1257
Double Inversion Recovery in myocardial Arterial Spin Labeling (ASL) for reduced physiological noise1Computer Assisted Clinical Medicine, Medical Faculty Mannheim, Heidelberg University, Heidelberg, Germany, 2Mannheim Institute for Intelligent Systems in Medicine, Medical Faculty Mannheim, Heidelberg University, Mannheim, Germany, 3Department of Imaging Physics, Delft University of Technology, Delft, Netherlands, 4Centre de Resonance Magnetique Biologique et Medicale, Aix-Marseille Universite, Marseille, France
Synopsis
Keywords: Arterial Spin Labelling, Arterial spin labelling, Myocardial perfusion
Motivation: Myocardial Arterial Spin Labeling (myoASL) presents a promising contrast-agent-free approach for assessing myocardial blood flow (MBF), but its clinical translation is hampered by high levels of physiological noise (PN).
Goal(s): We introduce double inversion recovery (DIR) preparations for FAIR-myoASL to mitigate sensitivity to heart rate variations and reduce PN.
Approach: A flip-back inversion pulse was added immediately after the FAIR-labeling, to allow for near-complete recovery and, thus, for more effective cancellation of the myocardial background signal in the presence of heart rate variations.
Results: Using DIR preparations in vivo, led to a PN reduction of up to 66 % compared to conventional myoASL.
