1258
Time-Resolved pCASL MRA Using A Multi-Echo 3D-Radial SPGR Sequence1Department of Diagnostic Imaging, Monash Health, Melbourne, Australia, 2Department of Radiology, Monash University, Melbourne, Australia, 3Nuffield Department of Clinical Neurosciences, University of Oxford, Oxford, United Kingdom
Synopsis
Keywords: Arterial Spin Labelling, Arterial spin labelling
Motivation: To improve signal, spatial and temporal resolution, and acquisition time for time resolved ASL imaging for cerebral angiography.
Goal(s): To exploit a time-resolved multi-echo radial 3D ASL sequence to acquire ASL MRA data in a shorter amount of time.
Approach: We performed three flip angle optimized scans with a 1, 2, and 3 echo readout, respectively, and compared image quality and acquisition time.
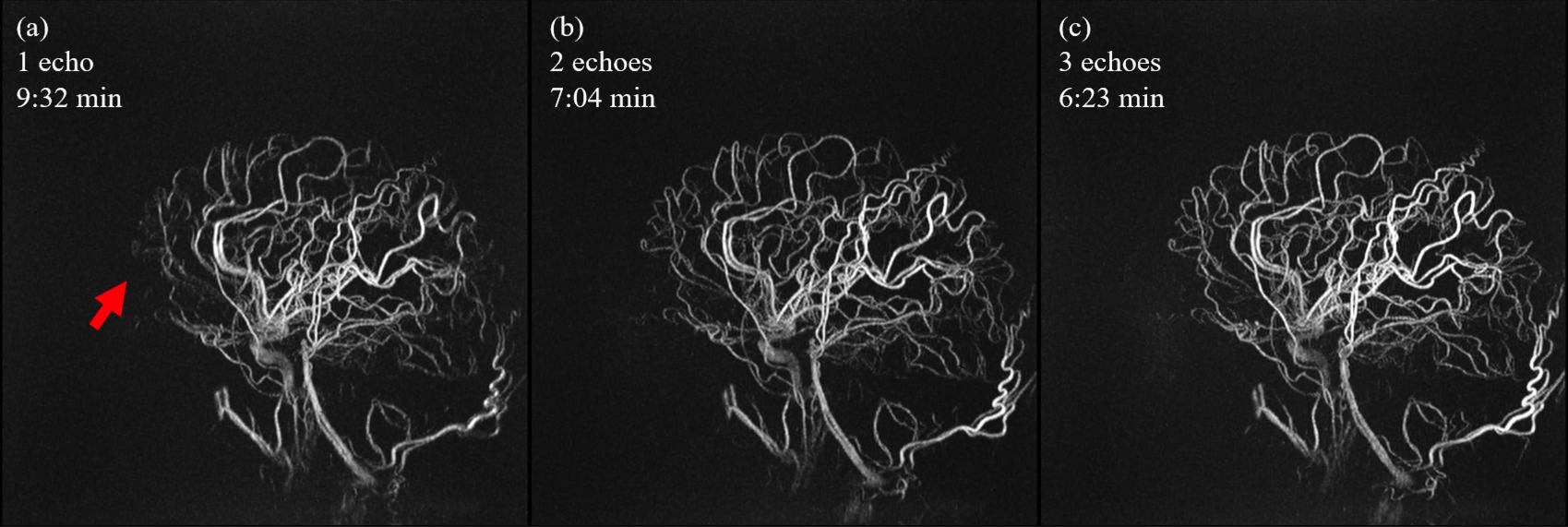
Results: Using a 3-echo readout, scan time could be reduced from 9:32 min to 6:23 min, without the loss of image quality. Multi-echo scans even showed more details than in the single-echo case.
Impact: Multi-echo 3D radial ASL angiography enables substantial scan time reduction for high-resolution time-resolved cerebral angiography. This will improve clinical applicability and scanner throughput, avoid the use of contrast agents, and is of direct benefit to patients.
