1205
Applying adaptive convolution to brain data – Making use of transfer learning1Medical Physics Group, University Clinic and Outpatient Clinic for Radiology, University Hospital Halle (Saale), Halle (Saale), Germany, 2Halle MR Imaging Core Facility, Medical Faculty, Martin-Luther-University Halle-Wittenberg, Halle (Saale), Germany
Synopsis
Keywords: Analysis/Processing, Quantitative Susceptibility mapping
Motivation: Deep learning approaches for QSM-based dipole inversion lack generalizability towards acquisition parameters.
Goal(s): Our aim was to address data scarcity by integrating known information in the network model and investigate the feasibility of transfer learning.
Approach: The acquisition parameters (voxel size, FOV orientation) were integrated with manifold learning. The models were pre-trained on large-scale synthetic data sets and fine-tuned on in-vivo brain data in a second step.
Results: The use of manifold learning increased generalizability, while transfer learning substantially improved the quality of computed susceptibility maps.
Impact: While this study demonstrates the feasibility of cross-domain knowledge transfer in deep learning approaches for QSM, it also points to the potential of fine-tuning network parameters to scanner-specific data in general, boosting the performance of neural networks therewith.
Introduction
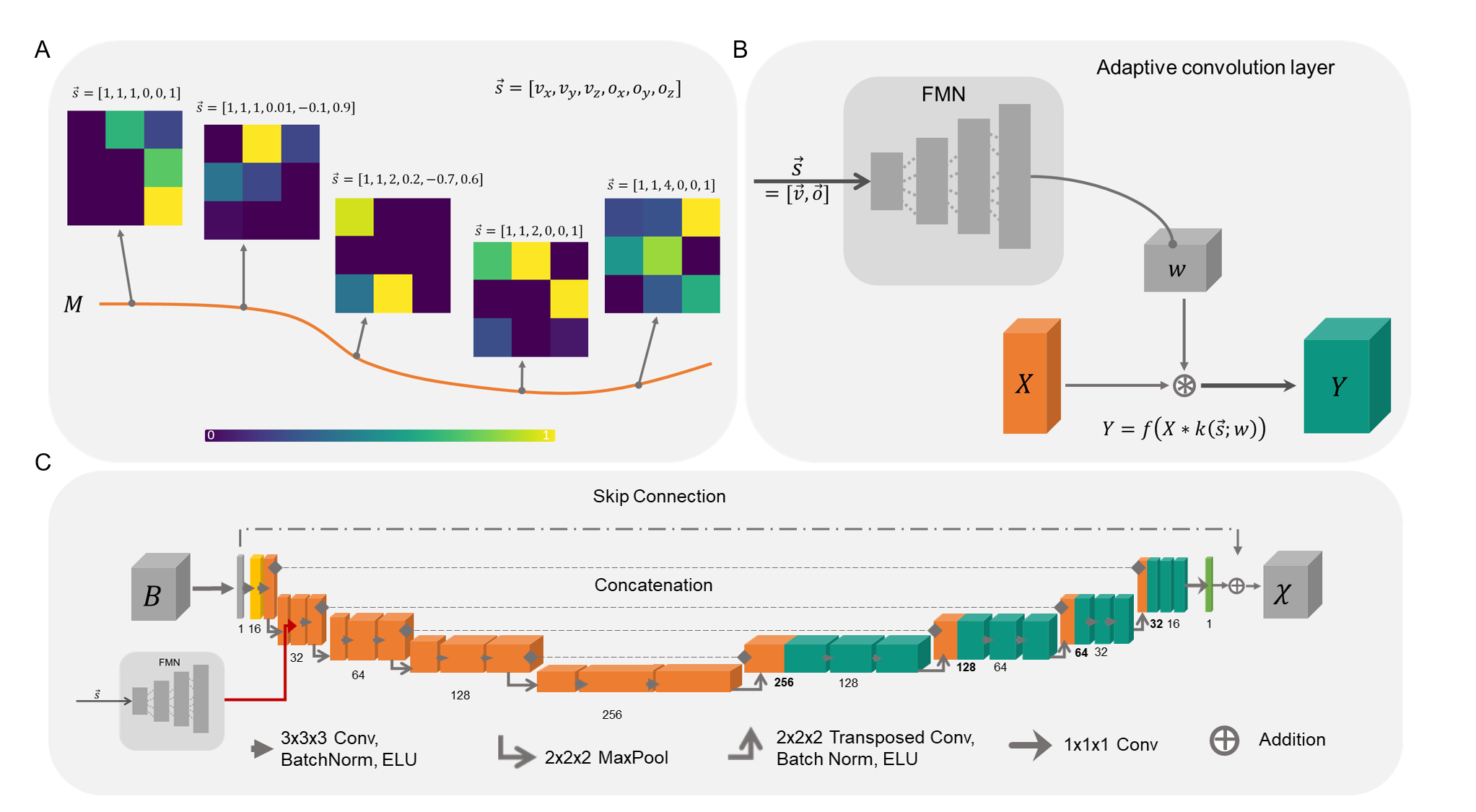