Impact: FAIR-myoASL with double inversion recovery (DIR) labeling can compensate for fluctuating myocardial background signals due to heart rate variability. In vivo, experiments suggest that DIR-preparations substantially reduce PN, thus, improving overall robustness and potentially facilitating broader clinical translation of myoASL.
Introduction
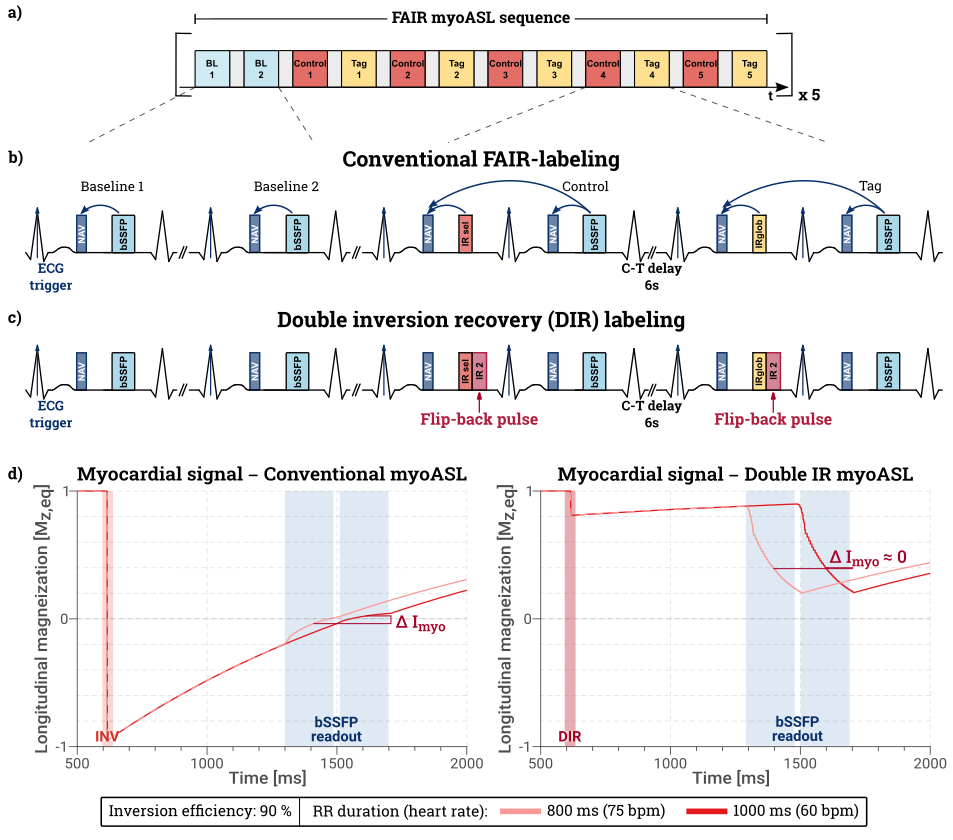
Myocardial Arterial Spin Labeling (myoASL) can provide a contrast-agent-free alternative to first-pass perfusion MRI. While promising results have been achieved in quantifying myocardial blood flow (MBF) and assessing perfusion defects with myoASL1,2, clinical translation is still hampered due to the inherently low signal-to-noise ratio (SNR), primarily due to high levels of physiological noise (PN)1. In myoASL, perfusion is typically quantified by subtracting two inversion-prepared images with differing blood contrast, where the static myocardial tissue signal ideally cancels out. However, changes in the inversion time (TI) between the two images cause residual signal variation in the myocardium. Particularly for double ECG-gated myoASL3 this is a major source of PN, as the TI is determined by the specific RR-interval duration. It is thus directly affected by heart rate variability. In this work, we investigate the use of double inversion recovery (DIR) preparations to reduce the sensitivity of the myocardial signal to TI variations and improve precision in free-breathing, respiratory-navigated myoASL.FAIR-myoASL sequence
