1249
Banding insensitive DESPO for T1 and T2 mapping applied to 3D prostate at 3T.1Pontificia Universidad Catolica de Chile, Santiago, Chile, 2Millenium Institute for Intelligent Healthcare Engineering, Santiago, Chile, 3Institute for Biological and Medical Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile, 4School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 5Department of Radiology, School of Medicine, Pontificia Universidad Católica de Chile, Santiago, Chile, 6Institute for Biological and Medical Engineering, Santiago, Chile
Synopsis
Keywords: Artifacts, Prostate, Banding artifacts, bSSFP mapping
Motivation: DESPO is a robust T2 brain mapping technique based on balanced steady-state free precession (bSSFP). However, it is susceptible to off-resonance artifacts, especially in areas with high susceptibility changes, such as the prostate.
Goal(s): Our proposed method, DESPO+, integrates the complete bSSFP and spoiled-gradient echo (SPGR) models, using a simulation-based approach for 3D T1/T2 maps in the prostate region.
Approach: We employed a simulated-based method of the full bSSFP and SPGR models incluiding off-resonance to reconstruct T1/T2/PD simultaneously.
Results: DESPO+ provides off-resonance insensitive with high-resolution 3D T1/T2 mapping, synthesizing T1-weighted/T2-weighted images using a short scan time of 3.6 minutes, similar to DESPO.
Impact: DESPO+ provides an off-resonance insensitive and customizable solution, enabling high-resolution 3D T1/T2 mapping and synthesized T1-weighted/T2-weighted images for the entire prostate, all achieved within a short scan time of 3.6 minutes, similar to DESPO.m
Introduction
DESPO is a fast method for simultaneously 3D T1 and T2 mapping based on Spoiled gradient echo (SPGR) and balanced steady-state free precession1. The primary benefits of bSSFP are its high SNR and efficient scanning capabilities. However, the banding artifacts due to off-resonance can compromise the quality of the T2 maps2. The severity of the banding artifact increases with longer repetition times (TRs), prompting a preference for shorter TRs even at the expense of spatial resolution2. Despite the use of short TRs, certain regions with high magnetic susceptibility variations (sinuses, prostate, etc.) still generate artifacts. Our proposal, DESPO+, involves a simulation-based method that generates a lookup table using the complete signal models of bSSFP and SPGR sequences, including off-resonance. Subsequently, a matching process is performed between the measured and simulated signatures. DESPO+ is a DESPO insensitive to off-resonance. The suggested method was assessed through simulations, a 3D standardized T1/T2 phantom, and in-vivo acquisitions.Method
T1, T2 and Proton Density (PD) map reconstructions:- Simulation-based signals: each entry of the lookup table is done by the full signal equations for bSSFP:
where $$$M_{0}$$$ is the equilibrium magnetization, $$$a=-(1\ -\ E_1\ )\ \sin(\alpha)\ E_2 $$$, $$$b=(1\ -\ E_1\ )\sin(\alpha)$$$, $$$c=E_2\left(E_1\ -\ 1\right)(1\ +\ \cos{\left(\alpha\right)}) $$$, $$$ d=\left(1\ -{\ E}_1\cos{\left(\alpha\right)}\right)\ -\ \left(E_1\ -\ \cos{\left(\alpha\ \right)}\right){E_2}^2 $$$, $$$ E_{1,2}=e^{\frac{TR}{T_{1,2}}}$$$, $$$\phi = 2\pi TR \Delta f $$$, $$$\Delta f$$$ is the off-resonance. And, for SPGR:
$$ M_{s}(t) = M_{0} \frac{(1-E_{1})sin(\alpha)\overline{E}_{2}(t)}{1-E_{1}cos(\alpha)} $$
- Image acquisition: acquire P images using SPGR and Q images using bSSFP with variable TR, FA, and TE. Typically, P = 2 and Q = 3; thus there are five images. The signature (M) for each pixel is a vector with five values, one from each image.