Quantitative susceptibility mapping (QSM), a post-processing technique used to compute the magnetic susceptibility distribution from the local magnetic field, increasingly relies on deep learning (DL) approaches. However, DL in medical imaging faces the challenge of data scarcity as well as the lack of large-scale and comprehensive training data, to learn internal representations that lead to invariance against changes in data. For QSM, the choice of imaging parameters (e.g., voxel size, FOV-orientation) in gradient-echo MRI substantially affect the local magnetic field representation and field direction in the acquired volume. It has been shown with the approach of adaptive convolution (AC)1 that these known parameters can be used as a-priori information and directly incorporated in the DL model to solve the ill-posed field-to-susceptibility inversion, outperforming conventional DL approaches. In short, AC learns the mapping between the additional presented information (imaging parameters) and the changes in the local magnetic field associated with this varying information (Fig. 1A) and subsequently selects the optimal set of convolution weights (Fig. 1B). In this contribution, we demonstrate the application of AC to brain data and assess the feasibility of a transfer learning approach for QSM-based dipole inversion for the first time.Methods
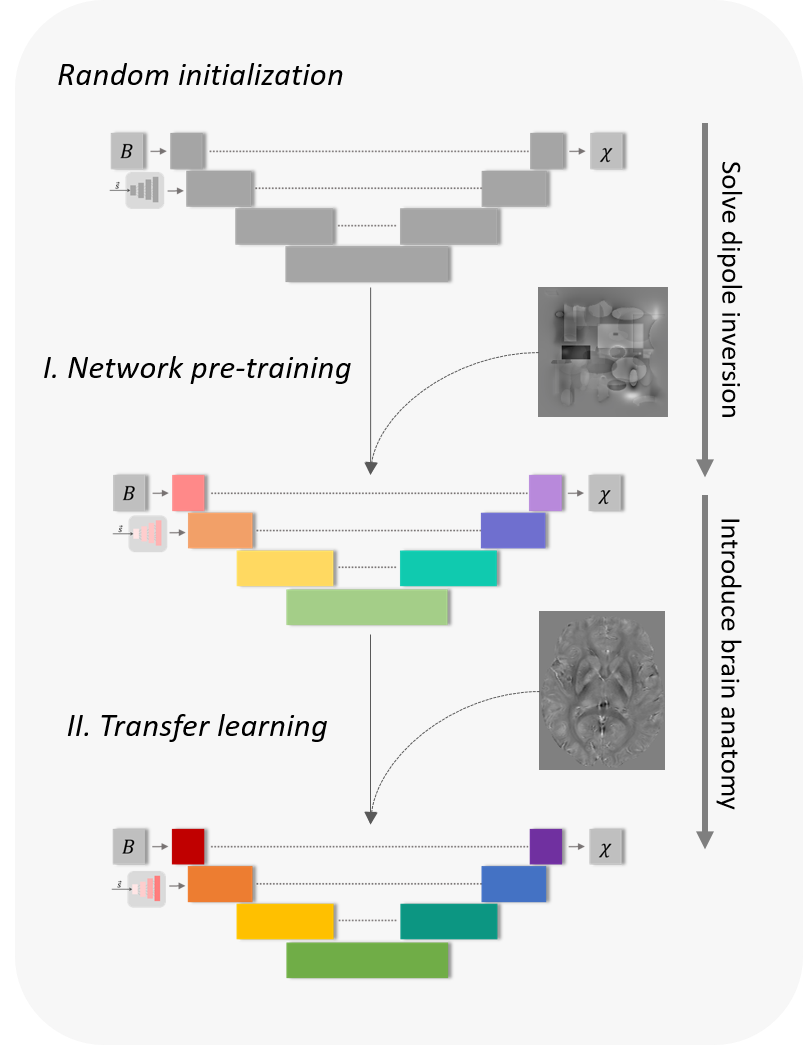
The adaptive model1 with a modified 3D U-Net2 backbone (Fig. 1C), directly including a-priori information about voxel-size and field-of-view (FOV) orientation via an additional array, was pre-trained on purely synthetic data sets for 500 epochs. The network was five layers deep with 16 initial channels and ELU activation function3,4. Data augmentation was performed regarding image rotation, flipping, scaling of susceptibilities and noise corruption. Transfer