1217
Computer-assisted surgical modification of lead trajectory can substantially reduce RF heating of epicardial leads in children during 1.5T MRI1Biomedical Engineering, Northwestern University, Evanston, IL, United States, 2Radiology, Northwestern University, Chicago, IL, United States, 3Division of Cardiology, Ann and Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States, 4Division of Cardiovascular-Thoracic Surgery, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States, 5A. A. Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Boston, MA, United States
Synopsis
Keywords: Safety, Safety, epicardial leads;implants
Motivation: Once epicardial CIEDs are implanted in pediatric patients, they pose a relative contraindication for MRI scans due to the increased risk of RF heating.
Goal(s): Enhance MRI safety by reducing RF heating through surgical modification of the lead configuration.
Approach: Mathematical models of the CIED with different lead configurations were developed and validated using the transfer function approach. Low heating trajectories were identified and implemented in a patient.
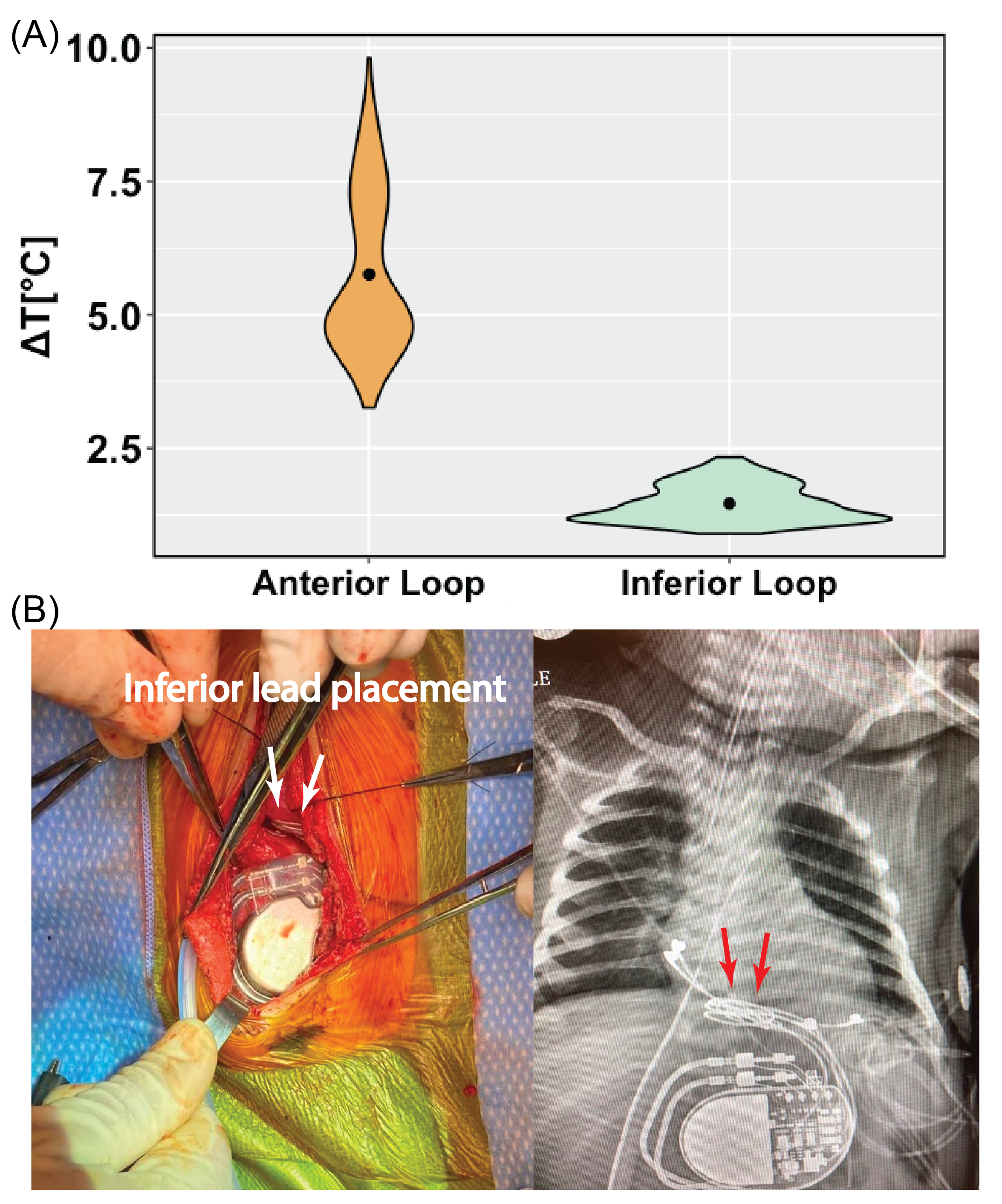
Results: Placing the excess lead length on the heart’s inferior surface resulted in an average 4-fold reduction in RF heating compared to anterior placement.
