1230
Integrated Multi-label 3D Deep Learning Multi-task Model for Intelligent MR Spine Scan Planning1GE Healthcare, Bangalore, India, 2GE Healthcare, Niskayuna, NY, United States
Synopsis
Keywords: Analysis/Processing, Spinal Cord, Localizer images, MRI, Spine, Segmentation, Deep Learning
Motivation: Obtaining consistent spine MRI images irrespective of patient posture, spine deformities, and technologists’ skills, with minimal disruption in the existing workflow.
Goal(s): To develop an intelligent scan plane prescription for spine MRI using deep learning on regular 3-plane localizer images.
Approach: We adopted a multi-resolution CNN network for multiple segmentation tasks - spine vertebrae, intervertebral disc (IVD), and saturation band (SB) across all the spine stations (cervical, thoracic, and lumbar) and orientations (sagittal and coronal).
Results: We reported good segmentation of vertebrae and IVD, along with consistent SB placement with angle error of less than 5 degree and no overlap with the spine region.
Impact: We present a first-of-its-kind integrated multi-label 3D DL model that operates on 2D 3-plane regular localizers to aid consistent MRI scan planning. This model combines MRI localizer images across orientation, across spine stations, and across multiple imaging tasks.
Introduction
In spine, anatomical details that are important for MR scan planning can be spine vertebrae for scan coverage and bounding box orientation, intervertebral disc (IVD) information for planning axial scan, or saturation band (SB) placement to suppress noise signals from nearby large pulsating blood vessels. Identifying of these anatomies is done using low-resolution localizer images, however, the quality of the scan is highly dependent on the expertise of the technologist1. Automatic identification of these anatomical details dramatically simplifies the scan planning2-3, making it robust against patient position, anatomical variabilities, and technologist expertise. Individual models, to automate scan planning components, can be found in the literature4, however, an integrated model that provides multiple anatomical identification details is not reported yet. In this work, we present such an integrated Deep Learning (DL) model.Methods