learning (TL) was performed thereafter, to tailor the network models specifically to brain data (Fig. 2). The training data for TL was composed of 109 in vivo brain data sets acquired with varying FOV and head orientations at 3T5 and 7T6. Patch-based training was performed on a total of 13080 patches. TL was performed for 30 epochs. All models were trained with the Adam-W optimizer7. A cosine annealing learning rate schedule with warm restarts was used for network pre-training8. For the TL, the parameters of the adaptive layer remained fixed, the learning rate for all parameters in the decoding branch of the model was set to η=0.001 and to η=0.00001 for all other parameters.Results
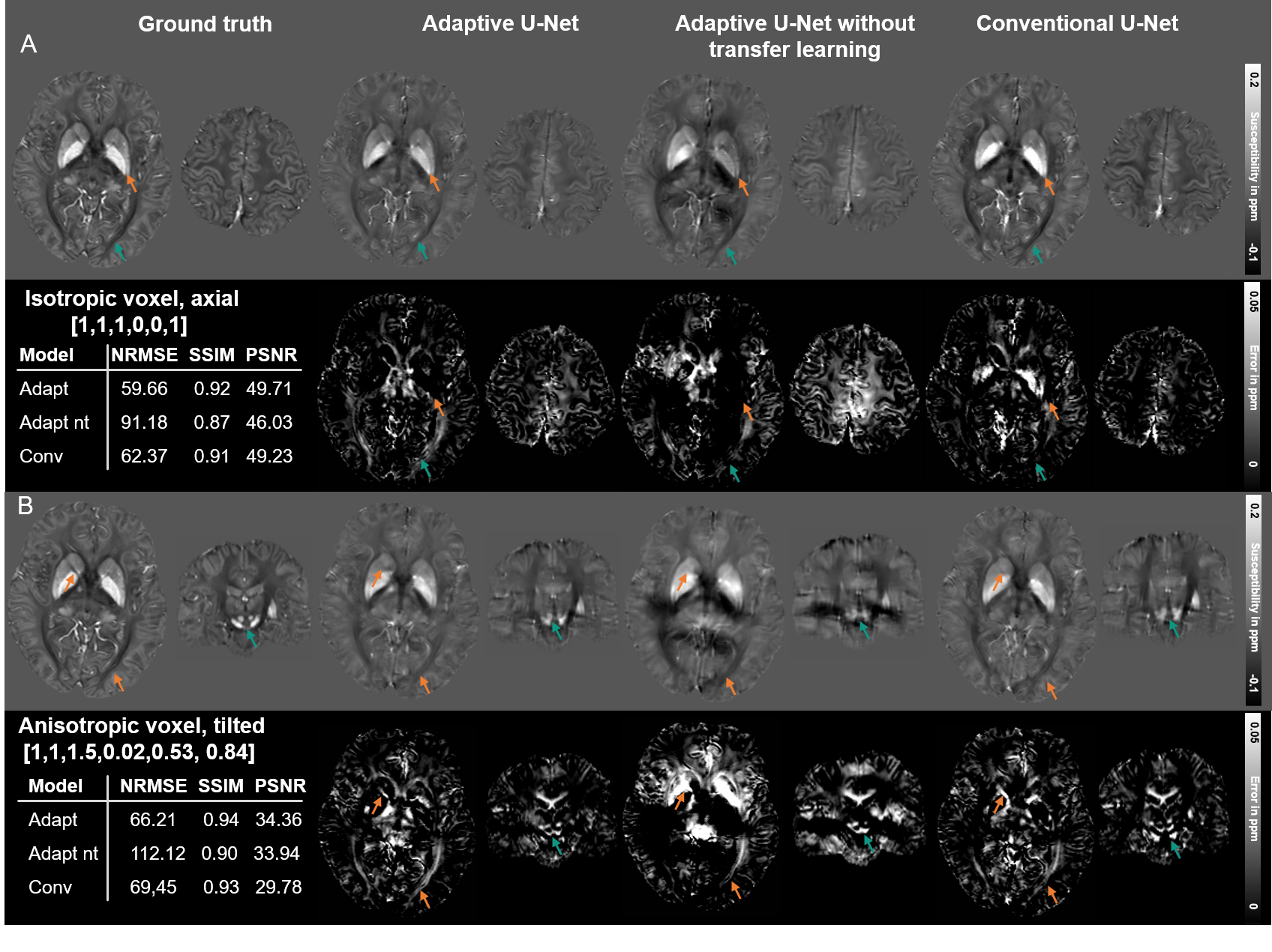
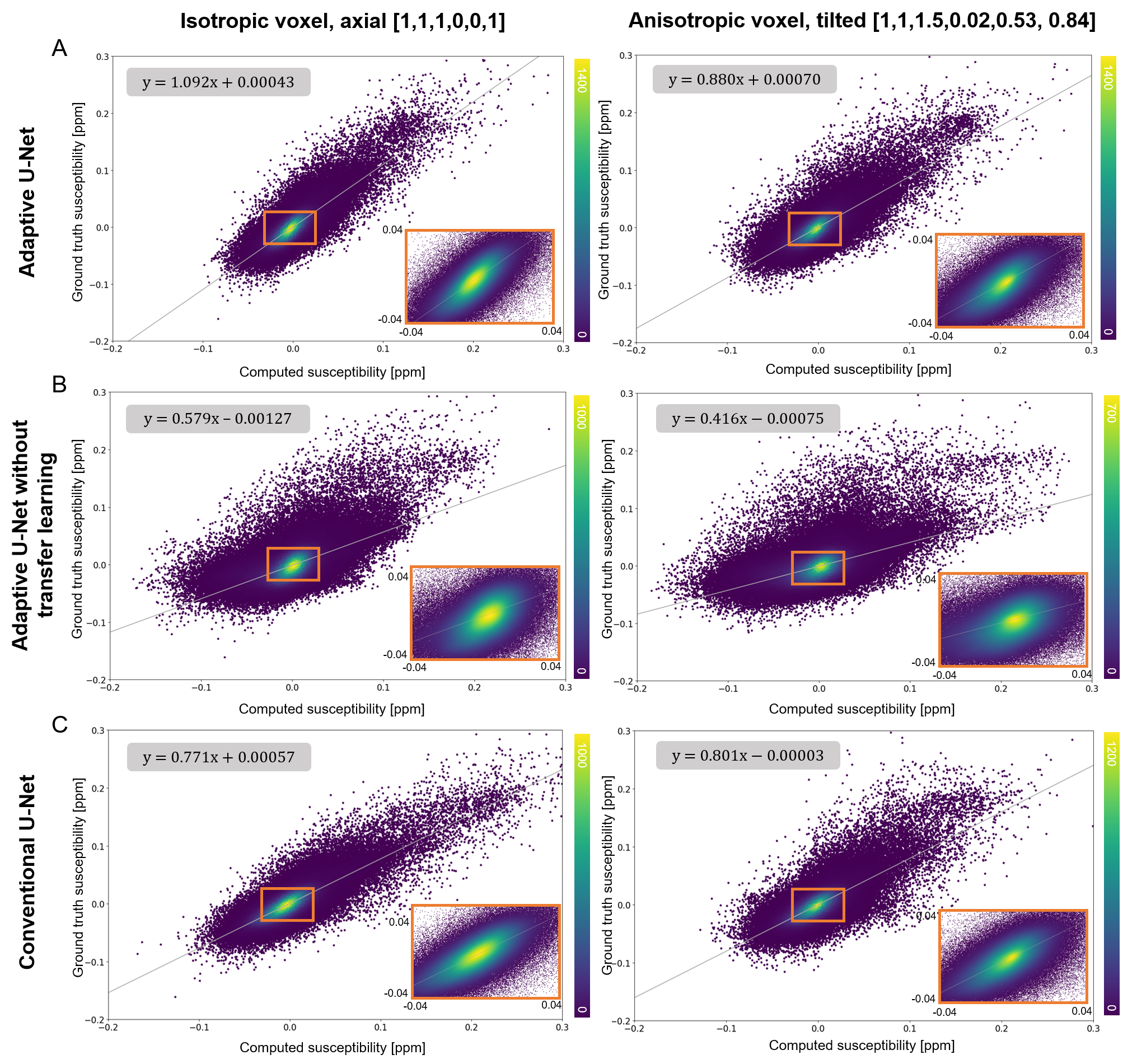
The susceptibility maps computed with the adaptive model with TL are the ones most similar to the ground truth, visually and in metrics (Fig. 3). Differences in the reconstructed maps are present in the globus pallidus (Fig. 3A, orange arrows) and in the optic radiation (Fig. 3A, turquoise arrows). As indicated by the difference maps, the adaptive U-Net with TL delineated the substantia nigra and subthalamic nuclei (Fig. 3B turquoise arrows) the clearest. The adaptive model without TL achieved the lowest metrics and showed the largest deviations to the COSMOS map. The scatter plots of 400k susceptibilities drawn across the whole brain (Fig. 4) from in vivo brain data (Fig. 3) revealed point clouds centered on a straight line for all models with respect to the COSMOS susceptibilities. The slopes of the fitting lines for the adaptive U-Net with TL deviated least from 1, indicating closest agreement between ground truth and computed susceptibilities.Discussion