Impact: Implementing physics-based surgical modifications to the trajectory of epicardial leads can consistently and significantly reduce RF heating in children undergoing MRI at 1.5T.
Introduction
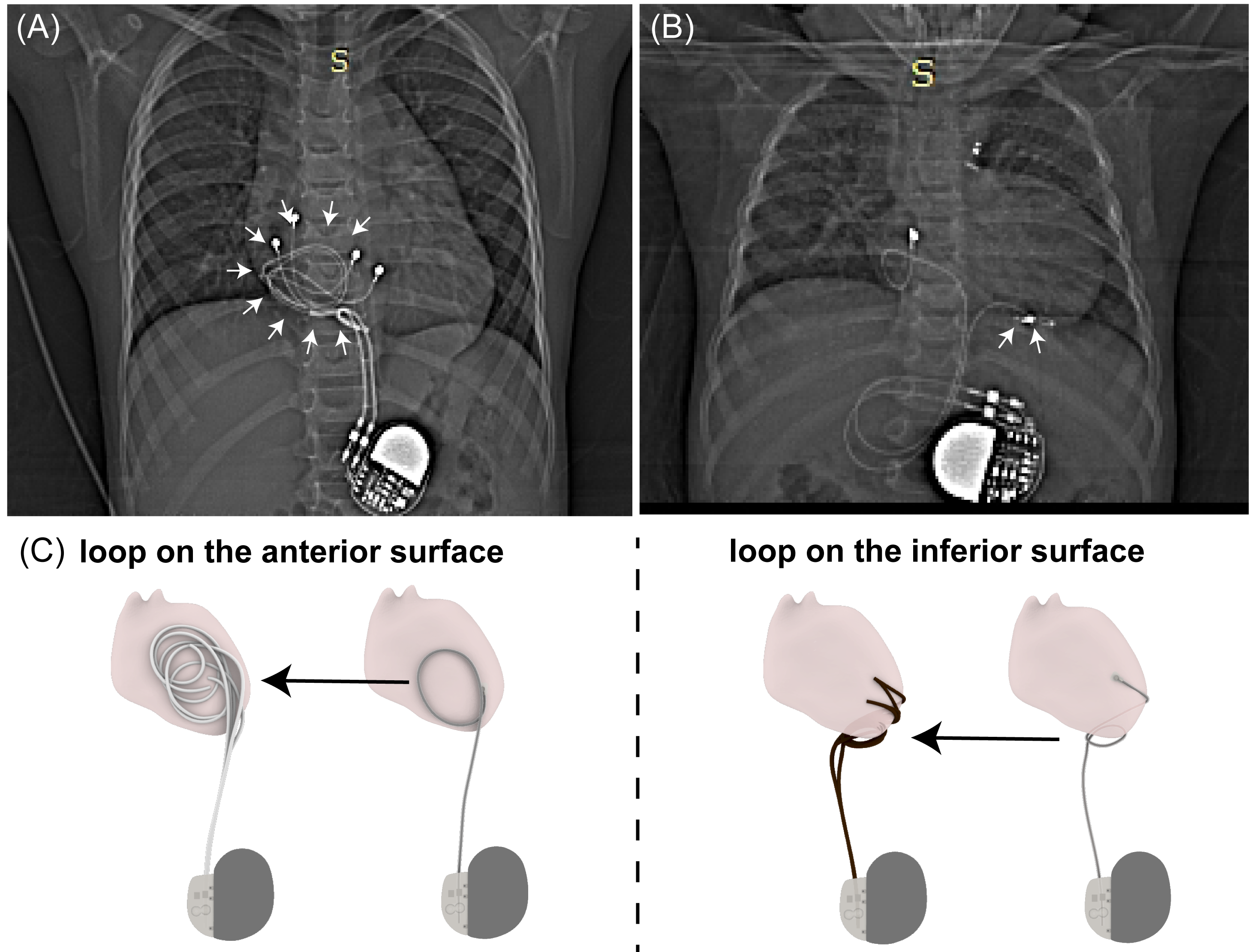
Congenital heart defects (CHDs) are the most common birth defects in the U.S., impacting 1% of newborns. Infants and children with CHDs often require cardiac implantable electronic devices (CIEDs), which traditionally involve epicardial leads that complicate MRI access due to RF heating risks.1-3 Specifically, substantial RF heating (>12) has been reported around tips of 25-cm epicardial leads in pediatric phantoms,4 high enough to cause necrosis in muscle after a 10-minute scan.5 Recent advancements drawn