All imaging was performed at 3T (Skyra, Siemens) using a double ECG-gated Flow-Alternating Inversion Recovery (FAIR) myoASL sequence with bSFFP readout4,5. Dual respiratory gating was implemented, where control/tag images were only accepted when both consecutive pencil-beam navigators were within the acceptance window5. Additionally, a DIR FAIR-myoASL sequence was implemented, where the conventional inversion pulse was immediately followed by an identical inversion pulse with inverted pulse phase6. The flip-back ensures near-complete recovery of the stationary myocardial tissue during TI. Thus, even in the presence of TI changes, the myocardial signal effectively cancels out in the subtraction of control and tag image. In total, three FAIR-myoASL sequences were acquired: conventional myoASL with single FAIR-labeling, and two DIR-prepared myoASL sequences, using additional selective inversion pulses and additional non-selective pulses, respectively (Figure 1). Each sequence consisted of two baseline images and five/three (in vivo/phantom) control-tag pairs.Methods
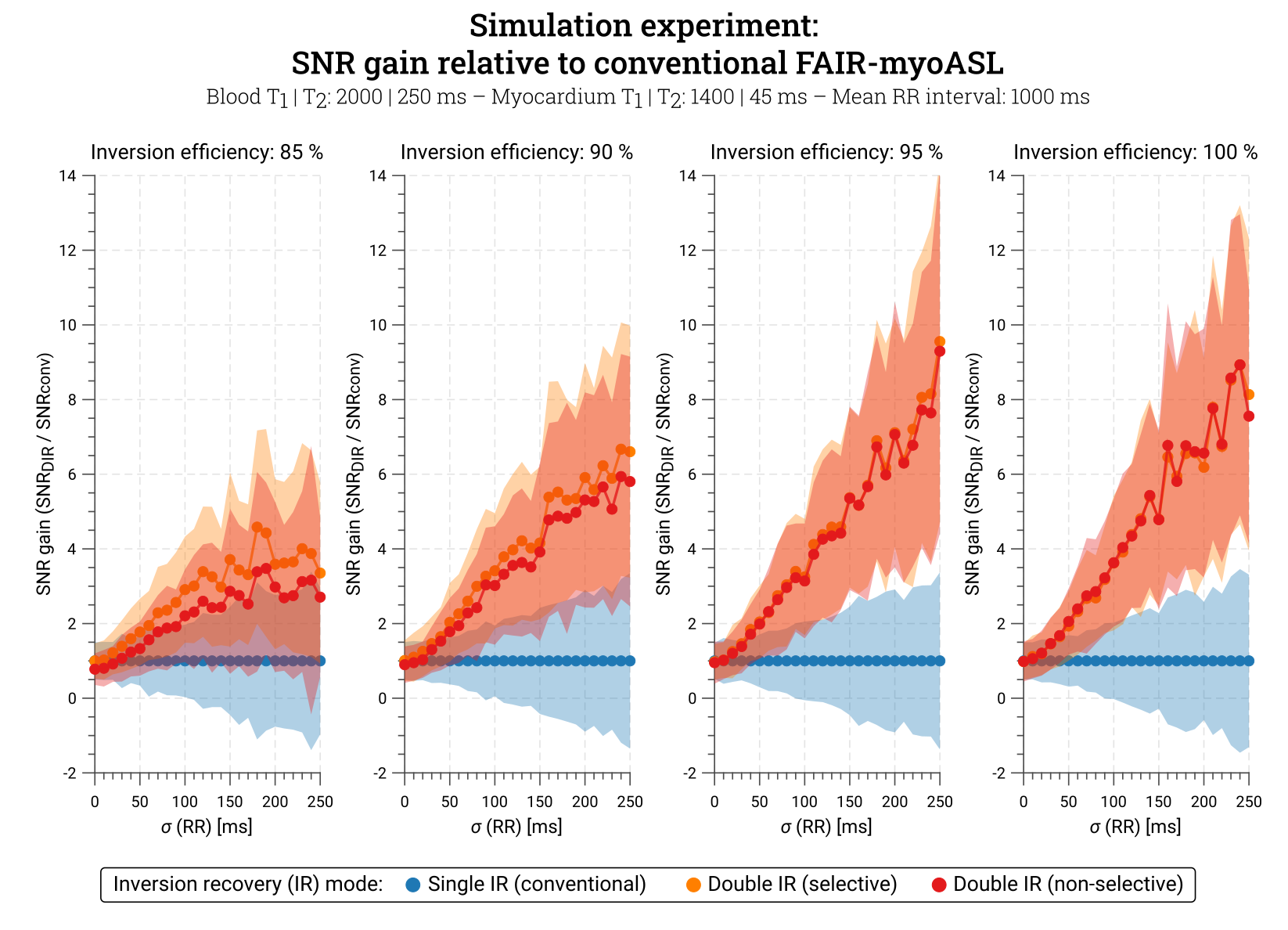
