1227
Helmet RF Applicator Enhances Thermal Magnetic Resonance Theranostics of Brain Tumours1Berlin Ultrahigh Field Facility (B.U.F.F.), Max-Delbrück Center for Molecular Medicine in the Helmholtz Association, Berlin, Germany, 2FG Theoretische Elektrotechnik, Technische Universität Berlin, Berlin, Germany, 3Berliner Hochschule für Technik, Berlin, Germany, 4Chair of Medical Engineering, 3Technische Universität Berlin, Berlin, Germany, 5MRI.TOOLS GmbH, Berlin, Germany, 6Charite’ Universitätsmedizin, Berlin, Germany, 7a joint cooperation between the Charité Medical Faculty and the Max-Delbrück Center for Molecular Medicine, Berlin, Germany
Synopsis
Keywords: RF Arrays & Systems, RF Arrays & Systems, Novel soil design, Brain MRI, 7T, Hyperthermia, Thermal MR, Theranostics, Simulations, Experiments
Motivation: Thermal MR adds an interventional dimension to an MRI device. Ultrahigh-field MRI is an excellent fit for ThermalMR since it benefits from multi-channel transmission in the short wavelength regime
Goal(s): This work investigates the MRI and RF heating performance gain of a multi-channel Tx in a helmet array versus an annular array.
Approach: We aim to enhance B1+ uniformity for brain MRI at 7.0T and enhance SAR10g for brain thermal therapy using perpendicular RF elements.
Results: Our simulations and phantom experiments demonstrate superior mean B1+ coverage and better B1+ uniformity for MRI and enhanced SAR10g for thermal therapy using the helmet configuration.
Impact: Dome-shaped helmet transmit RF applicators provide a viable alternative for theranostics involving ultrahigh-field MRI and targeted RF-heating for thermal therapy The performance gain of the helmet transmit RF applicator is demonstrated in numerical simulations and in experiments at 7.0 T.
Introduction
ThermalMR integrates MRI diagnostics and targeted RF heating for thermal therapy in a single theranostic device. The requirements for MRI (B1+ efficiency and uniformity) and targeted RF heating (SAR10g-based metrics1) govern the design of ThermalMR-RF-applicators(Figure1). We hypothesize that dome-shaped helmet RF arrays (HA) will improve the efficacy of ThermalMR of brain tumors versus an annular RF array (AA). To test our hypothesis, in this work we examine a dome-shaped helmet ThermalMR applicator comprising eight broadband self-grounded bow-tie (bbSGBT) antennae2-4 arranged in an annular array plus two bbSGBT placed on top of the head perpendicular to B0. An annular RF applicator comprised of 10 transmit bbSGBT elements is used as a reference.Methods
Electromagnetic field (EMF) simulations were primarily performed in CST Microwave Studio 2020 using the head of the human voxel model Duke5 at 297.2 MHz (bbSGBT Bandwidth:234-561 MHz). Considering the EMF distribution of a bbSGBT antenna (Figure2a-c) two RF arrays were investigated: i) a dome-shaped helmet array (Figure2d) and ii) an annular array (Figure2e). B1+ and SAR10g6 distribution in the region of interest (ROI) covering the brain were calculated in Matlab 2021a.MRI: For transmission field shaping, a genetic algorithm7 was used in conjunction with unconstrained minimization(fminunc)8. To assess the MRI performance, the metrics B1+ efficiency, mean B1+, min B1+and relative standard deviation (SD) of B1+ divided by the mean value of the coefficient of variation of B1+/(CoV=SD/mean)9 were used.
RF heating: Constructive E-field interference in the target volume (TV) was achieved with a time multi-plexed focusing method10. To evaluate the quality of targeted RF heating, we calculated maximum SAR10g (SAR10g,max). To mimic a realistic clinical scenario, a voxel model was generated from a CT scan of a patient (total head mass=3.68kg) with a glioblastoma multiforme (volume=172ml, σtumor=1.15 S/m, εrtumor=66.5)11 and imported into Sim4life (ZMT, Zurich, CH) for SAR and temperature EMF simulations. Cumulative histograms of the 10%, 50% or 90% of the masked clinical target volume (CTV) covered by a minimum temperature is defined by T10,T50,and T90, respectively.