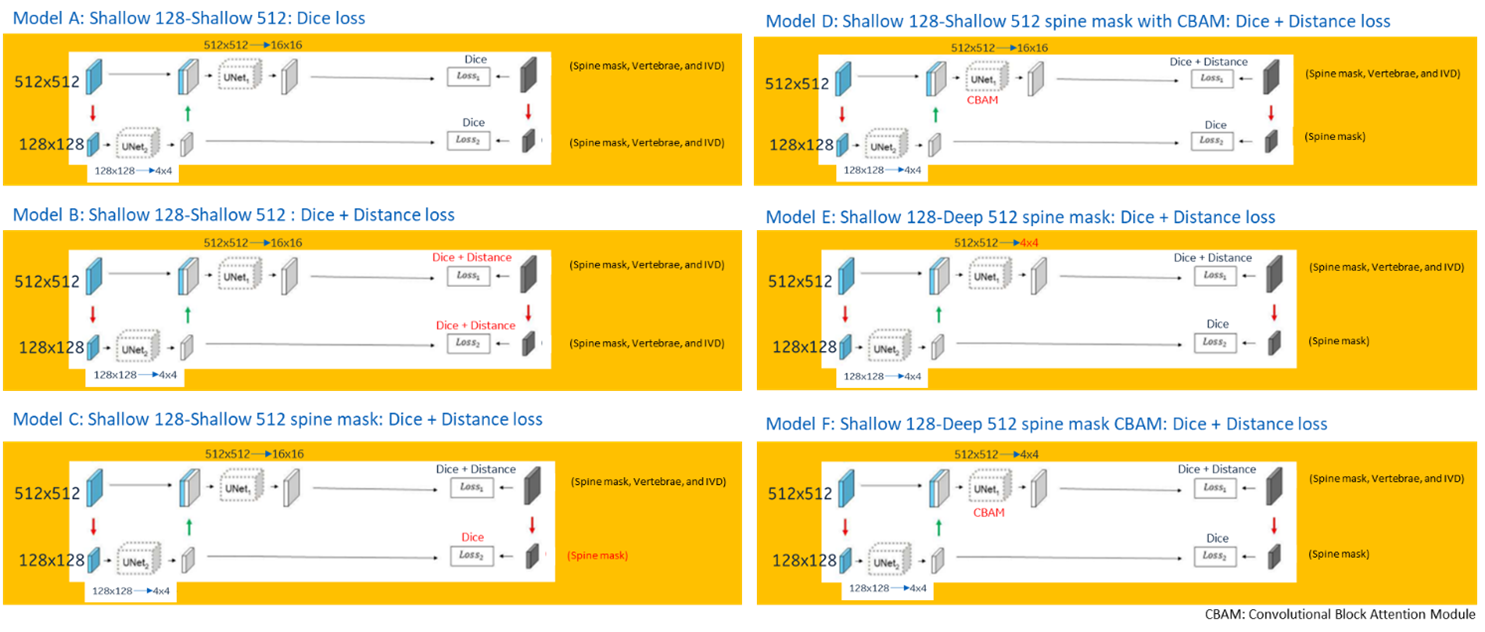
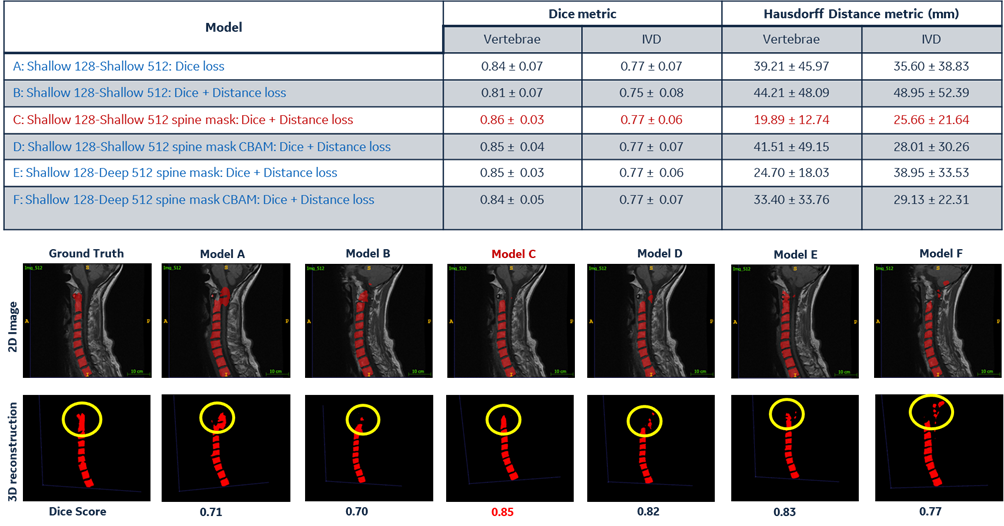
Data: A total of 122 cervical, 65 thoracic, and 181 lumbar scans were included in this study, which includes straight sagittal and coronal localizer images acquired with single-shot fast spin echo (SSFSE). The data had variations in coverage, resolution, and imaging FOV. Ground truth (GT) masks (vertebrae and disc) were generated using the high resolution sagittal T1w images. We used rigid image registration (Elastix3) to transfer the GT masks in localizer images. From the vertebrae and IVD point cloud, an alpha shape5 spine mask was generated. Using these labels, SB plane mask was generated for sagittal images4. In coronal images, SB plane mask was taken as spine bounding box.DL Model details: The backbone of our model is a multi-resolution approach, wherein, first the images are down sampled to low spatial resolution (128x128) and fed into a CNN network to localize the anatomy. The predictions from the first network are merged with the original up sampled image (512x512) and fed into another CNN network for the segmentation tasks. Both the networks are trained simultaneously using either dice alone or combination of dice with distance loss function. We first performed experiments on high resolution T1w images to choose an optimal model configuration. Fig-1 shows various configurations tested in this study. Based on the performance of these models, we chose the best model configuration (Maximum dice and least Hausdorff distance metric6) for training the localizer dataset. The dataset was augmented using random rotations, cropping and intensity changes. The prediction of the model was evaluated using Dice score for vertebrae and IVD segmentation. For SB placement, minimum distance (MD_V > 0) between DL-estimated planes and spine vertebrae was used. We also evaluated the SB plane fitting against GT plane using angle error (< 5 degree).