from studies in deep brain stimulation devices suggest that altering lead trajectory may substantially reduce RF heating.6 Here, we demonstrate that surgical modification of epicardial lead trajectories can substantially reduce RF heating in children during MRI at 1.5 T. Specifically, we show that coiling the excess length of a 25-cm epicardial lead and placing it on the inferior surface of the heart can reduce RF heating fourfold compared to the common practice of anterior loop placement (refer to Figure 1). The result was persistent across different tissue properties and for both head-first and feet-first patient positions. Proposed modifications could be easily adopted in the operating room, resulting in a twelvefold reduction in RF heating at the tip of an epicardial lead implanted in a 10-day-old infant.Methods:
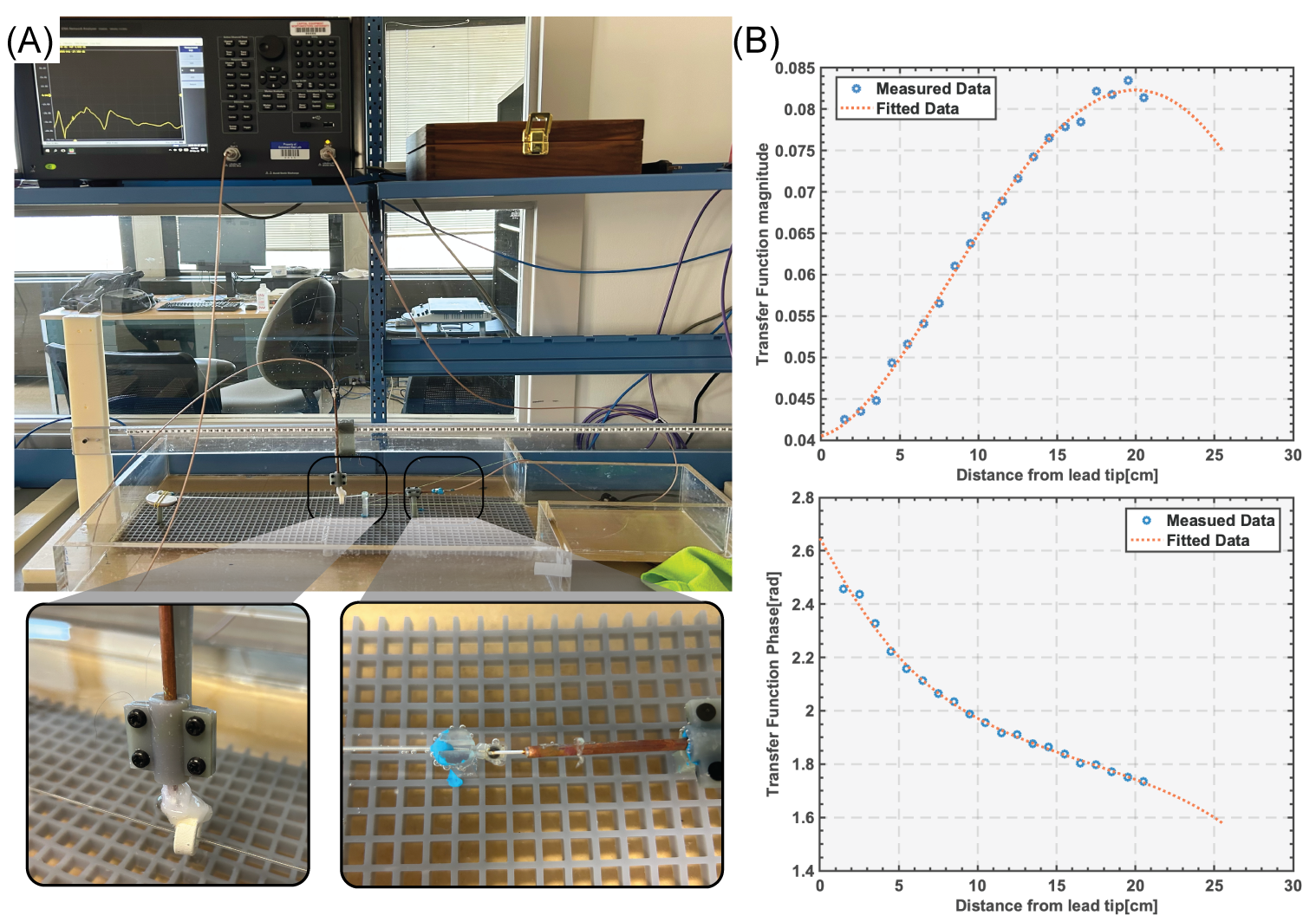
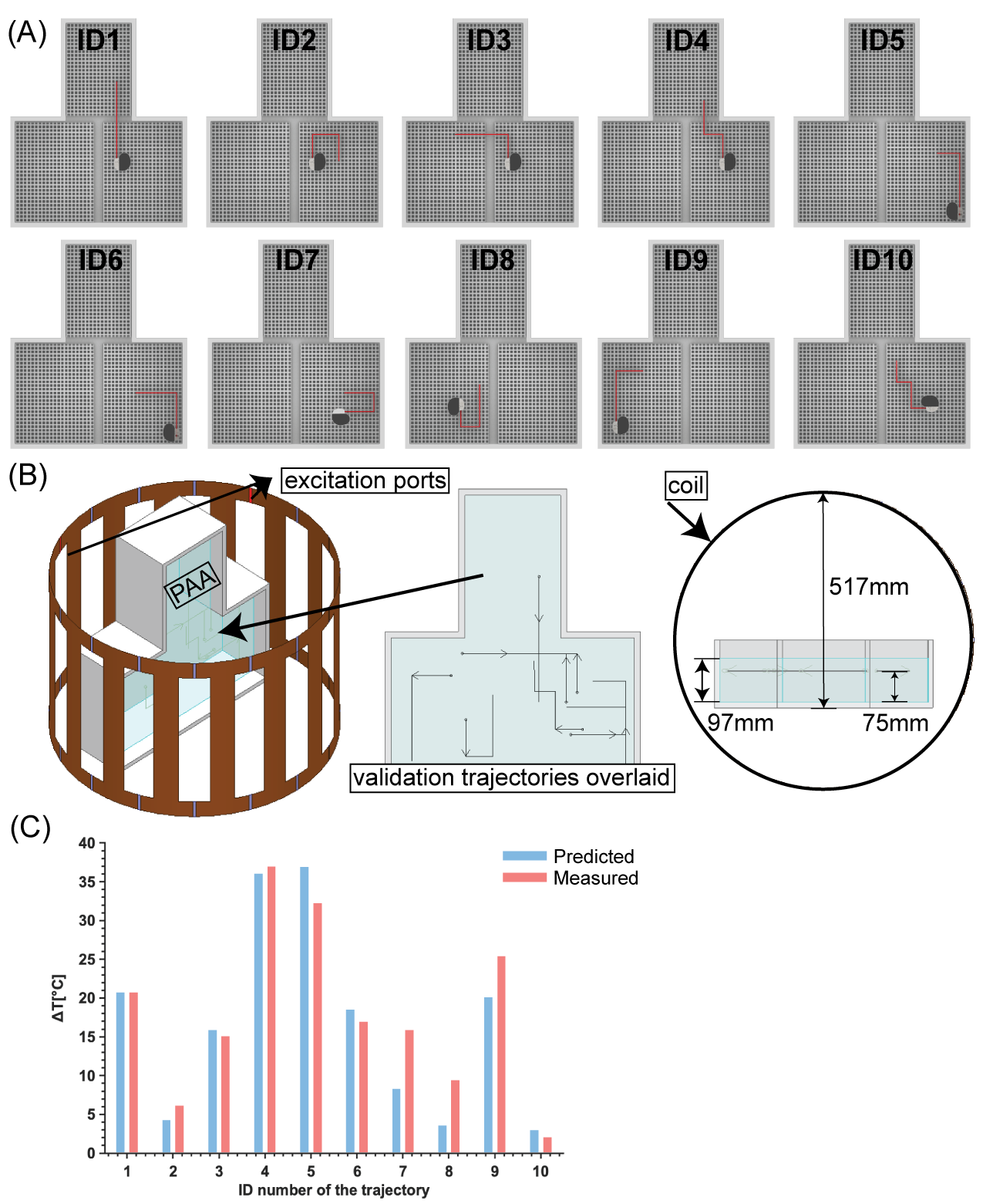
Construction and validation of the CIED model: We measured and validated the transfer function (TF) of a complete epicardial pacing system, which consisted of a Medtronic CapSure® EPI 4965 25-cm lead connected to a Medtronic Azure™ XT DR MRI SureScan pulse generator. The TF was measured with a two-port Vector Network Analyzer (VNA) (VNA 5063, Keysight Technologies, California, USA) in conjunction with a homemade receiving probe and a transmitting probe, following the reciprocal method.7 The specifics of the measurement setup were similar to those described in previous studies8,9.The