1237
Image2Flow: Fast Calculation of Pulmonary Artery Flow Fields from 3D Cardiac MRI Using Graph Convolutional Neural Networks1Institute of Cardiovascular Science, University College London, London, United Kingdom
Synopsis
Keywords: Analysis/Processing, Machine Learning/Artificial Intelligence
Motivation: Computational fluid dynamics (CFD) is used for non-invasive cardiovascular hemodynamic assessment, but it is limited by time-consuming manual segmentation and expertise needed for simulation.
Goal(s): Improve the speed and simplify volume mesh generation and CFD flow field calculation.
Approach: Develop a single deep-learning model capable of reconstructing the pulmonary artery from a 3D cardiac MRI as a volume mesh and predicting CFD-like pressure and flow.
Results: Our model achieves accurate pulmonary artery reconstruction with a median Dice score of 0.9. It computes CFD-like pressure and flow with median errors of 14.9% and 9.0%, respectively. Our model is ~10,000 times faster than manual calculation.
Impact: Image2Flow is a single-pass deep-learning model that rapidly and accurately reconstructs pulmonary artery volume meshes from 3D cardiac MR and predicts CFD-like flow fields. Our model can potentially streamline and expedite cardiovascular haemodynamic assessment and facilitate more efficient treatment planning.
Introduction
Computational fluid dynamics (CFD) can be used to non-invasively assess cardiovascular hemodynamics and predict physiological response to treatment in congenital heart disease.[1] However, its clinical feasibility is limited due to time-consuming segmentation, volume mesh generation and computationally intensive CFD simulation. [2]Therefore, we propose a single-pass deep-learning model that can rapidly reconstruct a pulmonary artery (PA) volume mesh from 3D whole heart MR (WH-MR) and predict CFD-like blood pressure/flow fields without separate segmentation, meshing and CFD simulation steps.
Methods
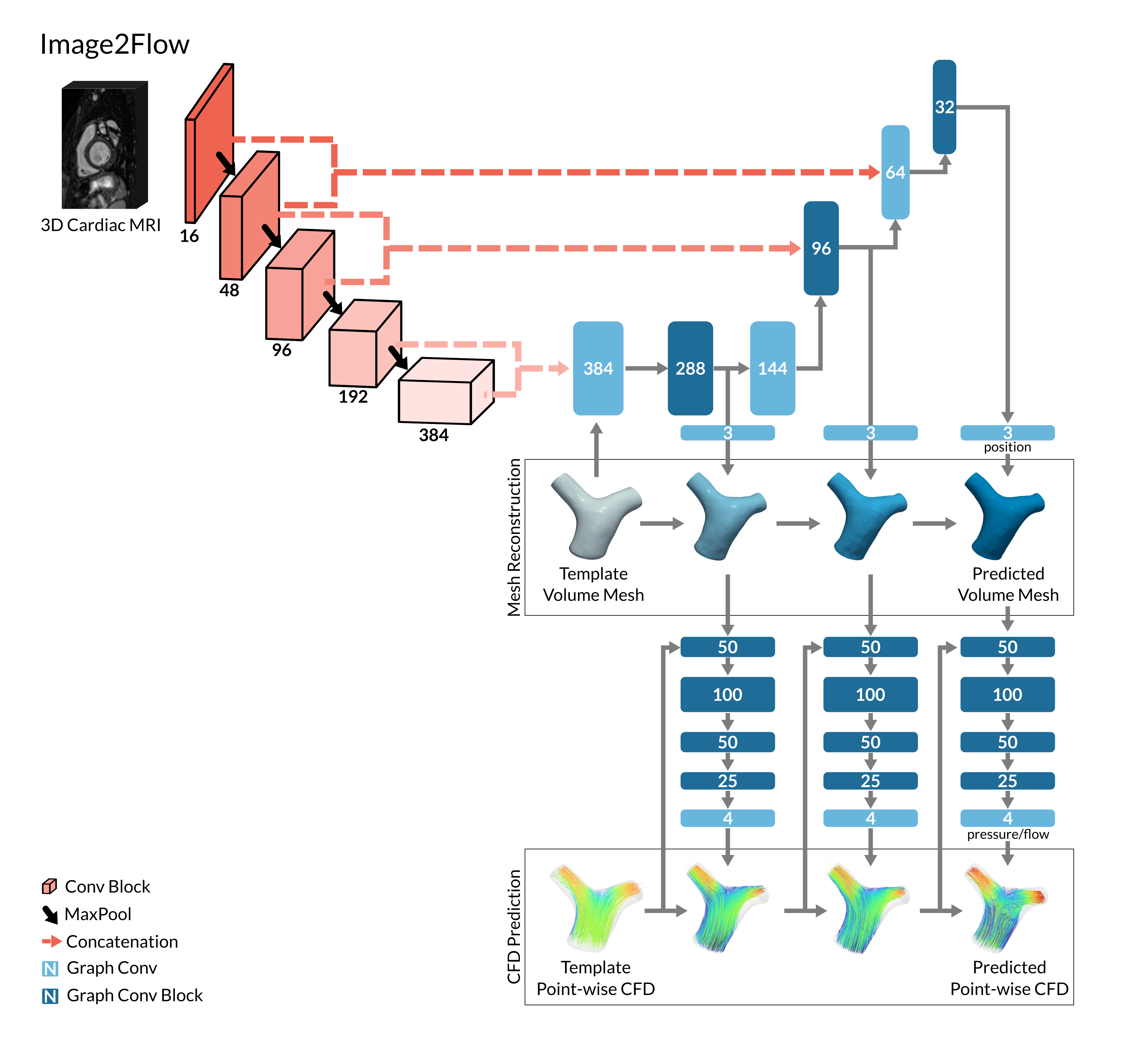
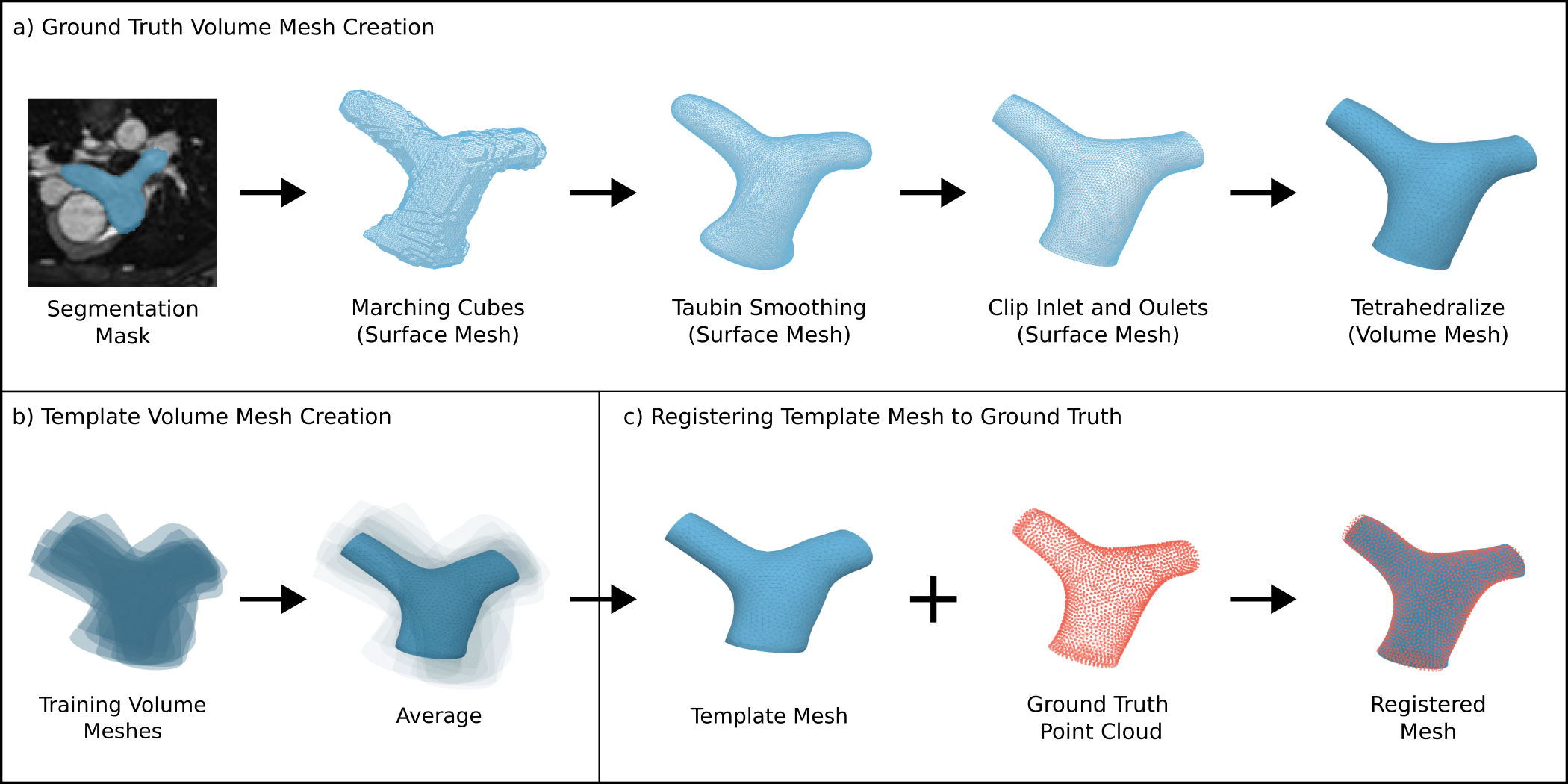
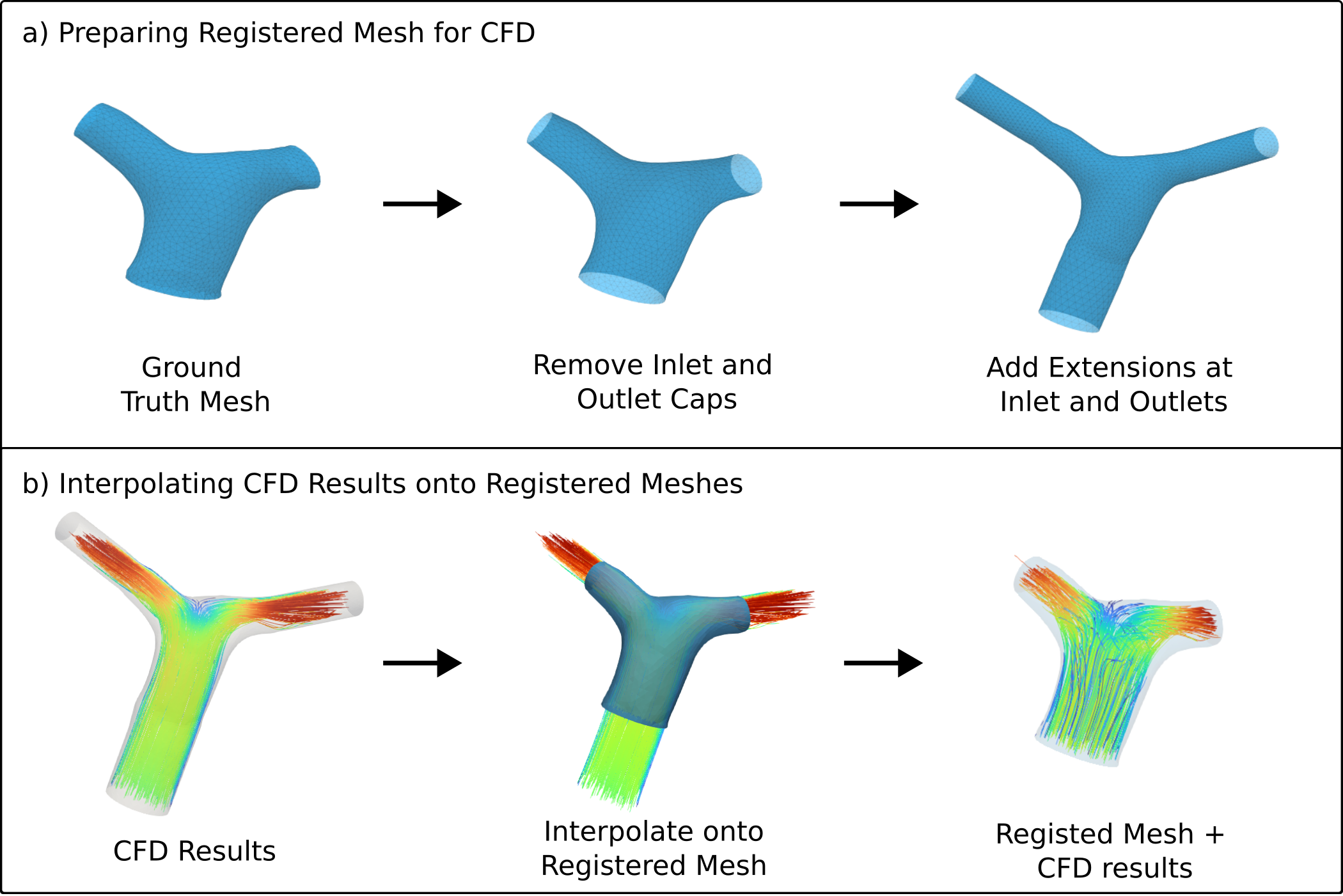
Our deep learning model, Image2Flow (Figure 1), was based on MeshDeformNet.[3] Image2Flow has an image encoding arm and a template deformation arm. The encoding arm takes the 3D WH-MR data and processes it through image convolutions. The deformation arm takes a template mesh (initialized with average pressure and flow values at each node) as