Results and Discussion
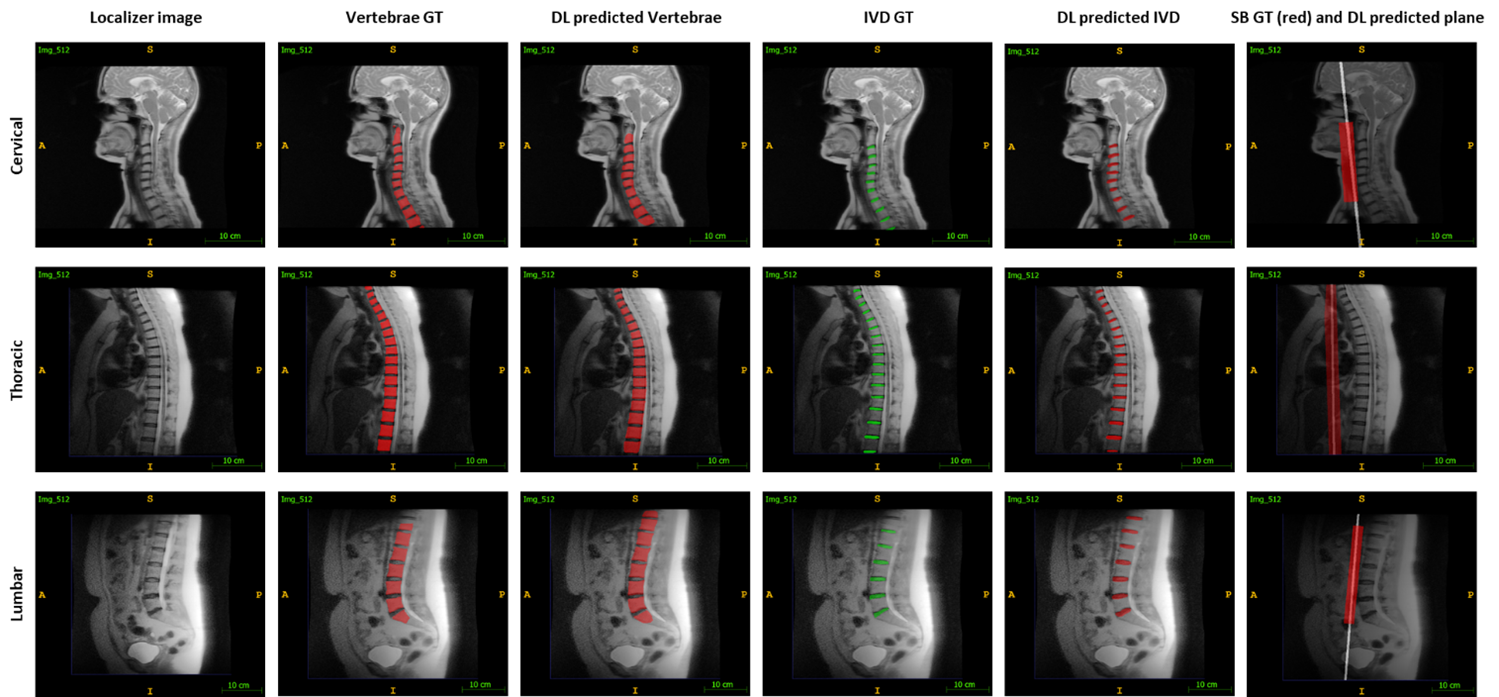
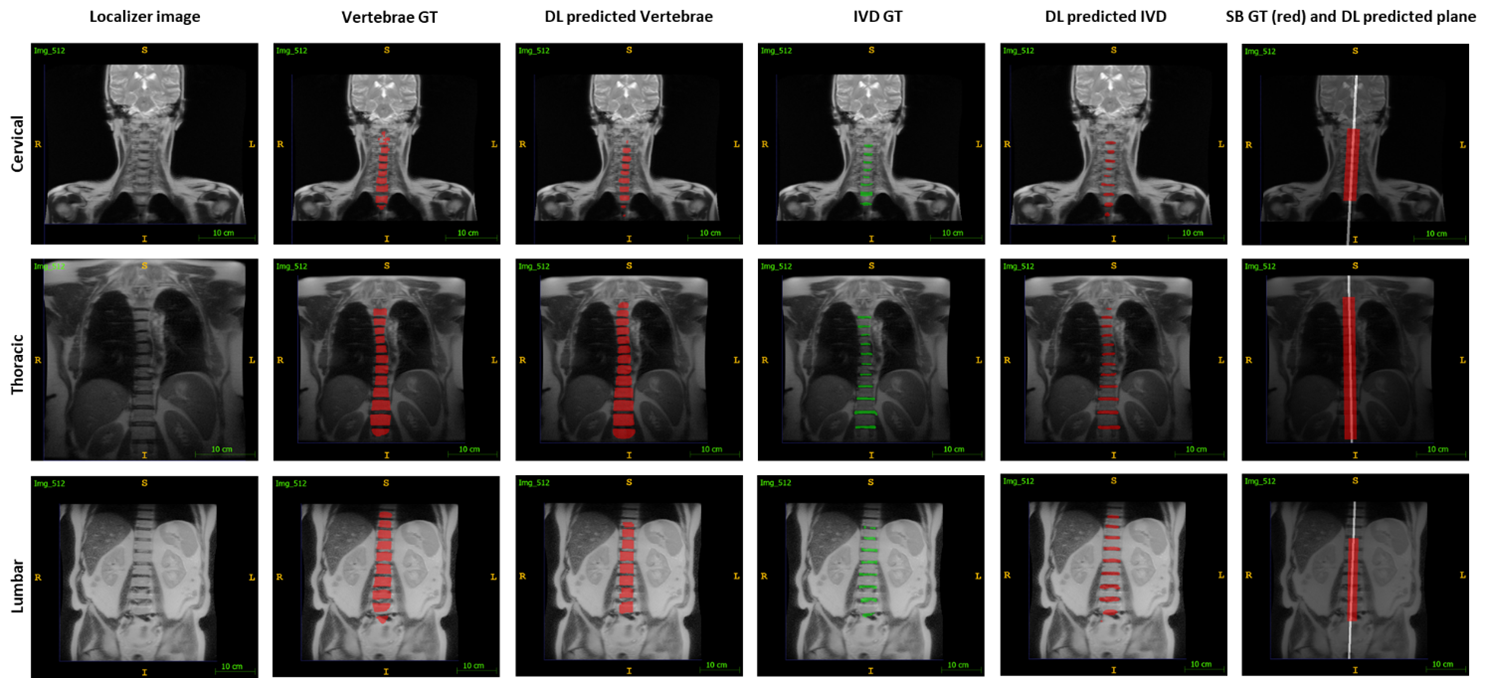
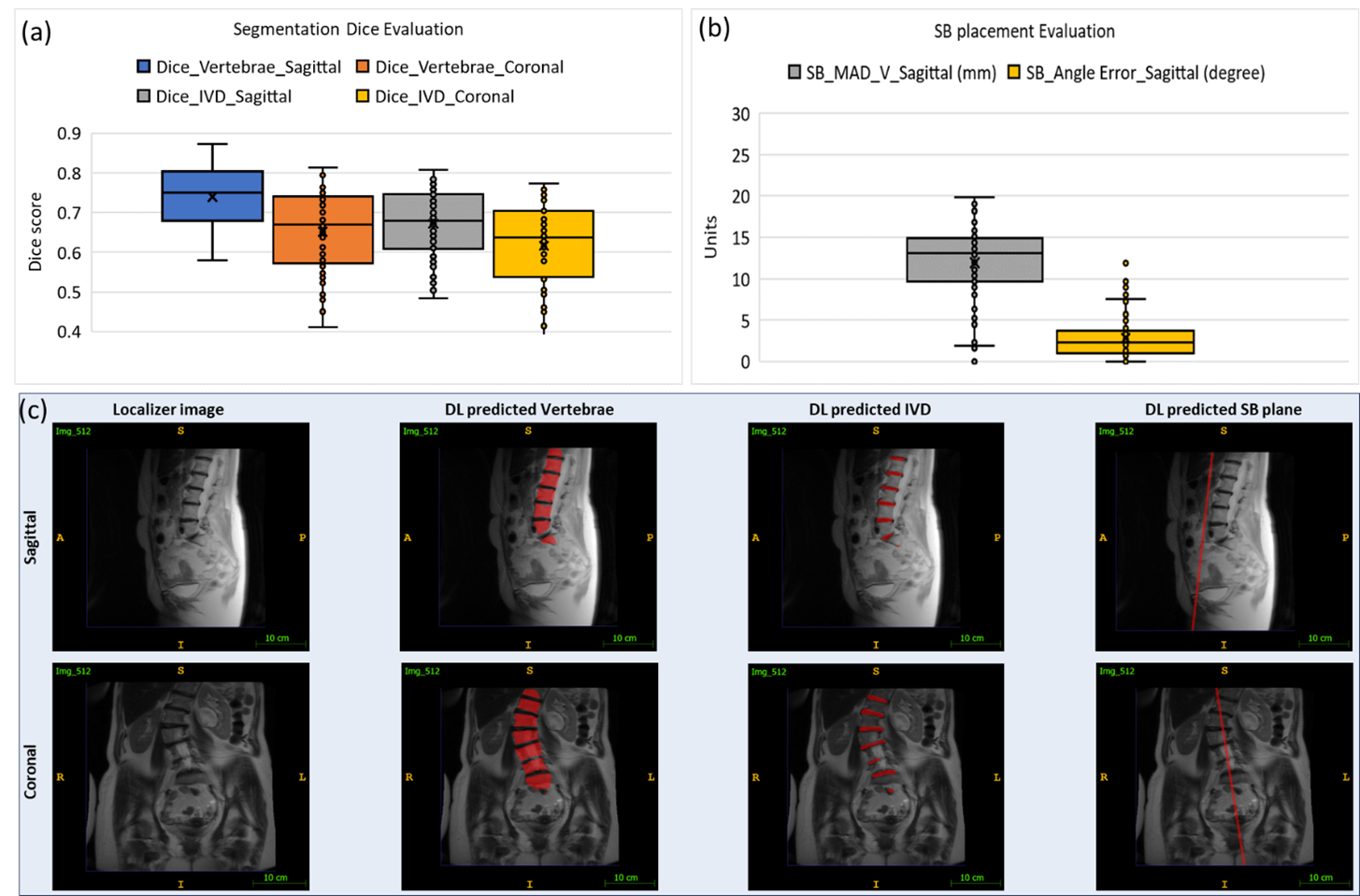
From the optimal model configuration selection experiment, we found that Model C (Fig-2) performs the best. Hence, using Model C, we trained and evaluated the localizer data set. Fig-3 and Fig-4 show predictions on sagittal and coronal localizer images, respectively. In coronal images, segmentation performed poorer compared to sagittal (Fig-5a). Lower Dice scores could be attributed to several factors. First, GT masks were transferred from high resolution to 3-plane localizer images, which typically have larger FOV than the high-resolution images. Second, data were cropped during training process to retain only the labelled vertebrae regions, thereby introducing voids in the image. We hypothesize that this process should be emulated during the inference process that can further improve the predictions. Third, due to computational constraints, the model was trained using random sampling