Introduction
Arterial spin labeling (ASL)-based MRA exhibits several key advantages over contrast-enhanced (CE), phase-contrast (PC), and TOF MRA. Relative to TOF, ASL MRA permits a high-resolution time-resolved angiographic acquisition of the inflowing ASL bolus. This feature is especially beneficial for the diagnostic work-up of chronic steno-occlusive cerebrovascular diseases and high-flow shunting lesions [1], [2]. As the angiographic acquisition does not need to be timed around a short exogenous contrast bolus, ASL MRA outperforms CE-MRA both in terms of spatial and temporal resolution. ASL MRAs are not cluttered by signal from normal draining veins as the label diffuses into tissue where it decays with tissue T1. This improves conspicuity of AV-shunts.Published works on time-resolved ASL-angiography differ in their strategies for labeling and readout, as well as how temporal resolution is achieved [3]–[6]. In general, such a sequence consists of several alternating label and control blocks; each one followed by a readout module. Total scan duration has been a shortcoming of ASL-based angiographic methods.
To address current shortcomings of time-resolved 3D ASL-MRA, we combined a pCASL module with a 3D-radial multi-echo readout and variable flip-angle readout scheme. This approach achieves radically faster data acquisition as well as high spatial and temporal resolution.
Methods
Sequence:A pCASL module with duration of 2 seconds was employed for labeling. After a hard-pulse excitation, data was acquired with a multi-echo 3D radial SPGR sequence. To acquire several radial encodings, phase encoding blips were used between echo acquisitions. Data was sampled during the pre-phaser (half echoes) and readout gradients (full echoes) with ramp sampling. The total readout length after labeling was fixed to 1 second. To achieve a time-resolved acquisition, it was further subdivided into 5 phases, resulting in a temporal footprint of 200ms.
The signal difference between label and control image continuously decreases because of T1 relaxation, as well as the repeated application of RF pulses. To guarantee stable signal intensity, a variable flip angle scheme was used. The angles were computed numerically for each experiment.
$$\alpha_n = \arccos \sqrt{ 1 + \frac{E_1^2-1}{E_1^{2(n-N)}-E_1^2}}$$
Here, N denotes the total number of excitations per shot, $$$\alpha_n$$$ is the current excitation angle, and E1 denotes the T1 relaxation term exp(-TR/T1). T1 of arterial blood at 3T was assumed to be 1600ms.
Experiments:
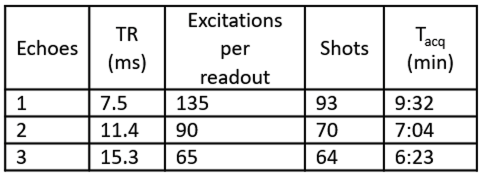
To assess the effect of multi-echo readouts, measurements with one, two, and three echoes were carried out. To accommodate the additional readouts, TR was increased from 7.5ms to 11.4ms, and 15.3ms. For all scans, the total number of spokes was kept approximately constant (~12500). Table 1 lists the variable sequence parameters and scan time reduction for multi-echo readouts.
Data were acquired with FOV=220mm, 0.68mm isotropic resolution and BW=280Hz/Pixel.
For image reconstruction, a gridding algorithm was used. All acquired half and full echoes where reconstructed separately, and subsequently summed up. This step is necessary to avoid phase cancelation of different echoes due to B0 inhomogeneity.