TF was calibrated and validated by placing the lead along 10 orthogonal trajectories (Figure 3) and subjecting the system to 261 seconds of RF exposure in a 1.5 T Siemens AERA scanner using a T1-TSE sequence while recording the temperature increase (ΔT) near the lead tip. The measured ΔT along an arbitrary trajectory was used to calculate the calibration factor C as follows: $$C=\frac{\Delta T_{measured}}{{\lvert\int_{0}^{l}{TF(x)\cdot E_{tan}(x)dx\rvert}}^2}$$
The remaining nine trajectories were used for validation, comparing the measured temperature measured with the TF-predicted ∆T (Figure 3C). $$\Delta T_{predicted} = C{\lvert\int_{0}^{l}{TF(x)\cdot E_{tan}(x)dx\rvert}^2}$$
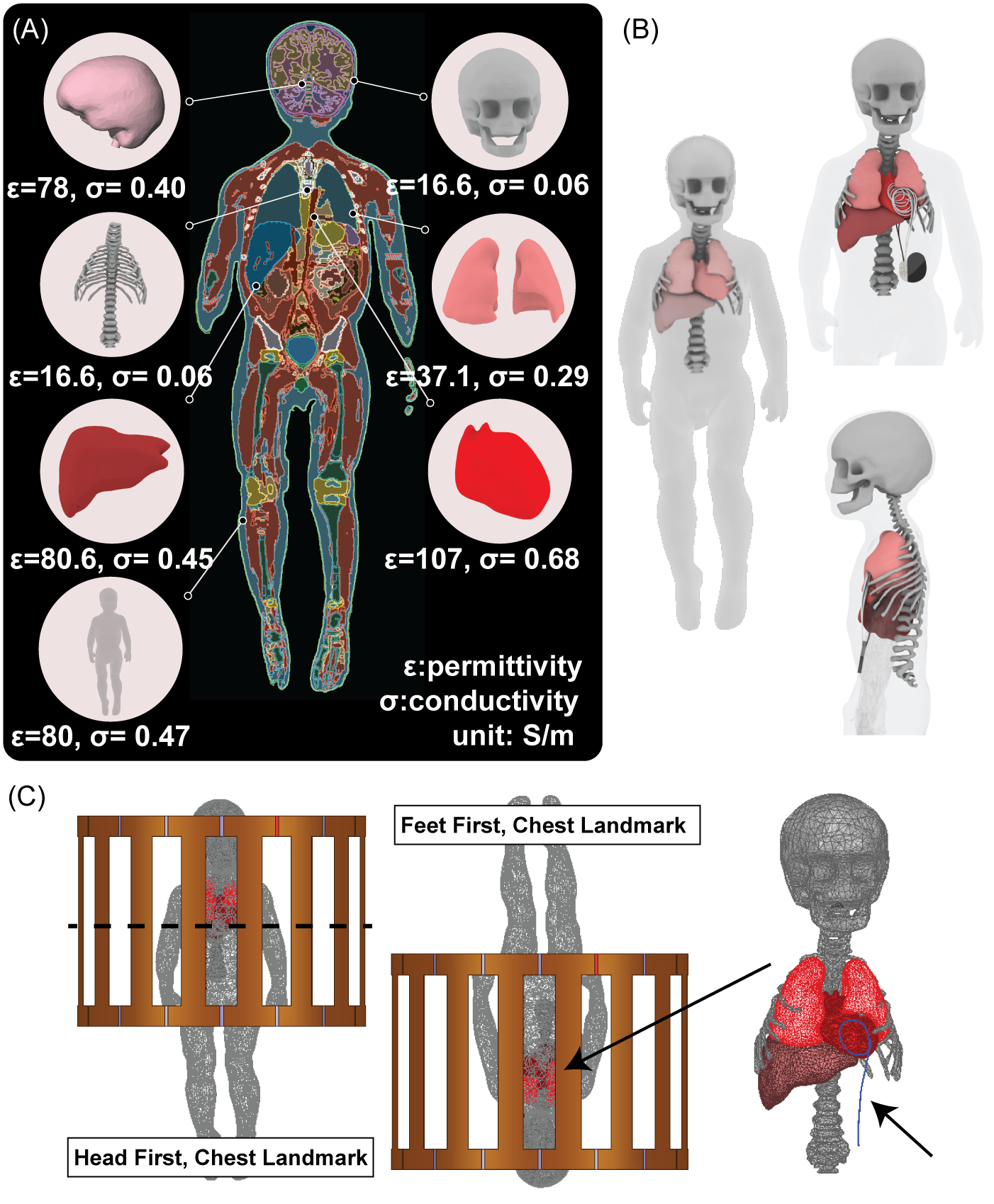
Simulations in realistic body models: Once the TF was validated, electromagnetic simulations were performed to predict the RF heating at the tip of the lead when the device was positioned in realistic pediatric body models. Models consisted of seven major tissues segmented from MR images of a 29-month-old child, each assigned to twelve distinct conductivity and permittivity values to account for the variability among the population (Figure 4). Each body model was positioned within the MRI coil with the heart at the isocenter, in both head-first and feet-first orientations. A total of 336 ΔT values were assessed, comparing RF heating of epicardial leads looped on the anterior surface of the heart (N=168) with those looped on the inferior surface (N=168).