- T1 and T2 maps: T1 and T2 values associated with the lookup table entry (k) with the highest inner product similarity between the measured (M) and simulated ($$$d_{k} $$$) signatures:
The lookup table was constructed using the following range values: T1(200-2500ms, every 10ms), T2(10-300ms, every 4ms), and $$$ \Delta f$$$ (-450-450Hz, every 4Hz).
- PD: it is determined by:
- Comparison method: we compared DESPO+ with DESPO1 using the Normalized Mean Squared Error (NRMSE) and Structural Similarity (SSIM) of T1/T2 values. Additionally, we synthesized T1 and T2 weighted images to compare them with acquired images for in-vivo.
- bSSFP and SPGR acquisitions: we tested in simulations, phantom and fourteen prostate volunteers. The acquisitions were done in a 3T Achieva MR system (Philips, Best, The Netherlands). Two 3D SPGR acquisitions with Flip Angles, α = 4º and 15º (TR/TE =9.0/3.46 ms) and three 3D bSSFP acquisitions with α (phase) = 15° (180°), 45° (180°) and 60° (180°), with TRs = 3.6, 4.8, and 6.2 ms. The FOV was 128x128 mm(simulations) and 160x160x108 mm(phantom and in-vivo acquisitions) with a resolution of 1x1x3 mm.
Results and Discussion
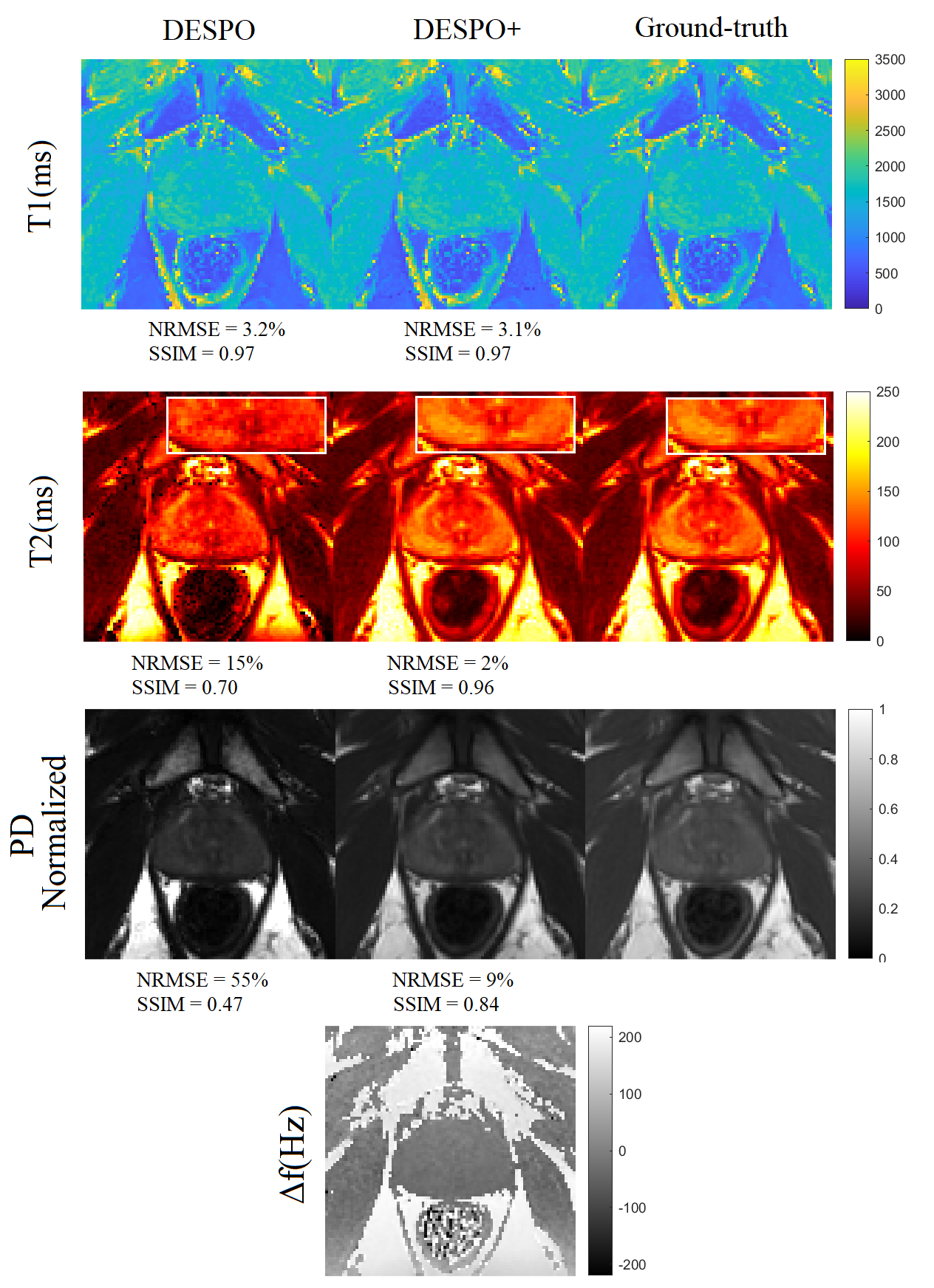
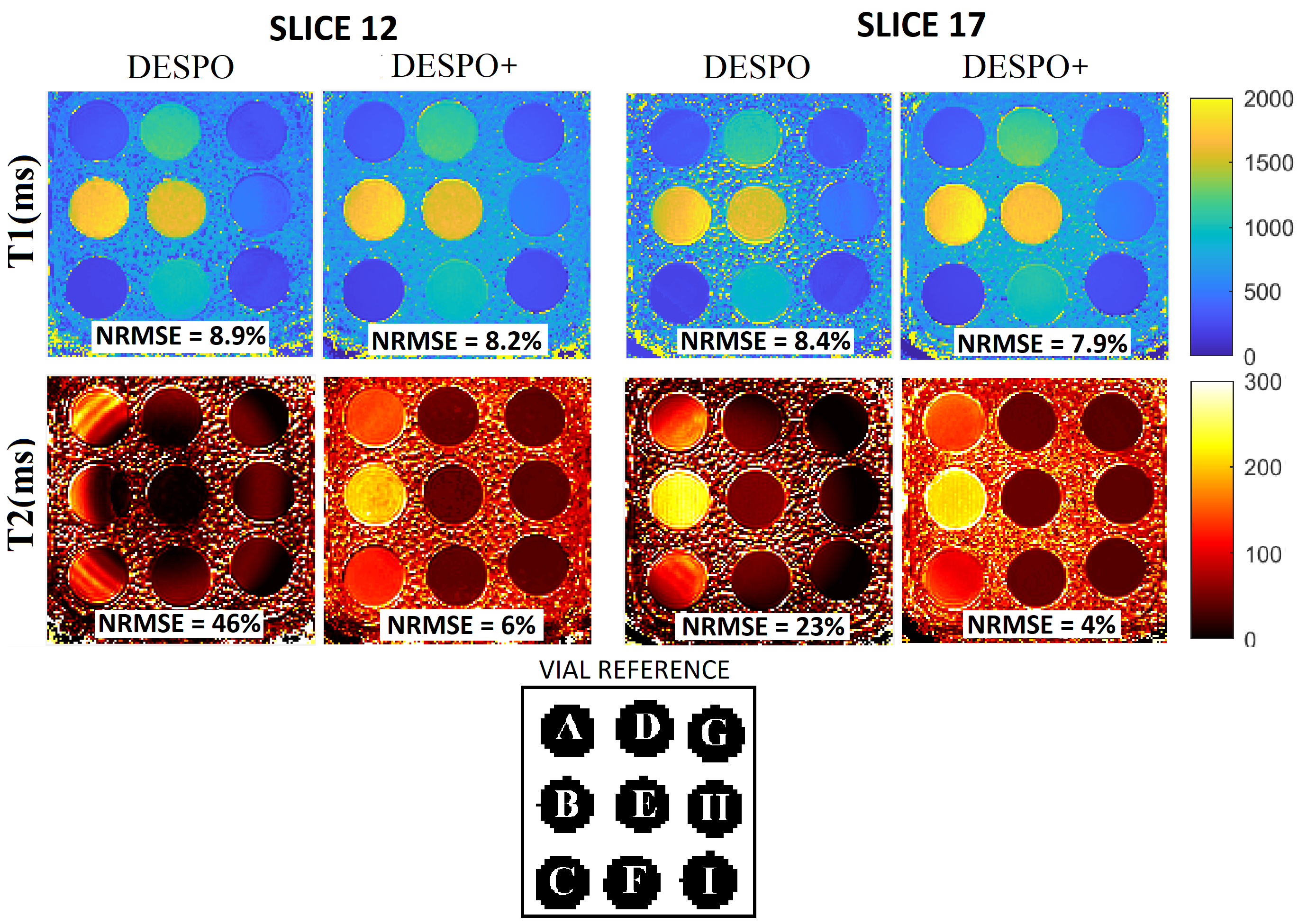
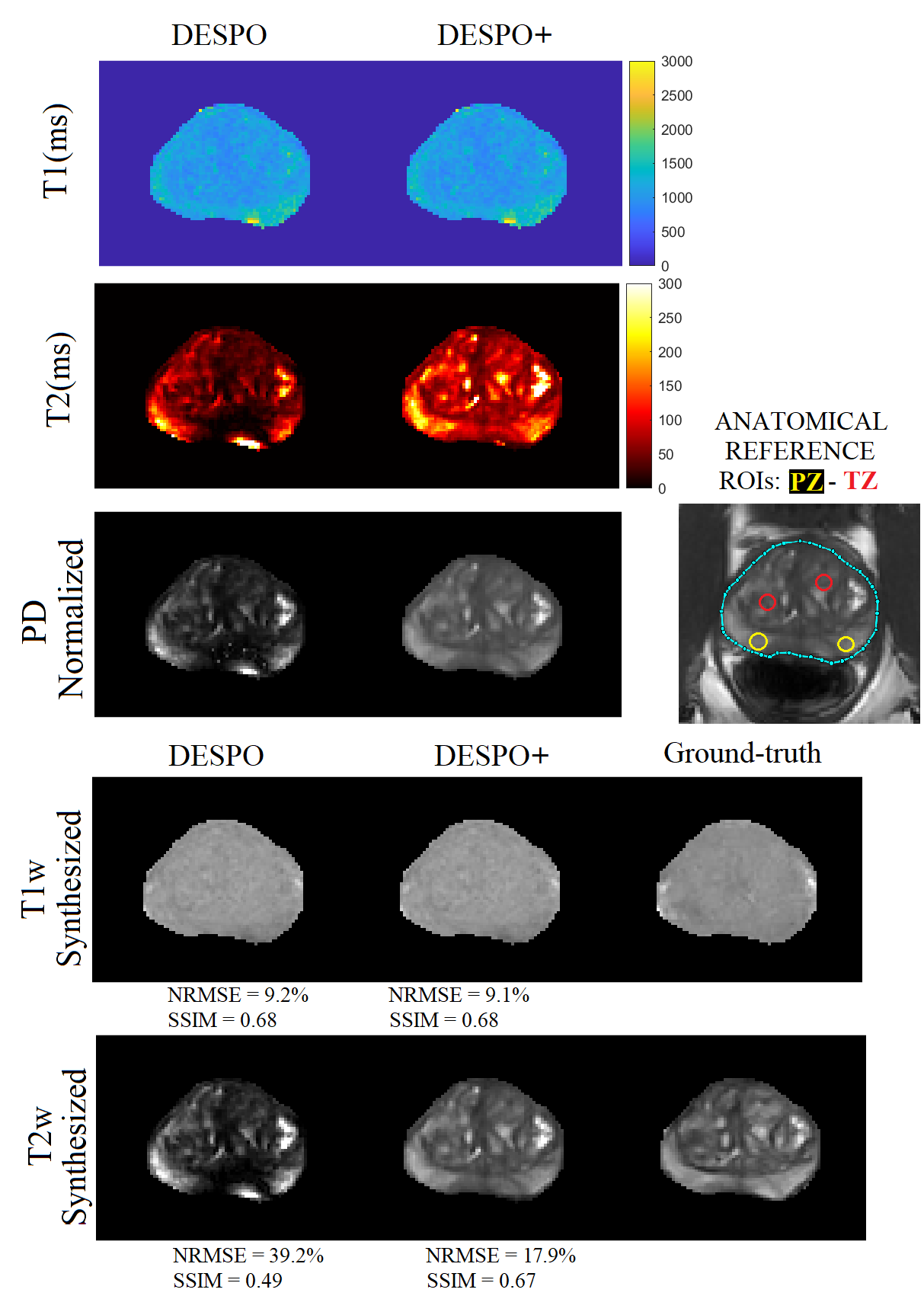