Experimental validation: Two RF arrays were implemented at 7.0 T. i) four bbSGBT building blocks placed posterior and four placed anterior ii) bbSGBT building blocks placed posterior and three placed anterior plus bbSGBT building blocks placed perpendicular to B0. For experiments the GUFI phantom (size=45*40*10 cm3, εr=55.5)12 was used. The imaging protocol (one sagittal and one transversal slices) included: 1H: FLASH, spatial resolution=0.5x0.5x2.5 mm3, TR=50 ms, TE=2.86 ms, nominal FA=40_degree, receiver bandwidth=260 Hz/Px, scan time=1.18 minutes.
Results
MRI: For the phantom, the sum of the magnitude of the superposed B1+[µT/√W] distribution obtained for the HA in the ROI showed a 40%(IM) and 9%(RM) improvement of mean B1+ over the AA (Figure3a). For Duke, the HA provided a 51%(IM) and 30%(RM) improvement of minimum B1+ over the AA for the brain ROI (Figure3). Figure3b shows assessment of B1+ uniformity across the entire brain demonstrated a 36%(IM) and 34%(RM) SD reduction for the HA versus the AA. For the objective of maximizing B1+,min the HA showed a 35.3% improvement vs. the AA; for the objective of minimiz the CoV, the HA provided a 42% lower CoV vs. the AA; maximize the mean B1+ revealed a 21% enhancement provided by the AA vs. the HA.RF heating: SAR10g,max is increased by 20%(L1), 17%(L2), 23%(L3), and 26%(L4) for the HA vs. AA (Figure4a). SAR10g and temperature distribution shows Tmin=40.2°C using the HA and 37.4°C using the AA inside the TV of the tumour (Figure4b, fourth row). Simulation results showed T90=41.5°C, T50=43.18°C, and T10=44.54°C for the HA versus T90=38.6 °C, T50=40.63°C, and T10=43.7°C for the AA(Figure4C). Our experimental results show that placing two bbSGBT building blocks perpendicular to B0 enhances B1+ uniformity along the long axis of the phantom(Figure5).
Discussion and Conclusion
Ensuing transmission field uniformity across the brain and enhancing RF heating quality for ThermalMR requires high-density RF applicators. However, the head presents a small surface area, and thus the number of Tx elements arranged in an AA around the head is limited. To offset this constraint, the HA takes advantage of two bbSGBT Tx elements placed on top of the head. Our evaluation of the MRI quality demonstrates enhanced B1+ coverage and uniformity across the brain of the HA vs. the AA. The assessment of RF heating quality shows that the HA facilitates a ~10% improvement of SAR10g,max in the TV vs. AA. These results provide a springboard for the implementation and application of a helmet array driven by broadband bbSGBTs at 7.0 T, 10.5 T and 14.0 T.Acknowledgements
This project has received funding from the European Research Council (ERC) under the European Union's Horizon 2020 research and innovation program under grant agreement No 743077 (ThermalMR) and from the Innovative Training Network (ITN) H2020-MSCA-ITN-2020-955625 of the Marie Skłodowska-Curie Actions of the European Union.
References
1. Paulides, M.M., et al. ESHO benchmarks for computational modeling and optimization in hyperthermia therapy. Int J Hyperthermia 38, 1425-1442 (2021).
2. Eigentler, T.W., et al. Wideband Self-Grounded Bow-Tie Antenna for Thermal MR. NMR Biomed 33, e4274 (2020).
3. Eigentler, T.W., et al. 32-Channel self-grounded bow-tie transceiver array for cardiac MR at 7.0T. Magnetic resonance in medicine : official journal of the Society of Magnetic Resonance in Medicine / Society of Magnetic Resonance in Medicine 86, 2862-2879 (2021).
4. Nurzed, B., et al. Radiofrequency Antenna Concepts for Human Cardiac MR at 14.0 T. MAGMA accepted for publication(2023).
5. Christ, A. The virtual family project-development of anatomical whole-body models of two adults and two children. Proc. 23rd Annual Review of Progress in Applied Computational Electromagnetics (ACES) 2007 (2007).
6. IEEE Recommended Practice for Determining the Peak Spatial-Average Specific Absorption Rate (SAR) in the Human Head from Wireless Communications Devices: Measurement Techniques. IEEE Std 1528-2013 (Revision of IEEE Std 1528-2003), 1-246 (2013).