Bloch simulations were performed to assess the effect of added selective or non-selective inversion pulses on the myoASL-SNR. Physiological noise was simulated using varying RR durations (CoV: 0%-25%) and for a range of inversion efficiencies (85%-100%). All three sequences were acquired in a NiCl2-doped agarose phantom for a range of simulated HRs (50-100 bpm), as well as in two healthy volunteers (1 female, 1 male, 30.5±3.5 years). All images were acquired with 1.9x1.9x8mm3 voxel size, TE/TR 1.63/3.26 ms, FA 70°, GRAPPA 2, Partial Fourier (6/8), and with 5 repetitions. MOLLI8 was used for T1 mapping in phantom and in vivo. Data analysis involved group-wise registration9, followed by pixel- and segment-wise calculation of MBF using Buxton’s general kinetic model7 and individual blood T1 as previously described4.Results
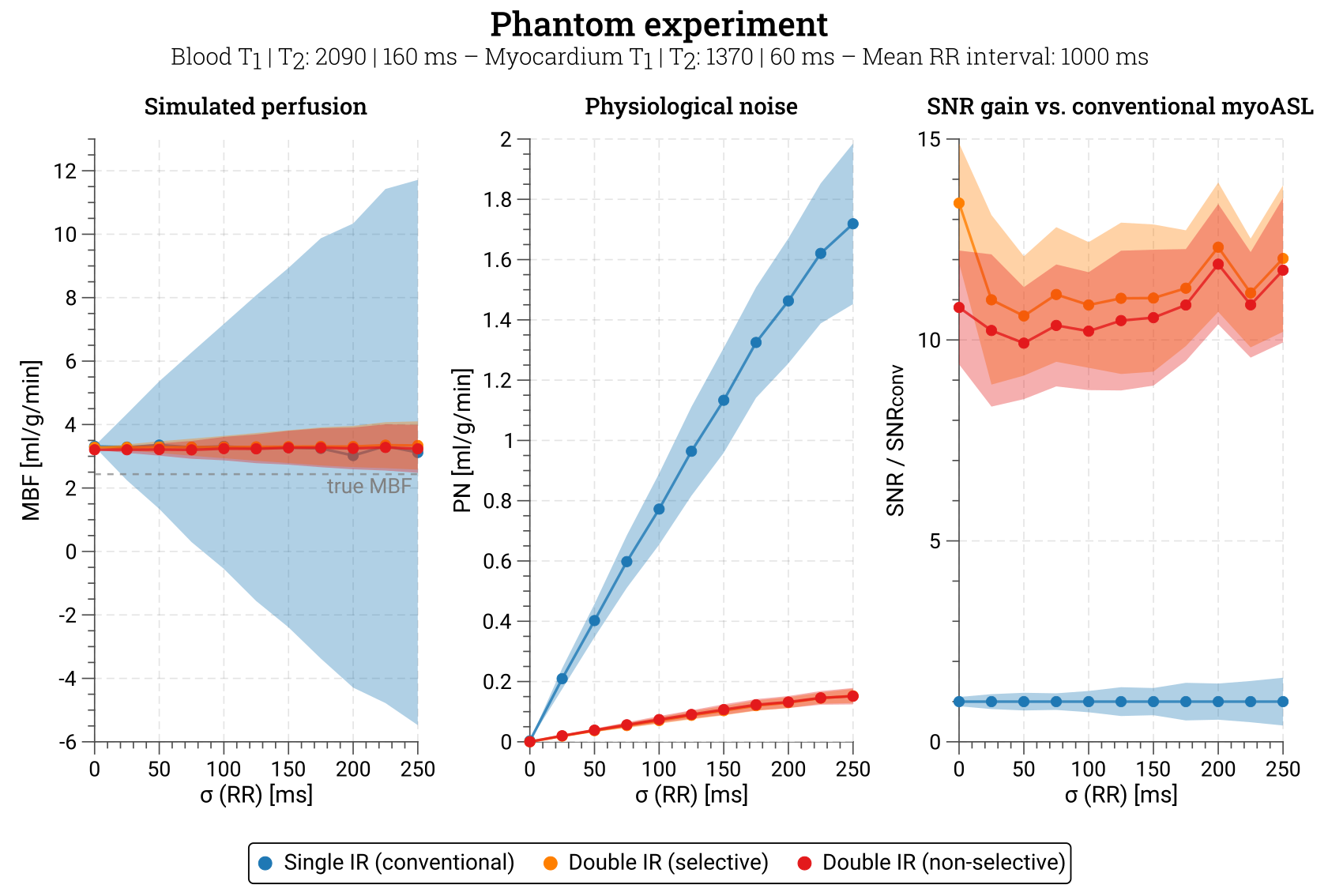
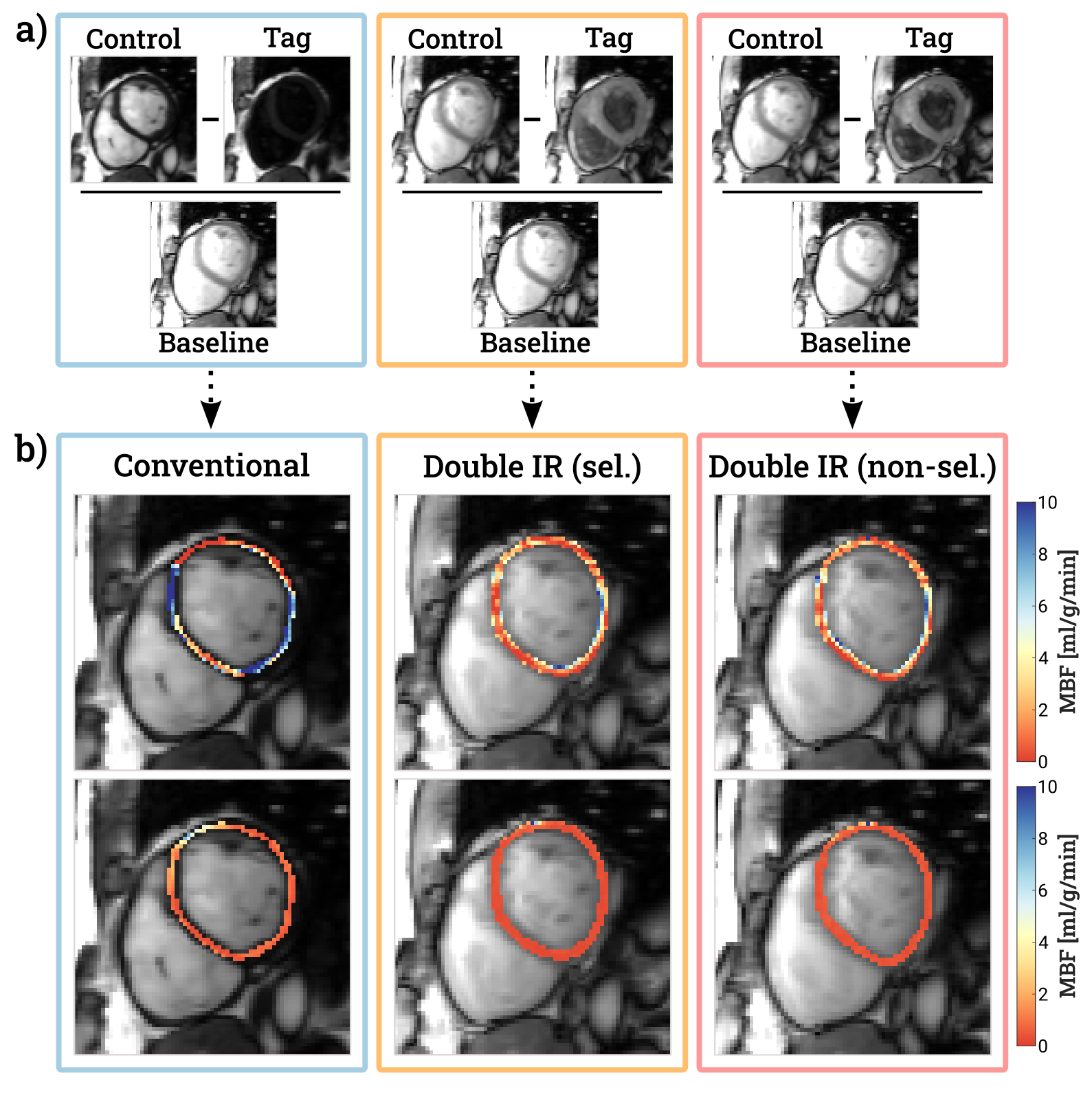
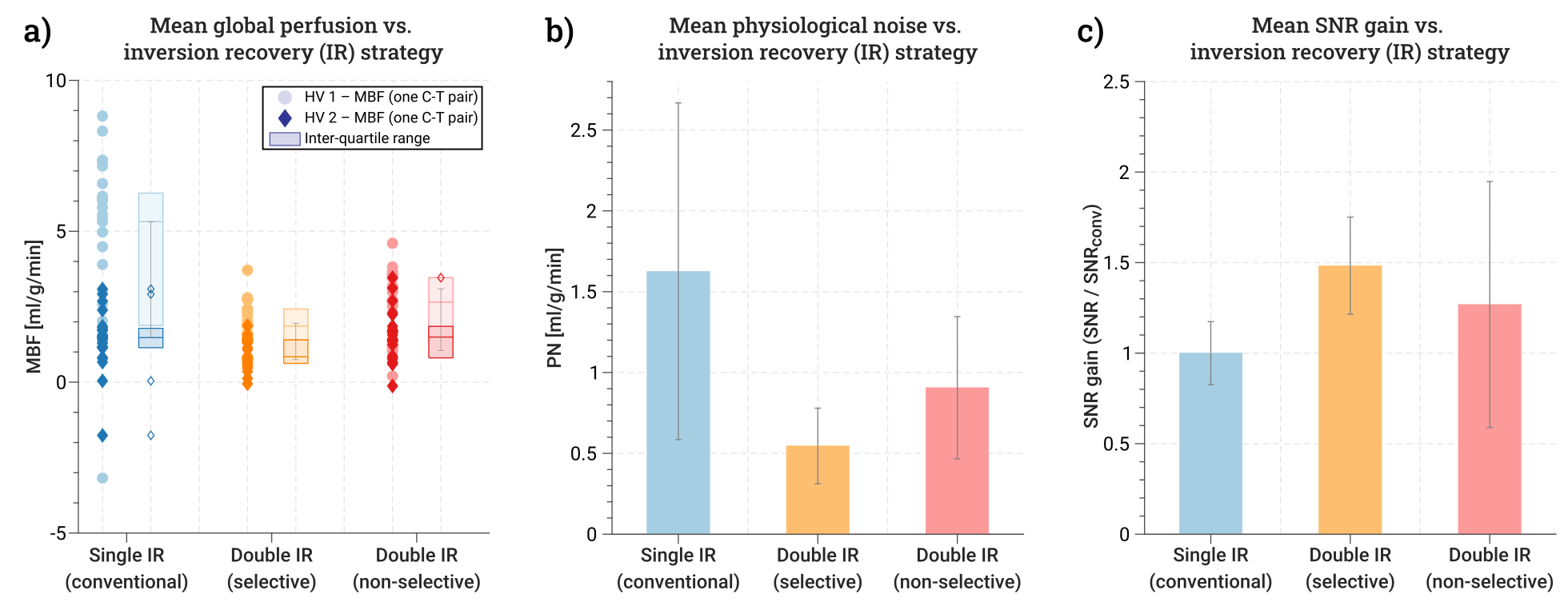
Simulated myoASL-SNR increased up to 9.5 times with DIR-labeling compared to conventional FAIR-labeling (Figure 2). The SNR gain was higher for higher inversion efficiencies and larger HR variations, i.e. higher ratios of PN relative to thermal noise. Phantom results showed that while MBF values remained nearly constant across all three sequences, PN was substantially reduced with DIR-prepared sequences, leading to an average SNR gain of 11.1±0.5 (Figure 3). In vivo, MBF maps showed improved quality and reduced PN levels when acquired with