Results
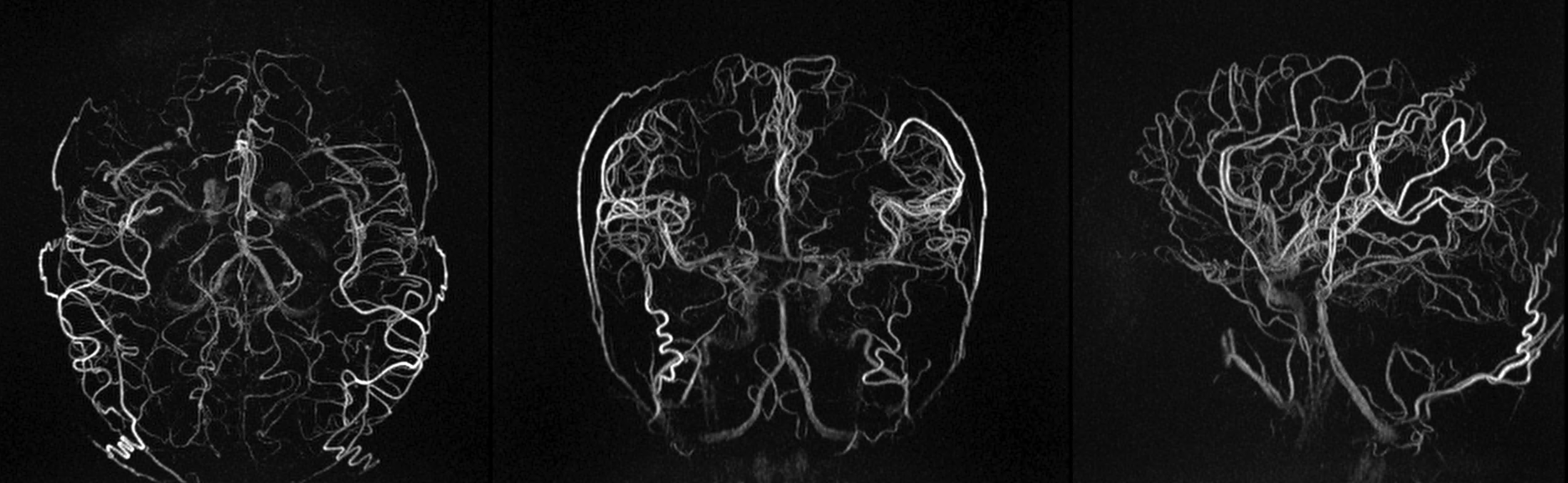
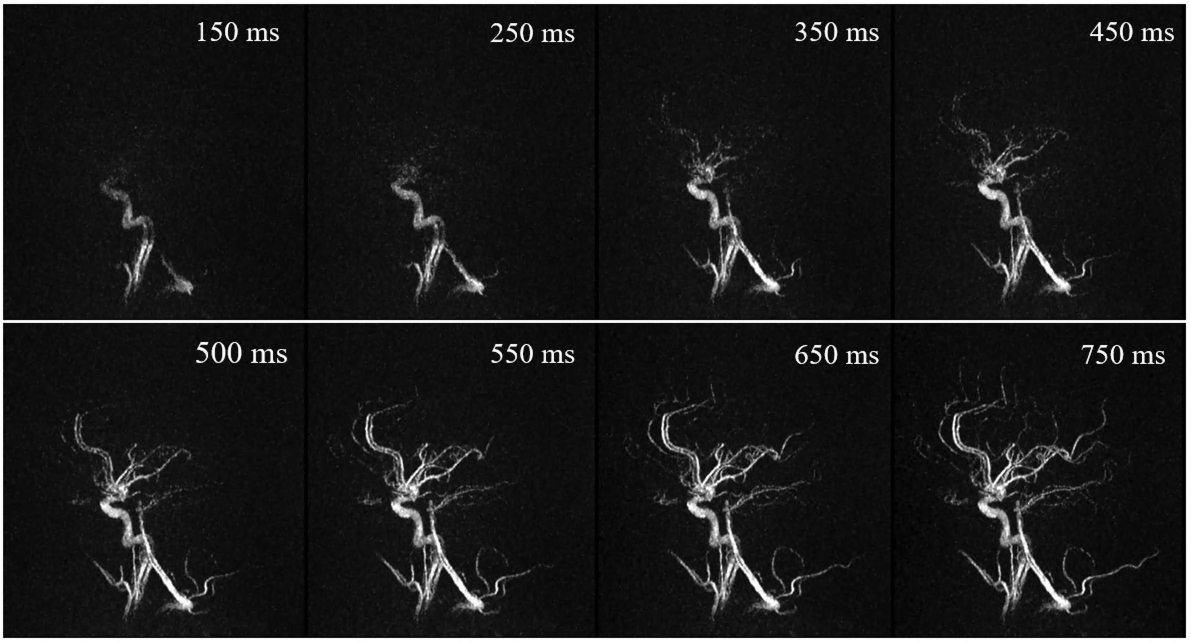
Fig 1. shows a comparison of the combined reconstruction of all phases for the acquisitions with varying echo number. All images exhibit excellent image quality. Signal intensity visually appears strong and similar for all experiments, whereas for the single-echo acquisition fewer details are visible. In Fig. 2. MIPs in three orientations illustrate the isotropic nature of the sequence. Fig. 3 displays a sliding window reconstruction of several phases with temporal resolution of 100ms. Inflow subtraction [4] was performed to depict the inflow of blood into the vasculature.Discussion
We described a time-resolved 3D-radial pCASL ASL angiography sequence with isotropic resolution of 0.68 mm. Using a sliding window reconstruction high temporal resolution can be achieved. Multi-echo acquisition allows for scan time reduction from 9:32 min to 6:23 min without loss of image quality. Further, optimized flip angles stabilize echo intensities over time. The increased TR of multi-echo acquisitions enables the use of higher flip angles. However, this comes at the cost of increased B0 dephasing and T2* decay. By using magnitude echo summation, signal cancellation due to off-resonance phase shifts can be avoided in the gridding process.Acknowledgements
No acknowledgement found.References