a graph and performs a series of graph convolutions after concatenation with features from the image encoding arm. During each deformation block, the spatial node coordinates, as well as the pressure and flow values at each node are updated to better suit the ground truth CFD flow fields.For training data, pulmonary arteries were manually segmented on 135 3D WH-MRs (split 110/10/15 for training/validation/testing). The segmentation masks were used to generate surface meshes, with inlets and outlets being manually clipped. Extensions were added to the clipped surface which were then converted to volume meshes with 9000 nodes (Figure 2a) using Vascular Modelling ToolKit (VMTK). CFD flow fields were then calculated on these meshes using Ansys Fluent, with a 0.2m/s inflow velocity.
The template volume mesh was created by averaging the training meshes (Figure 2b). Subsequently, all ground truth meshes were registered with the template to establish spatial point correspondence across the meshes (Figure 2c). Registration was performed using the mesh reconstruction component of Image2Flow (Figure 1), which produced highly accurate results, with a median Dice score of 0.98 (0.97 – 0.98). The pointwise CFD results were then projected onto the point correspondent meshes (Figure 3).
The neural network input consisted of the raw 3D WH-MR data and the template mesh with CFD flow fields, while the output was the registered volume meshes with CFD flow fields (Figure 1).
The mesh reconstruction losses consisted of various components: a chamfer loss to guarantee accurate vertex positions; an edge length deviation loss to promote uniform-sized tetrahedral elements and to maintain surface smoothness; a coplanar cap loss to ensure flat inlet and outlet caps; and an aspect ratio loss to ensure a high-quality mesh without self-intersections. Additionally, our CFD loss is calculated using the mean squared-error on the pointwise pressure/flow.
In the test data set, the segmentation accuracy of our model was measured using a Dice score after converting the volume meshes into binary masks. We also calculated the normalized absolute error (NAE) for pressure and velocity at each node to enable a meaningful comparison of results between subjects. NAE is the pressure/velocity at each node in the ground truth mesh subtracted by the corresponding pressure/velocity in the predicted mesh divided by the range of values in the ground truth mesh. We then calculate the mean error by averaging the NAE across all the nodes in the mesh (MNAE).