7. Chipperfield, A., Fleming, P. & Fonseca, C. Genetic algorithm tools for control systems engineering. in Proceedings of adaptive computing in engineering design and control, Vol. 128 133 (Plymouth Engineering Design Centre UK, 1994).
8. Coleman, T., Branch, M.A. & Grace, A. Optimization toolbox. For use with MATLAB. User’s guide for MATLAB 5(1999).
9. Mao, W., Smith, M.B. & Collins, C.M. Exploring the limits of RF shimming for high-field MRI of the human head. Magn Reson Med 56, 918-922 (2006).
10. Kuehne, A., Oberacker, E., Waiczies, H. & Niendorf, T. Solving the time-and frequency-multiplexed problem of constrained radiofrequency induced hyperthermia. Cancers 12, 1072 (2020).
11. Oberacker, E., et al. Patient-Specific Planning for Thermal Magnetic Resonance of Glioblastoma Multiforme. Cancers (Basel) 13(2021).
12. Voelker, M.N., et al. Quality assurance phantoms and procedures for UHF MRI‒the German Ultrahigh Field Imaging (GUFI) approach. in Proceedings of the Annual Meeting ISMRM. Honolulu, Vol. 3912 (2017).
13. Oberacker, E., et al. Radiofrequency applicator concepts for thermal magnetic resonance of brain tumors at 297 MHz (7.0 Tesla). Int J Hyperthermia 37, 549-563 (2020).
Figures
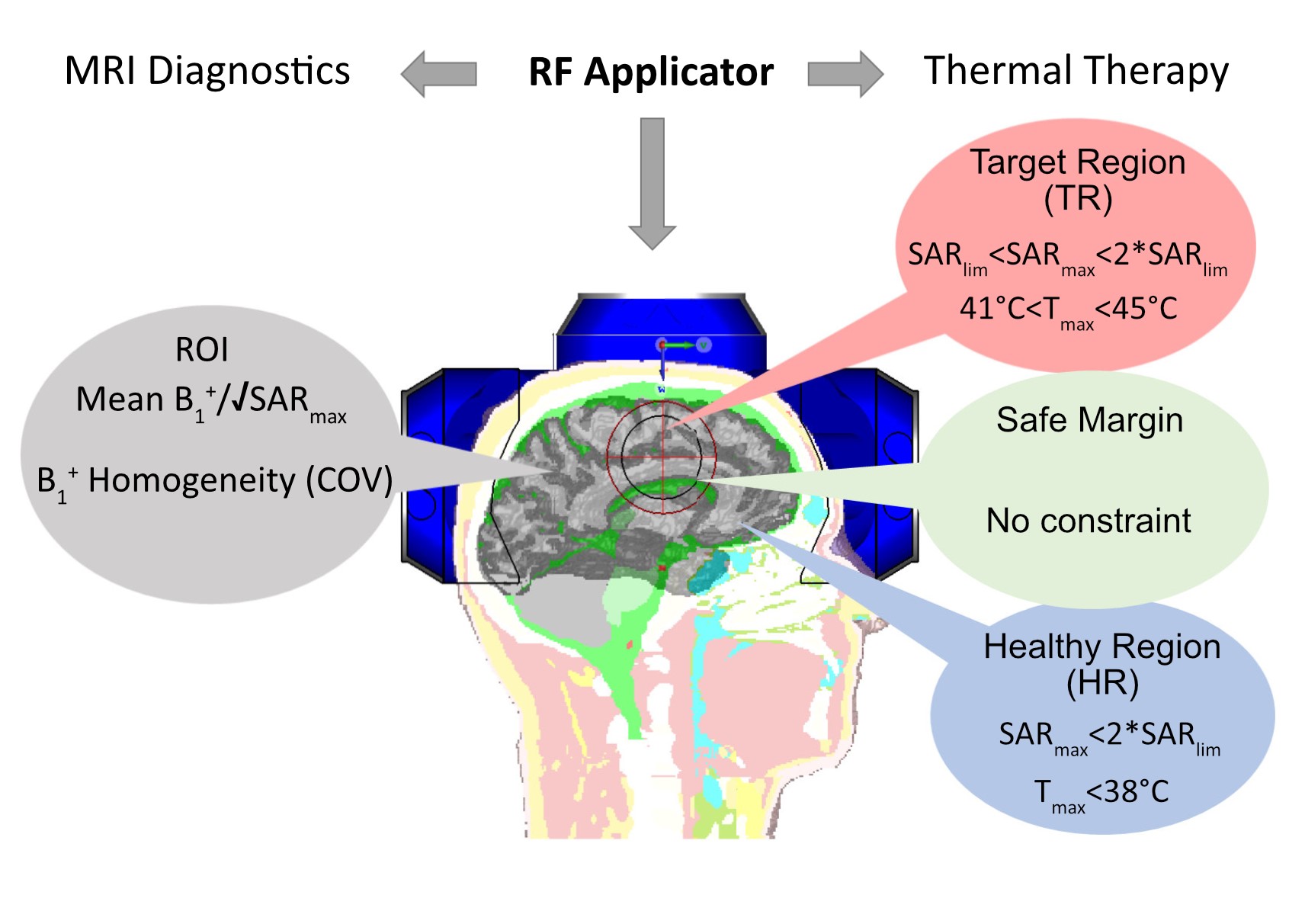
Fig. 1: ThermalMR integrates MRI diagnostics and thermal therapy in a single RF applicator. MRI diagnostics and thermal therapy have different requirements and quality metrics in the region of interest (ROI), healthy volume, target volume, and safe margin 13.