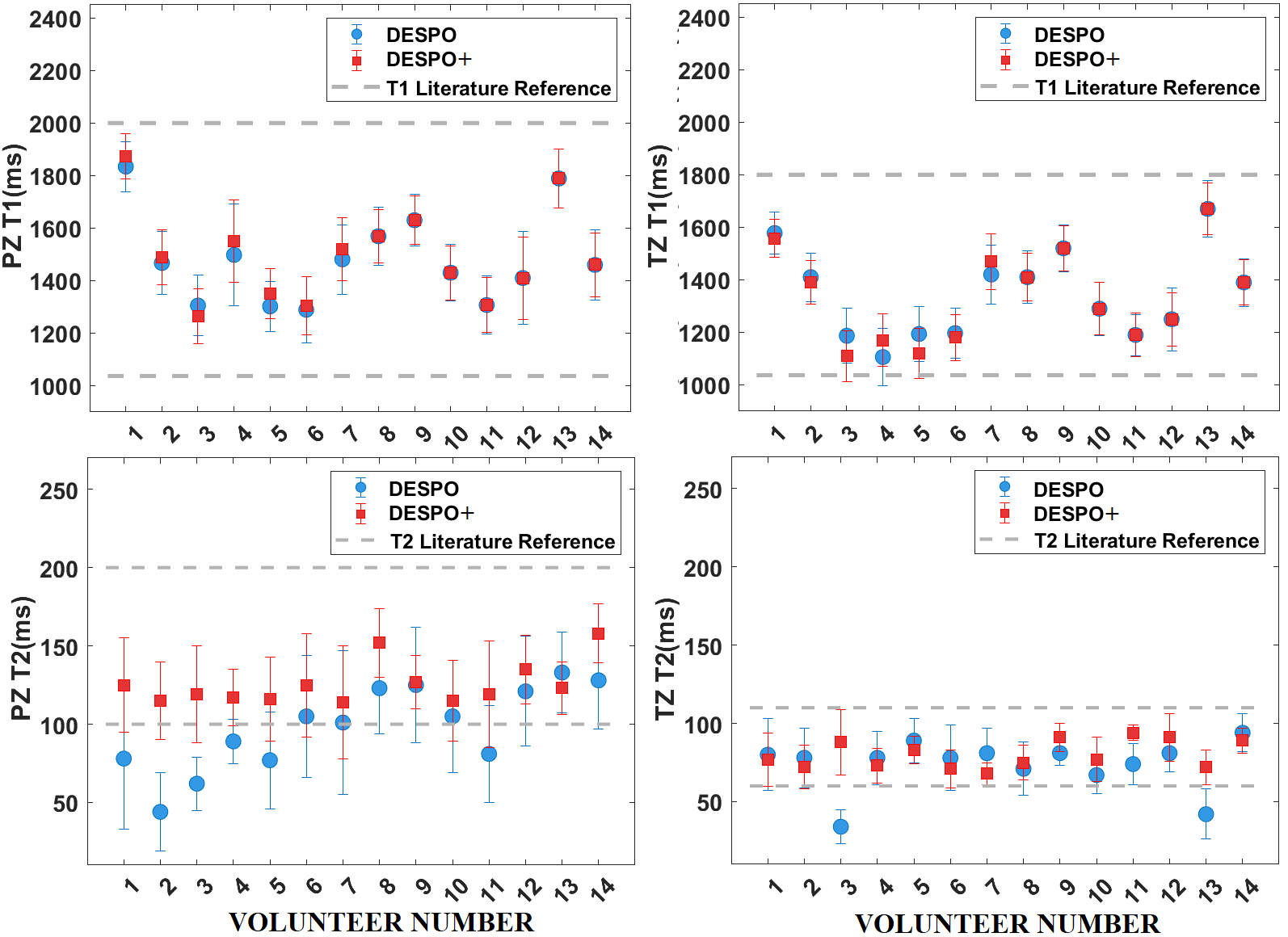
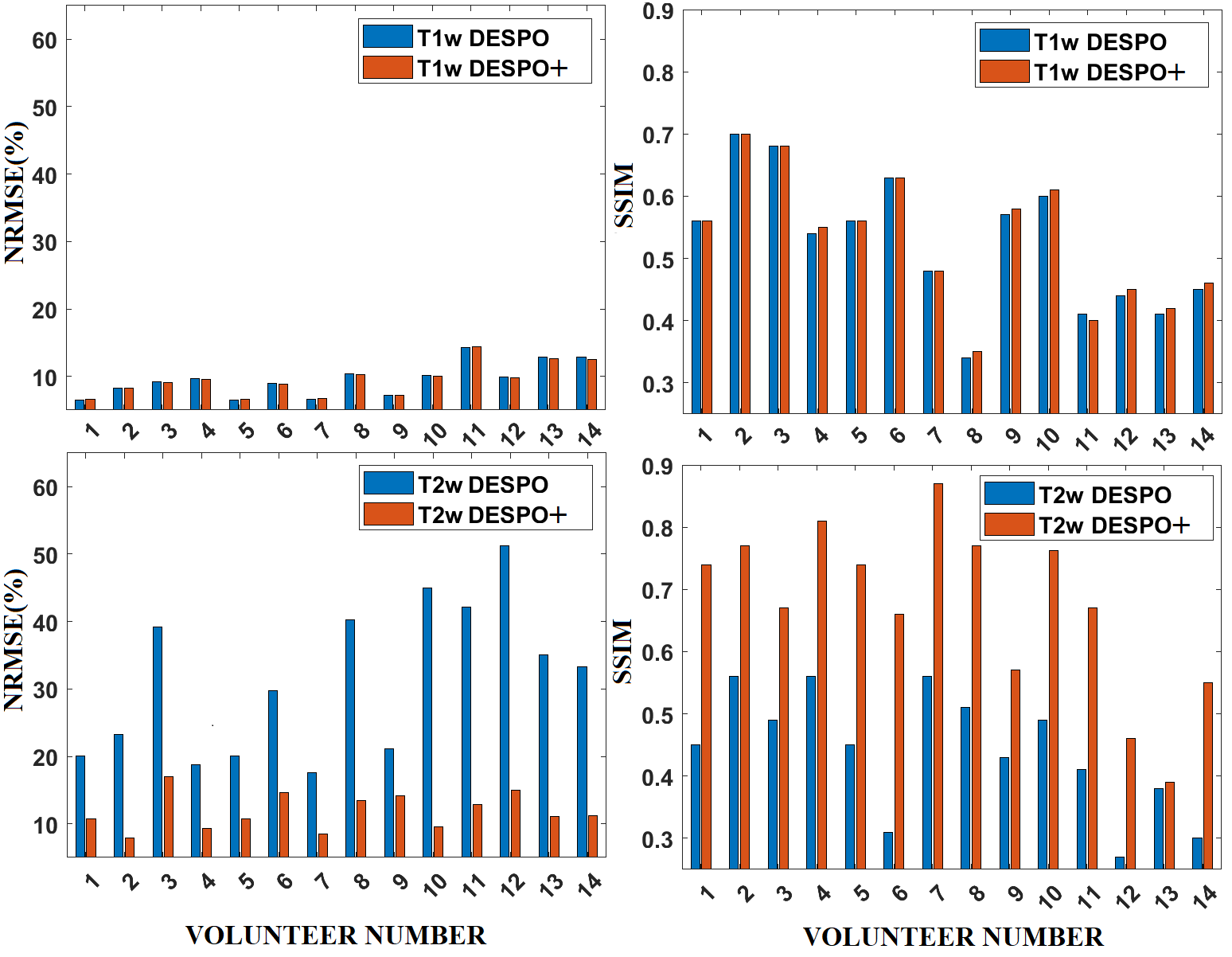
Figure 1 shows a simulation result of the reconstructed T1/T2/PD maps employing DESPO+ and the conventional DESPO. DESPO shows a signal loss or underestimation of T2 and PD values. This is more evident in the peripheral zone (PZ), as indicated by the zoom areas (white rectangles). This coincides with the high NRMSE errors of 55% for PD and 15% for T2. In contrast, DESPO+ significantly reduces these NRMSEs to 9% for PD and 2% for T2, demonstrating a substantial improvement. Figure 2 shows slices 12 and 17 reconstructed for T1/T2 maps using DESPO+ and the conventional DESPO. The vendor supplied ground-truth values for each vial utilised3. T2 maps reconstructed using DESPO exhibit pronounced signal loss due to the characteristic dark banding artifacts. This outcome corresponds to the markedly high NRMSEs for DESPO compared to the ground truth: 46% for slice-12 and 23% for slice-17. In contrast, DESPO+ reduces these NRMSEs to 6% for slice-12 and 4% for slice-17. For in-vivo, DESPO in Figure 3 displays considerable underestimation (dark zones), especially in the vicinity of the PZ. The T2 maps generated by DESPO+ successfully restore the signal loss from banding artifacts. Figure 4 shows T2 underestimation by DESPO in PZ, where DESPO+ agrees well with the literature. This discrepancy comes from susceptibility differences at the rectum-prostate interface. Figure 5 shows that DESPO+ has lower NRMSEs and higher SSIMs than DESPO in the synthetization of T1w/T2w.Conclusion
DESPO+ provides an off-resonance insensitive and customizable solution, enabling high-resolution 3D T1/T2 mapping and synthesized T1-weighted/T2-weighted images for the entire prostate, all achieved within a short scan time of 3.6 minutes, similar to DESPO.Acknowledgements
This work was funded by Fondecyt 1210648 and 1210747, and Millennium Science Initiative Program ICN2021_004 (iHealth)References
1. Deoni SCL, Rutt BK, Peters TM. Rapid combined T1 and T2 mapping using gradient recalled acquisition in the steady state. Magn ReasonMed2003;49:515–526.
2. Deoni SCL. Transverse relaxation time (T2) mapping in the brain with off-resonance correction using phase-cycled steady-state free precession imaging. J Magn Reson Imaging 2009;30:411–417.
3. G. Captur et al., “A T1 and ECV phantom for global T1 mapping quality 708 assurance: The T1 mapping and ECV standardisation in CMR (T1MES) 709 program,” J. Cardiovascular Magn. Reson., vol. 18, no. S1, p. W14, 710 Jan. 2016.
Figures