Surgical implementation: The trajectory with the lower RF heating was identified and implemented in a 10-day-old 3.8 kg infant. The implantation was accomplished with an inferior limited medial sternotomy, rather than a full midline sternotomy, and the pulse generator was placed in a bilateral sub-rectus position (Figure 5). Postoperative X-ray images were used to replicate the device position in a phantom and assess RF heating.
Results:
The comparison between measured and predicted ΔT demonstrated a very good agreement between TF predictions and measured temperatures, with a 95% confidence interval calculated to be [1.4℃-4.5℃] (Figure 3).For CIED in realistic body models, the mean ± standard deviation of RF heating was 5.76±1.50°C for trajectories with a loop on the anterior heart surface vs. 1.46±0.35°C for trajectories with a loop on the inferior heart surface (averaged over both patient orientations). An unpaired two-sample Mann-Whitney Wilcoxon test revealed a significant difference in median RF heating between anterior and inferior trajectory groups, with the former showing higher heating (P<2.2e-16).
The surgical implementation of the low-heating trajectory was completed without complications and resulted in a 12-fold lower RF heating.
Discussion and Conclusion:
Computer-assisted surgical modification of epicardial lead trajectories can significantly reduce MRI-induced RF heating in children undergoing MRI at 1.5T. These techniques can be easily adopted in the operating room, leading to meaningful enhancement in MRI safety margins.Acknowledgements
This work was supported by NIH grant R01EB034377.References
1. Horenstein MS, Hakimi M, Walters H, 3rd, Karpawich PP. Chronic performance of steroid-eluting epicardial leads in a growing pediatric population: a 10-year comparison. Pacing Clin Electrophysiol. Jul 2003;26(7 Pt 1):1467-71. doi:10.1046/j.1460-9592.2003.t01-1-00212.x
2. Paech C, Kostelka M, Dähnert I, Flosdorff P, Riede FT, Gebauer RA. Performance of steroid eluting bipolar epicardial leads in pediatric and congenital heart disease patients: 15 years of single center experience. Journal of Cardiothoracic Surgery. 2014/05/12 2014;9(1):84. doi:10.1186/1749-8090-9-84
3. Noiseux N, Khairy P, Fournier A, Vobecky SJ. Thirty years of experience with epicardial pacing in children. Cardiology in the Young. 2004;14(5):512-519. doi:10.1017/S1047951104005086
4. Jiang F, Henry KR, Bhusal B, et al. Age Matters: A Comparative Study of RF Heating of Epicardial and Endocardial Electronic Devices in Pediatric and Adult Phantoms during Cardiothoracic MRI. Diagnostics. 2023;13(17):2847.
5. Van Rhoon GC, Samaras T, Yarmolenko PS, Dewhirst MW, Neufeld E, Kuster N. CEM43° C thermal dose thresholds: a potential guide for magnetic resonance radiofrequency exposure levels? European radiology. 2013;23(8):2215-2227.
6. Vu J, Bhusal B, Rosenow J, Pilitsis J, Golestanirad L. Modifying surgical implantation of deep brain stimulation leads significantly reduces RF-induced heating during 3 T MRI. 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC). 2021:4978-4981.
7. Feng S, Qiang R, Kainz W, Chen J. A Technique to Evaluate MRI-Induced Electric Fields at the Ends of Practical Implanted Lead. IEEE Transactions on Microwave Theory and Techniques. 2015;63(1):305-313. doi:10.1109/TMTT.2014.2376523
8. Missoffe A, Aissani S. Experimental setup for transfer function measurement to assess RF heating of medical leads in MRI: Validation in the case of a single wire. Magn Reson Med. Mar 2018;79(3):1766-1772. doi:10.1002/mrm.26773
9. Jiang F, Bhusal B, Nguyen B, et al. Modifying the trajectory of epicardial leads can substantially reduce MRI-induced RF heating in pediatric patients with a cardiac implantable electronic device at 1.5T. Magnetic Resonance in Medicine. 2023;90(6):2510-2523. doi:https://doi.org/10.1002/mrm.29776
Figures