[1] S. A. Amukotuwa, M. P. Marks, G. Zaharchuk, F. Calamante, R. Bammer, and N. Fischbein, “Arterial Spin-Labeling Improves Detection of Intracranial Dural Arteriovenous Fistulas with MRI,” Am. J. Neuroradiol., vol. 39, no. 4, pp. 669–677, Apr. 2018, doi: 10.3174/ajnr.A5570.
[2] T. T. Le, N. J. Fischbein, J. B. André, C. Wijman, J. Rosenberg, and G. Zaharchuk, “Identification of Venous Signal on Arterial Spin Labeling Improves Diagnosis of Dural Arteriovenous Fistulas and Small Arteriovenous Malformations,” Am. J. Neuroradiol., vol. 33, no. 1, pp. 61–68, Jan. 2012, doi: 10.3174/ajnr.A2761.
[3] T. W. Okell and M. Chiew, “Optimization of 4D combined angiography and perfusion using radial imaging and arterial spin labeling,” Magn. Reson. Med., vol. 89, no. 5, pp. 1853–1870, 2023, doi: 10.1002/mrm.29558.
[4] D. Kopeinigg and R. Bammer, “Time-Resolved Angiography using InfLow Subtraction (TRAILS),” Magn. Reson. Med., vol. 72, no. 3, pp. 669–678, 2014, doi: 10.1002/mrm.24985.
[5] H. Wu et al., “Non-contrast Dynamic 3D Intracranial MR Angiography using Pseudo-Continuous Arterial Spin Labeling (PCASL) and Accelerated 3D Radial Acquisition,” J. Magn. Reson. Imaging JMRI, vol. 39, no. 5, pp. 1320–1326, May 2014, doi: 10.1002/jmri.24279.
[6] Y. Suzuki et al., “Acceleration of ASL-based time-resolved MR angiography by acquisition of control and labeled images in the same shot (ACTRESS),” Magn. Reson. Med., vol. 79, no. 1, pp. 224–233, 2018, doi: 10.1002/mrm.26667.
Figures