Results
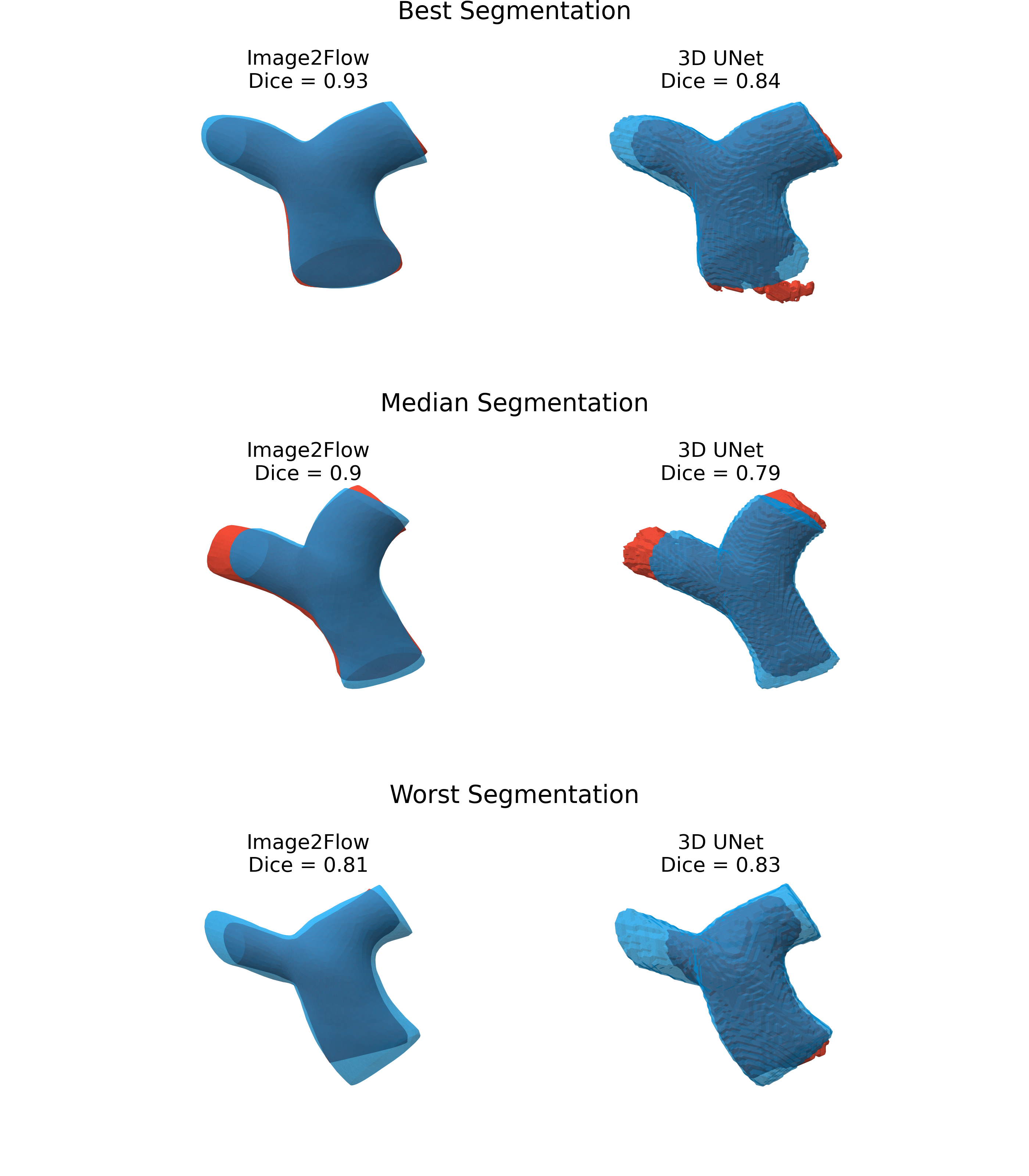
Image2Flow demonstrated an inference time of ~230ms per 3D dataset, compared to ~30 minutes for manual segmentation and 10 minutes for CFD calculation.Model validation on 15 datasets showed good segmentation accuracy (Figure 4), with a median Dice score for Image2Flow of 0.90 (0.87 – 0.91). In comparison, the conventional 3D UNet (segmentation alone) only achieved a Dice score of 0.83 (0.73 – 0.87).
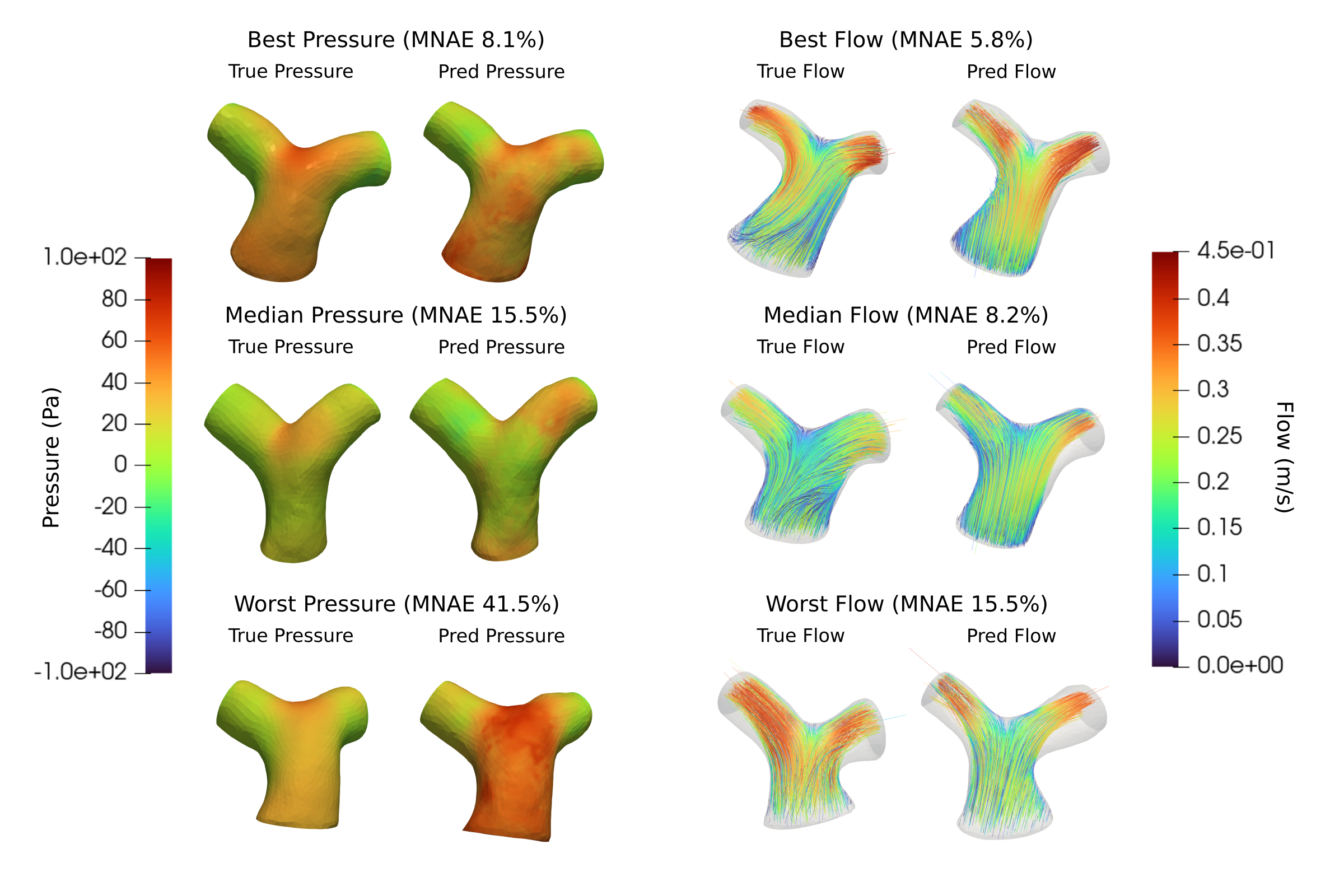
The same model also provided relatively good estimates of CFD flow fields (Figure 5). Image2Flow achieved a pointwise MNAE of 14.9% (11.1 – 21.2%) for pressure and 9.0% (8.5 – 9.9%) for flow.
Conclusion
To our knowledge, this is the first study that uses a graph-based DL model to efficiently segment and estimate flow fields in the pulmonary arteries directly from 3D whole heart data.Unlike previous methods that focused on surface mesh generation [3,4], Image2Flow, not only directly generates volume meshes (that could be used for CFD simulation), but also makes estimates of flow fields in a