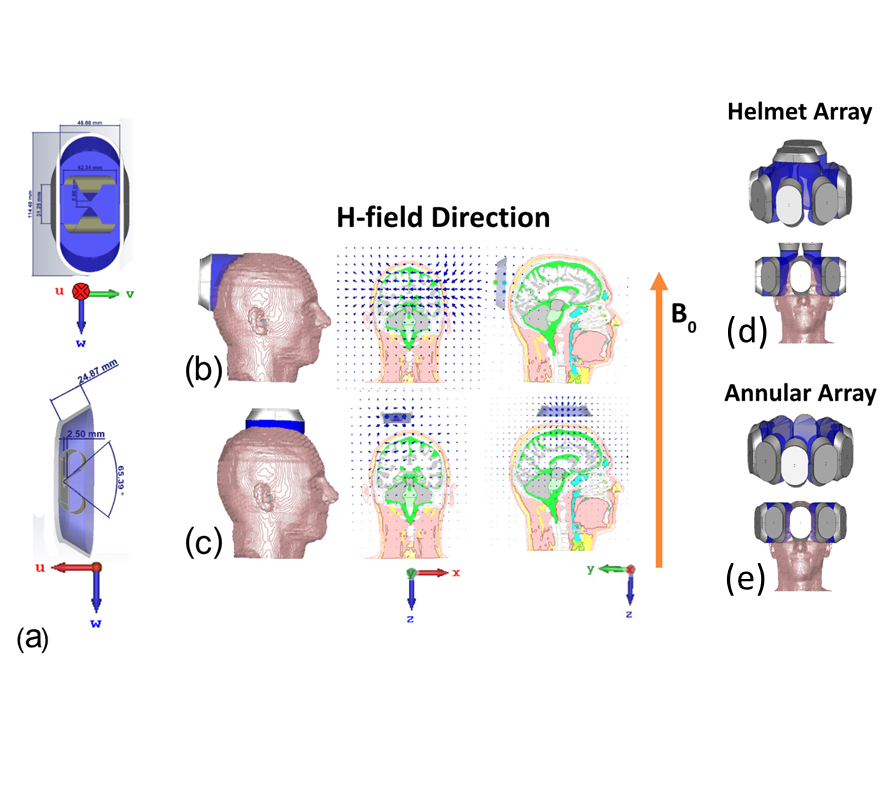
Fig. 2: a) Schematic of a bbSGBT building block in a UWV coordinate system frame. (b) H-field induced by a bbSGBT antenna with the long axis being aligned along the superior-inferior direction (y-axis); (c) H-field induced by a bbSGBT antenna placed on top of Duke with the long axis aligned along the y or the x-direction; RF-applicator configurations: d) helmet array (HA), and e) annular array (AA). Each array includes 10 bbSGBT Tx elements for transmission.
