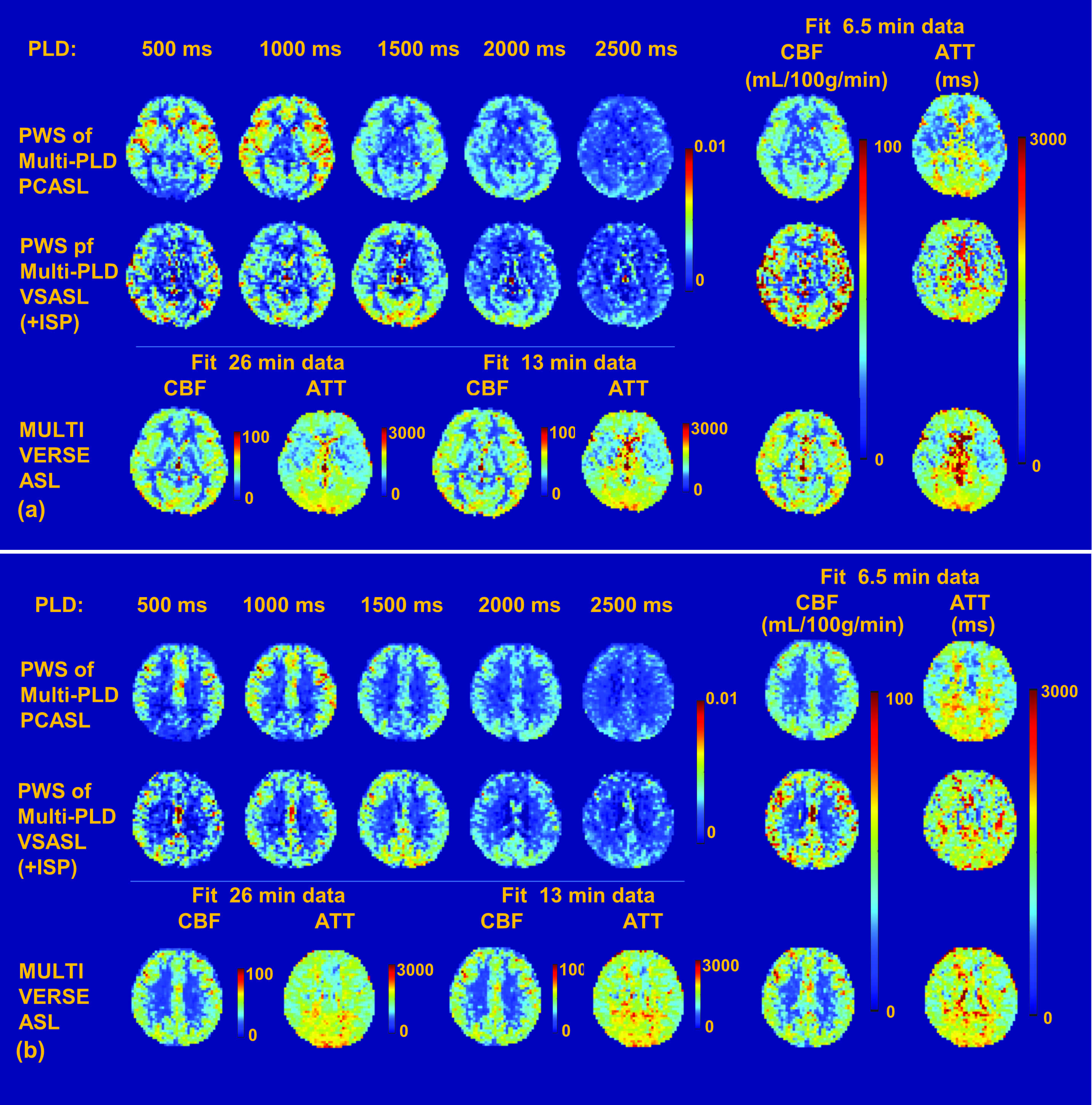
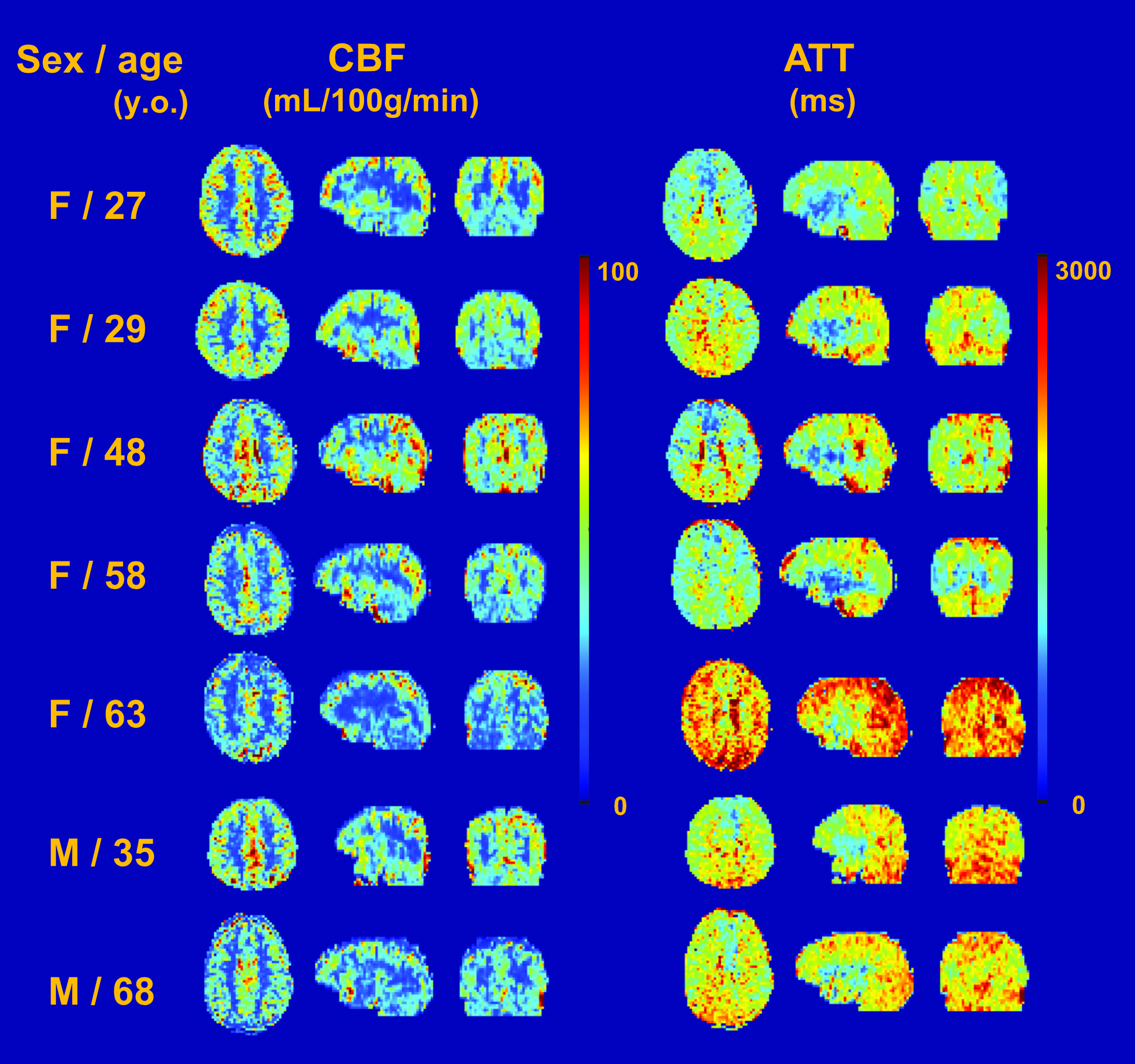
Fig.1 provides fitting examples of multi-PLD PCASL, multi-PLD VSASL, and MULTIVERSE ASL with true ATT=600ms, 1800ms, and 3000ms, respectively. Fig.2 shows the comparison of the three methods from Monte Carlo simulations. Across a wide range of ATT (500-4000ms), MULTIVERSE ASL outperformed in the accuracy and precision of CBF fitting than multi-PLD PCASL or multi-PLD VSASL (Fig.2a, c). MULTIVERSE provided better accuracy in estimating ATT overall and better precision in moderate and long ATT than multi-PLD PCASL and VSASL (Fig.2b, d).Fig.3 shows that multi-PLD PCASL provided a higher perfusion signal at regions with shorter ATT (e.g. frontal lobe) while VSASL provided a higher perfusion signal at regions with longer ATT (e.g. posterior lobe). Fig.3 also shows comparable CBF and ATT maps resulting from 6.5min multi-PLD PCASL, VSASL, and MULTIVERSE ASL, respectively, which are slightly noisier than the MULTIVERSE ASL results using the entire 26min of data. Fig.4 illustrates CBF and ATT maps from all 7 subjects given by MULTVERSE ASL with 6.5min of data, showing normal variations of gender and age7.