DIR-preparations (Figure 4). Using conventional FAIR-labeling, the in vivo mean MBF±PN was 2.47±1.06 ml/g/min and 1.09±0.44 ml/g/min for subjects 1 and 2, respectively (Figure 4 & 5). Selective DIR-preparations yielded a mean MBF±PN of 1.60±0.31 ml/g/min for subject 1 and 0.78±0.18 ml/g/min for subject 2. With additional non-selective inversion pulses, the corresponding values were 2.07±0.75 ml/g/min and 0.97±0.68 ml/g/min for subjects 1 and 2, respectively. The average PN across both subjects was reduced by 66±14% for selective and 44±27% for non-selective DIR-preparations, respectively (Figure 5).Discussion
In this work, we evaluated the use of DIR-labeling for reducing PN in free-breathing, respiratory-navigated FAIR-myoASL. Phantom as well as in vivo MBF were in agreement with previously published perfusion values obtained from myoASL1,4 and partly elevated compared to reported values from first-pass perfusion MRI10. In vivo, slightly lower MBF was observed for DIR-labeling, likely due to reduced non-zero-mean contributions to the PN. Our simulations and phantom experiments show that a flip-back pulse, added immediately after the FAIR-labeling, can compensate for inconsistent myocardial background signal due to HR-dependent changes in TI. Our in vivo data further suggests that DIR-preparations yield substantial reductions in PN and, in turn, an improved myoASL-SNR.Conclusion