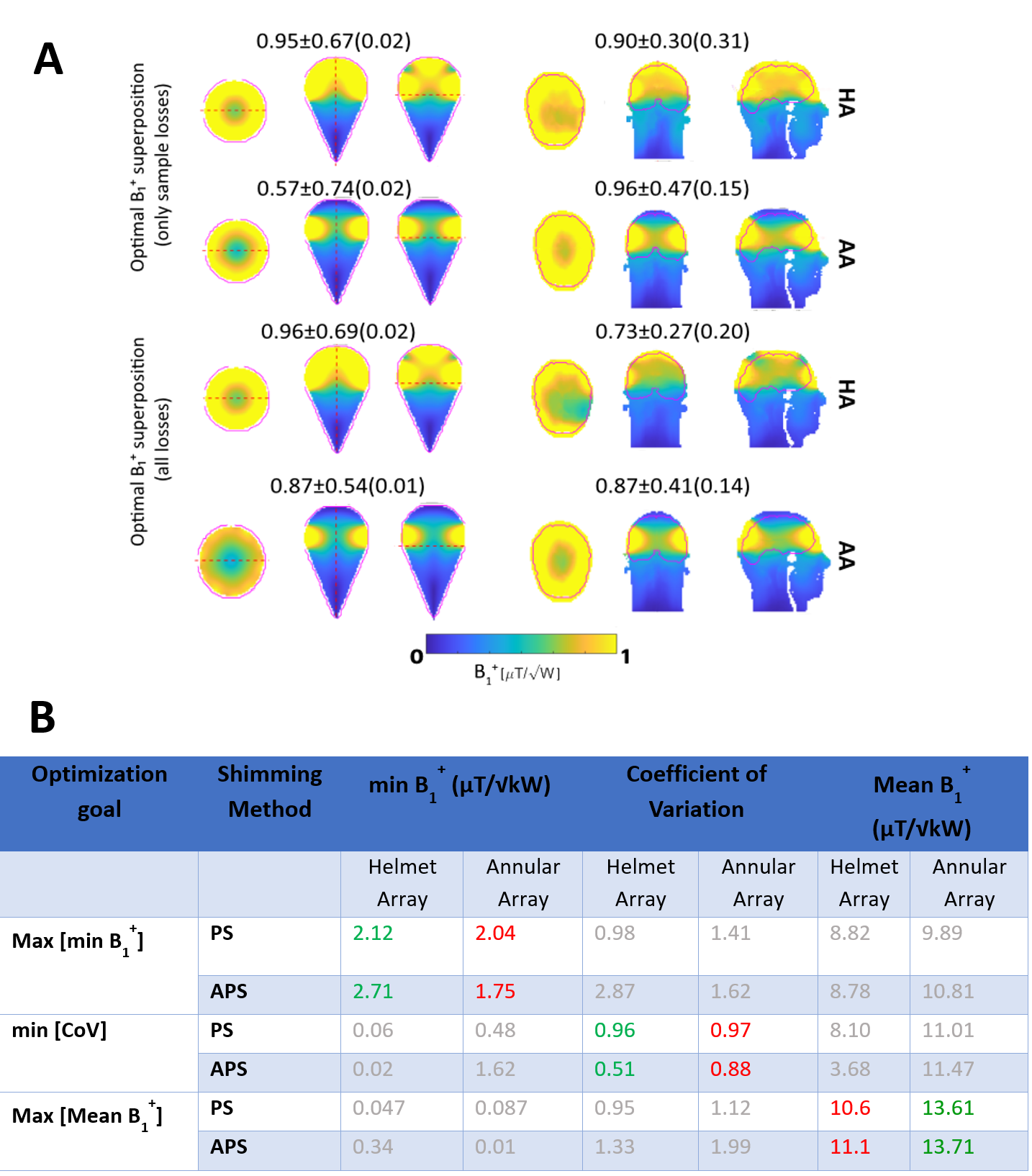
Fig. 3: A)Simulated B1+ for axial, coronal, and sagittal views obtained for the phantom (left) and the human head voxel model(right) (ideal model (IM), realistic model(RM)). Annotations indicate mean±SD(minimum) B1+ for the HA and AA RF applicator configurations. The ROI is depicted in red. B)The table is the summary of the B1+ metrics across the entire 3D brain of the human head voxel model (Duke) using phase-only shimming (PS) and amplitude and phase shimming (APS). Green and red numbers highlight the results obtained for each optimization goal outlined in the very left column.