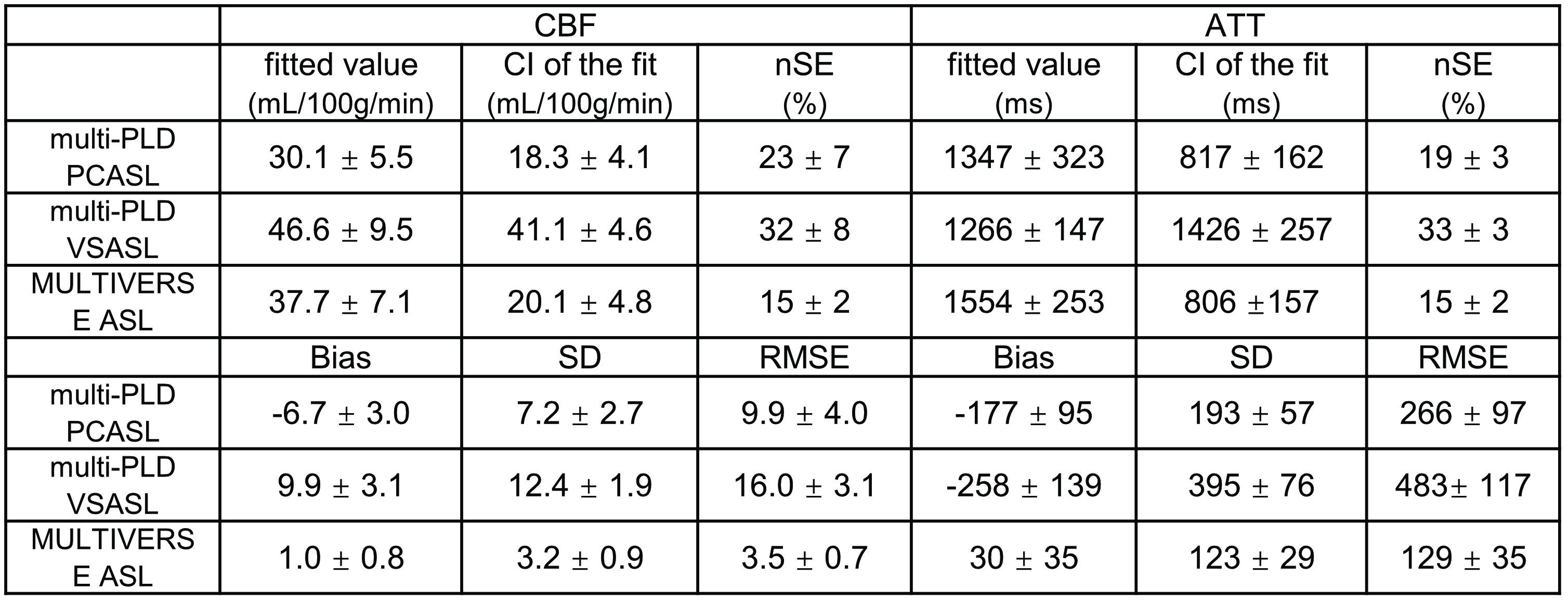
Table 1 shows that CI of CBF and ATT were narrower in MULTIVERSE ASL and multi-PLD PCASL compared to multi-PLD VSASL, and nSE was significantly shorter in MULTIVERSE ASL than in either PCASL (P=0.007/0.01 for CBF/ATT) or VSASL (P=0.0008/P<0.0001), indicating a more reliable fitting in MULTIVERSE ASL. When using the 26min MULTIVERSE ASL as ground truth, 6.5min MULTIVERSE ASL demonstrated less bias than PCASL (P=0.0003/0.002 for CBF/ATT) or VSASL (P=0.0002/0.001); less SD of bias than PCASL (P=0.002/0.004) or VSASL (P<0.0001/P<0.0001); less RMSE than PCASL (P=0.002/0.004) or VSASL (P<0.0001/P=0.0001).
Conclusion
Compared to multi-PLD PCASL or VSASL alone, the combined fitting of MULTIVERSE ASL improved the accuracy and precision and reduced uncertainty in CBF and ATT quantification across an extended range of ATT, which was not possible with existing ASL methods. This novel method highlights the clinical potential of ASL in various altered physiological and pathological conditions.Acknowledgements
No acknowledgement found.References
1 Alsop DC, Detre JA, Golay X, Günther M, Hendrikse J, Hernandez-Garcia L et al. Recommended implementation of arterial spin-labeled perfusion MRI for clinical applications: A consensus of the ISMRM perfusion study group and the European consortium for ASL in dementia. Magn Reson Med 2015; 73: 102–116.
2 Woods JG, Chappell MA, Okell TW. A general framework for optimizing arterial spin labeling MRI experiments. Magnetic Resonance in Medicine 2019; 81: 2474–2488.
3 Xu F, Xu C, Liu D, Zhu D, Lu H, Qin Q. Comparison of Velocity Selective ASL and PCASL with Phase-Contrast MRI for Measuring CO2-induced Cerebrovascular Reactivity. In: Proceedings of the 31th annual meeting of ISMRM. London, England, UK, 2022, p 4907.
4 Ian D. Driver, Chandler HL, Patitucci E, Wise RG, Germuska M. Velocity-selective arterial spin labelling bolus duration measurements: Implications for consensus recommendations. In: Proceedings of the 32th annual meeting of ISMRM. Toronto, ON, Canada, 2023, p 0375.
5 Woods JG, Wong EC, Boyd EC, Bolar DS. VESPA ASL: VElocity and SPAtially Selective Arterial Spin Labeling. Magnetic Resonance in Medicine 2022; 87: 2667–2684.
6 Qin Q, van Zijl PCM. Velocity-selective-inversion prepared arterial spin labeling. Magn Reson Med 2016; 76: 1136–1148.
7 Xu F, Liu D, Zhu D, Hillis AE, Bakker A, Soldan A et al. Test-retest reliability of 3D velocity-selective arterial spin labeling for detecting normal variations of cerebral blood flow. Neuroimage 2023; 271: 120039.
8 Buxton RB, Frank LR, Wong EC, Siewert B, Warach S, Edelman RR. A general kinetic model for quantitative perfusion imaging with arterial spin labeling. Magn Reson Med 1998; 40: 383–396.
Figures