single-pass. Image2Flow has an inference time of only 230 ms, making our approach approximately 10,000 times faster than traditional manual segmentation and CFD calculations. This substantial acceleration has the potential to significantly impact clinical practice by expediting cardiovascular assessments and facilitating more efficient treatment planning.
Acknowledgements
No acknowledgement found.References
- Morris PD, Narracott A, von Tengg-Kobligk H, Soto DA, Hsiao S, Lungu A, Evans P, Bressloff NW, Lawford PV, Hose DR, Gunn JP. Computational fluid dynamics modelling in cardiovascular medicine. Heart. 2016 Jan 1;102(1):18-28.
- Pajaziti E, Montalt-Tordera J, Capelli C, Sivera R, Sauvage E, Quail M, Schievano S, Muthurangu V. Shape-driven deep neural networks for fast acquisition of aortic 3D pressure and velocity flow fields. PLOS Computational Biology. 2023 Apr 24;19(4):e1011055.
- Kong F, Wilson N, Shadden S. A deep-learning approach for direct whole-heart mesh reconstruction. Medical image analysis. 2021 Dec 1;74:102222.
- Kong F, Shadden SC. Learning Whole Heart Mesh Generation From Patient Images for Computational Simulations. IEEE Transactions on Medical Imaging. 2022 Nov 3;42(2):533-45.
Figures