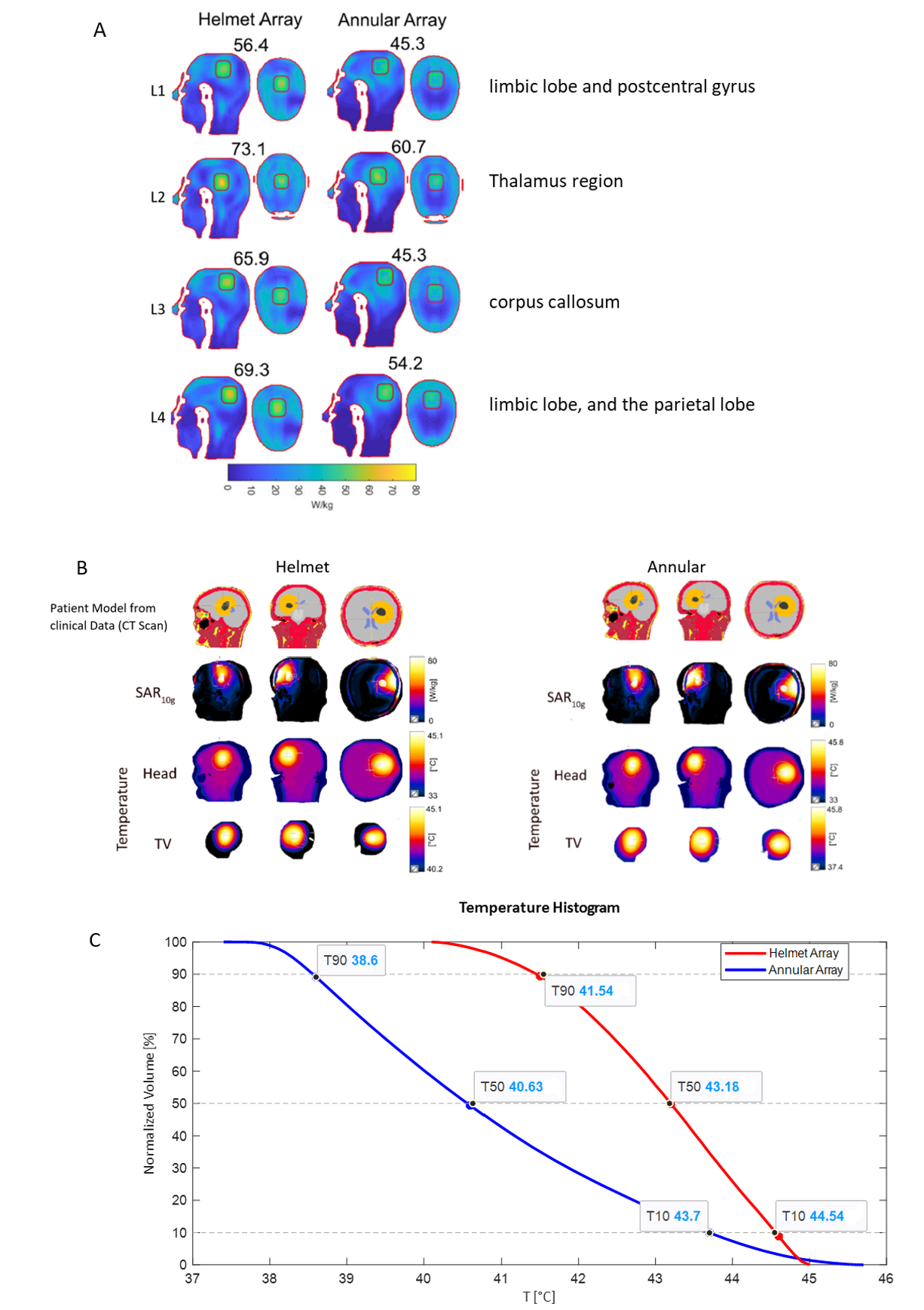
Fig. 4: A) SAR10g maps obtained for the HA and the AA for four TR3 locations placed in the human head voxel model Duke. MTS inside the TR is annotated. B) Clinical data from a patient model imported in sim4life (first row). By applying the sim4life optimization algorithm, SAR10g (second row), and temperature distribution inside the whole head (third row) and for the clinical TV (fourth row) of both AA and HA are illustrated. C) The cumulative normalized volume covered by different temperatures inside the TV to evaluate T10, T50, and T90 for the applicator.