Double inversion recovery prepared FAIR-myoASL offers a simple but promising approach to alleviate physiological noise and enable more precise and reliable perfusion quantification, potentially facilitating the broader clinical translation of myoASL.Acknowledgements
M.B.I. is funded by a PhD scholarship from the Landesgraduiertenförderung Baden-Württemberg, and a Procope Mobility stipend. S.W. acknowledges funding from the NWO (Start-up STU.019.024), and the European Union (ERC, VascularID, StG 101078711).References
- Zun, Z., Wong, E. C., & Nayak, K. S. (2009). Assessment of myocardial blood flow (MBF) in humans using arterial spin labeling (ASL): feasibility and noise analysis. Magn Reson Med, 62(4), 975-983.
- Zun, Z., Varadarajan, P., Pai, R. G., Wong, E. C., & Nayak, K. S. (2011). Arterial spin labeled CMR detects clinically relevant increase in myocardial blood flow with vasodilation. JACC: Cardiovascular Imaging, 4(12), 1253-1261.
- Do, H. P., Jao, T. R., & Nayak, K. S. (2014). Myocardial arterial spin labeling perfusion imaging with improved sensitivity. J Cardiovasc Magn Reson, 16, 1-6.
- Božić‐Iven, M., Rapacchi, S., Tao, Q., Pierce, I., Thornton, G., Nitsche, C., ... & Weingärtner, S. (2023). Improved reproducibility for myocardial ASL: Impact of physiological and acquisition parameters. Magn Reson Med.