of the training dataset, wherein random 500 dataset was shown to the model in every epoch. Performance of this model can be argued to be inferior compared to the model trained with all the data seen in the same epoch. Irrespective of the lower Dice score, the impact in the used case for scan planning is expected to be minimal to none. Furthermore, in case of SB placement, the model performed superior with less than 5% average angle error and the distance from the vertebrae was found to be 11.91 ± 4.67 mm (Fig-5b). We further tested our model on spine scoliosis cases. Fig-5c shows the DL predictions for one such scoliosis case.Conclusion
We trained a DL-based integrated model, for MRI localizer images, that works across multiple spine stations (cervical, lumbar, and sacral), multiple scan orientations (sagittal and coronal), and multiple use cases (vertebrae, disc, and saturation band segmentation). To the best of our knowledge, this is a first-of-its-kind integrated model to assist spine MR scan planning.Acknowledgements
No acknowledgement found.References
- Serai, Suraj D., et al. "Newly developed methods for reducing motion artifacts in pediatric abdominal MRI: tips and pearls." American Journal of Roentgenology 214.5 (2020): 1042-1053.
- Lecouvet FE, et al. “Clinical evaluation of automated scan prescription of knee MR images.” Journal of Magnetic Resonance Imaging: An Official Journal of the International Society for Magnetic Resonance in Medicine. 2009 Jan;29(1):141-5.
- S. Klein, et al. "elastix: a toolbox for intensity based medical image registration," IEEE Transactions on Medical Imaging, vol. 29, no. 1, pp. 196 - 205, January 2010.
- Ashish Saxena et al. “Deep learning-based saturation band placement in spine localizer images.”, ISMRM 2023, Toronto, Canada.
- Edelsbrunner, Herbert. "Alpha shapes-a survey." Tessellations in the Sciences: Virtues, Techniques and Applications of Geometric Tilings. 2011.
- E. Belogay, et al. “Calculating the Hausdorff distance between curves.” Information Processing Letters, 1997, v. 64, pp. 17-22.
Figures