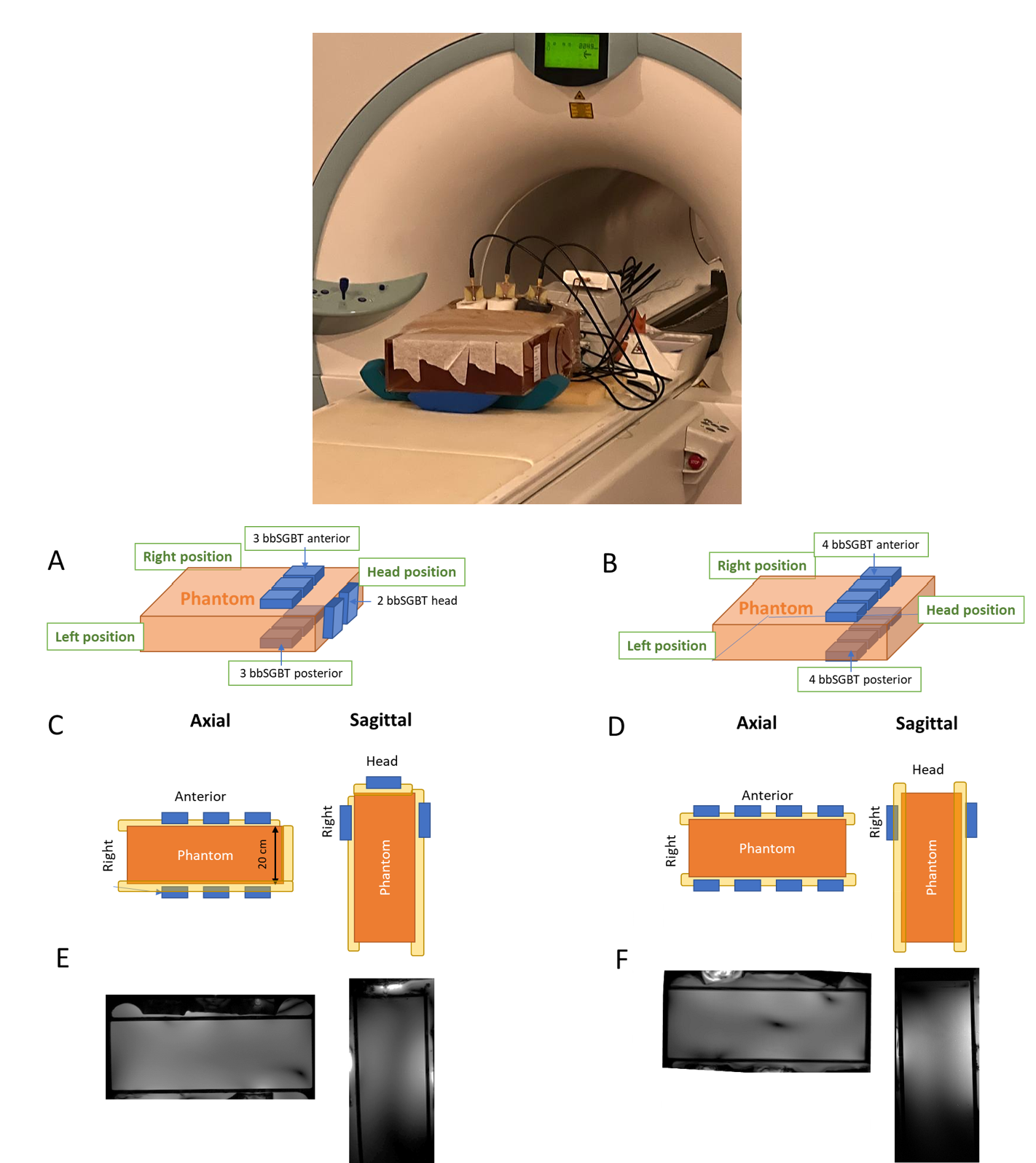
Fig. 5: Experimental setup for 8 channel bbSGBT arrays (top) with A) 3 anterior and 3 posterior and 2 perpendicular building blocks in head position and B) 4 anterior and 4 posterior building blocks. C,D) Axial and sagittal views of both setups. E,F) Axial and sagittal views obtained from FLASH MRI at 7T for both array configurations using the GUFI phantom. The dome-sphaped array provides improved coverage and depth penetration versus the reference annular array.