- Božić-Iven, M., Rapacchi, S., Tao, Q., Schad, L. R., & Weingärtner, S. (2023). Respiratory navigated free-breathing myocardial arterial spin labeling (ASL) with phase sensitive reconstruction. Proc ISMRM.
- Henningsson, M., Malik, S., Botnar, R., Castellanos, D., Hussain, T., & Leiner, T. (2022). Black‐blood contrast in cardiovascular MRI. J Magn Reson Imaging, 55(1), 61-80.
- Buxton, R. B., Frank, L. R., Wong, E. C., Siewert, B., Warach, S., & Edelman, R. R. (1998). A general kinetic model for quantitative perfusion imaging with arterial spin labeling. Magn Reson Med, 40(3), 383-396.
- Messroghli, D. R., Radjenovic, A., Kozerke, S., Higgins, D. M., Sivananthan, M. U., & Ridgway, J. P. (2004). Modified Look‐Locker inversion recovery (MOLLI) for high‐resolution T1 mapping of the heart. Magn Reson Med, 52(1), 141-146.
- Tao, Q., van der Tol, P., Berendsen, F. F., Paiman, E. H., Lamb, H. J., & van der Geest, R. J. (2018). Robust motion correction for myocardial T1 and extracellular volume mapping by principle component analysis‐based groupwise image registration. J Magn Reson Imaging, 47(5), 1397-1405.
- Kellman, P., Hansen, M. S., Nielles-Vallespin, S., Nickander, J., Themudo, R., Ugander, M., & Xue, H. (2017). Myocardial perfusion cardiovascular magnetic resonance: optimized dual sequence and reconstruction for quantification. J Cardiovasc Magn Reson, 19(1), 1-14.
Figures