The assessment on brain data revealed closest agreement between ground truth data and the adaptive model experiencing the proposed TL. In comparison to the adaptive model with TL, the conventional model showed greater deviations of reconstructed susceptibility values with respect to the COSMOS map, which is most likely due to non-optimal parameter optimization. The applied TL strategy to fine-tune the models’ network parameters towards brain data resulted in improved metrics and greater visual similarity to the ground truth map (Fig. 3), indicating an increased quality of reconstructed susceptibility maps, e.g. sharper delineation of anatomical structures. Our proposed TL approach for cross-domain knowledge transfer with pre-trained base models that solve the general problem of field-to-susceptibility inversion detached from anatomy, prevents the models from developing an anatomical bias. The specific anatomical knowledge is then introduced via TL, which enables fine-tuning of the base models to different body parts in possible further applications. Future work will focus on reducing the gap between simulated and real world data, e.g. including microstructural effects9 and the TL strategy itself.Conclusion
A priori information was successfully included into deep learning models via adaptive convolution for solving the ill-posed field-to-susceptibility problem. Additional transfer learning substantially improves the reconstruction outcomes on in vivo data by introducing specific anatomic priors to the base model.Acknowledgements
This project was supported by the European Regional Fund (ERDF - IP* 1b, ZS/2021/06/158189).References
1. Graf S, Küchler N, Wohlgemuth WA, Deistung A. Adaptive convolution for including a-priori information in deep learning models for quantitative susceptibility mapping. In: Proc. Intl. Soc. Mag. Reson. Med. 31; 2023.2. Ronneberger O, Fischer P, Brox T. U-Net: Convolutional Networks for Biomedical Image Segmentation; 2015.
3. Clevert D-A, Unterthiner T, Hochreiter S. Fast and Accurate Deep Network Learning by Exponential Linear Units (ELUs): arXiv. 2015. Available at: https://arxiv.org/pdf/1511.07289.
4. Graf S, Küchler N, Wohlgemuth WA, Deistung A. Comparison of activation functions for optimizing deep learning models solving QSM-based dipole inversion. In: Proc. Intl. Soc. Mag. Reson. Med. 31; 2023.
5. Shi Y, Feng R, Li Z, Zhuang J, Zhang Y, Wei H. Towards in vivo ground truth susceptibility for single-orientation deep learning QSM: A multi-orientation gradient-echo MRI dataset. NeuroImage. 2022;261:119522.
6. Deistung A, Schäfer A, Schweser F, Biedermann U, Turner R, Reichenbach JR. Toward in vivo histology: a comparison of quantitative susceptibility mapping (QSM) with magnitude-, phase-, and R2*-imaging at ultra-high magnetic field strength. NeuroImage. 2013;65:299-314.
7. Loshchilov I, Hutter F. Decoupled Weight Decay Regularization; 2017.
8. Loshchilov I, Hutter F. SGDR: Stochastic Gradient Descent with Warm Restarts; 2016.
9. Wharton S, Bowtell R. Effects of white matter microstructure on phase and susceptibility maps. Magnetic resonance in medicine. 2015;73(3):1258-1269.
Figures