1202
Healthy-to-Patients Domain-Adaptive Deep Learning for Time-Resolved Segmentation of Left Atrium in Short-Axis Cine MRI Images1Radiology, Northwestern University, Chicago, IL, United States, 2Preventive Medicine, Northwestern University, Chicago, IL, United States
Synopsis
Keywords: Analysis/Processing, Segmentation, Left Atrium, Mitral Valve Regurgitation, Domain Adaptation, Deep Learning
Motivation: Addressing challenges with current deep learning (DL) techniques that struggle with domain shifts.
Goal(s): To introduce a domain-adaptive technique that is able to segment the Left Atrium from MRI of patients employing model trained exclusively on healthy data.
Approach: Our approach involves training exclusively on healthy data and incorporating stochastic encoding of temporal composite variations as augmentations to encode the underlying space of plausible anatomical changes and dynamics. We tested on three challenging unseen patient daatsets.
Results: Our domain-adaptive approach showed significant improvement over the state-of-the-art LA segmentation model. Enabling LA segmentation of all time frames of the cardiac cycle.
Impact: The proposed domain-adaptive deep learning approach addresses a fundamental challenge of training deep learning models only on healthy control datasets while maintaining high performance on unseen patients' populations. This could potentially lead to solve performance issues for limited patients cohorts.
Purpose
Accurate Left Atrium (LA) segmentation from Short Axis (SAX) Cine MRI is vital for cardiac evaluation. However, current deep learning (DL) techniques struggle with domain shifts, where models trained on one patient group often fail when applied to another. Here, we introduce a novel DL approach focusing on domain adaptation. Unlike traditional confounded adaptation methods that treat mixed patient populations as a single domain, we address the true challenge of adapting from healthy to patient domains. Our approach involves training exclusively on healthy data and incorporating stochastic encoding of temporal composite variations as augmentations to encode the underlying space of plausible anatomical changes and dynamics. In addition to better generalizability, our approach allows LA segmentation from all time frames in the cardiac cycle as opposed to only 3-frames by previous methods [4, 5]. We evaluated our proposed approach on completely unseen patient data from three different challenging patient groups: Hypertrophic cardiomyopathy (HCM), Heart failure with reduced ejection fraction (HFrEF), and mitral valve regurgitation (MVR) patients, without training on any patient’s data.Methods
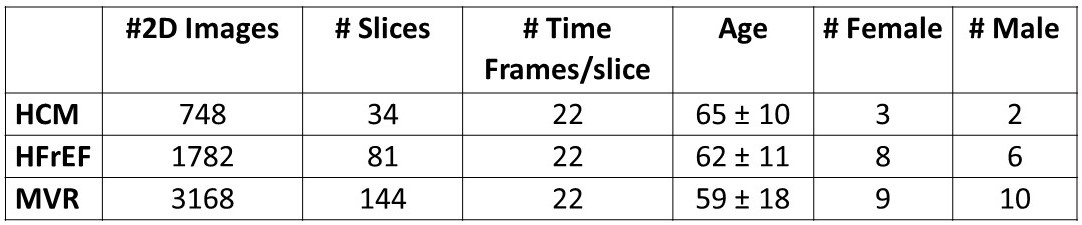
The study includes four datasets: 118 Healthy subjects, 5 HCM patients, 14 HFrEF patients, and 19 MVR patients (Table 1). All subjects underwent cardiac multi-slice cine short-axis SSFP MR imaging covering the left atrium. LA Segmentation was performed by experts over the entire cardiac cycle over all available LA slices.Training/Validation dataset: Only the healthy subjects’ dataset was used for training and validation (No patient data was used). We split the healthy subjects as 100 subjects for training (15150 images, 606 slices), and 18 for validation (2725 images, 109 slices, 25-time frames/slice).
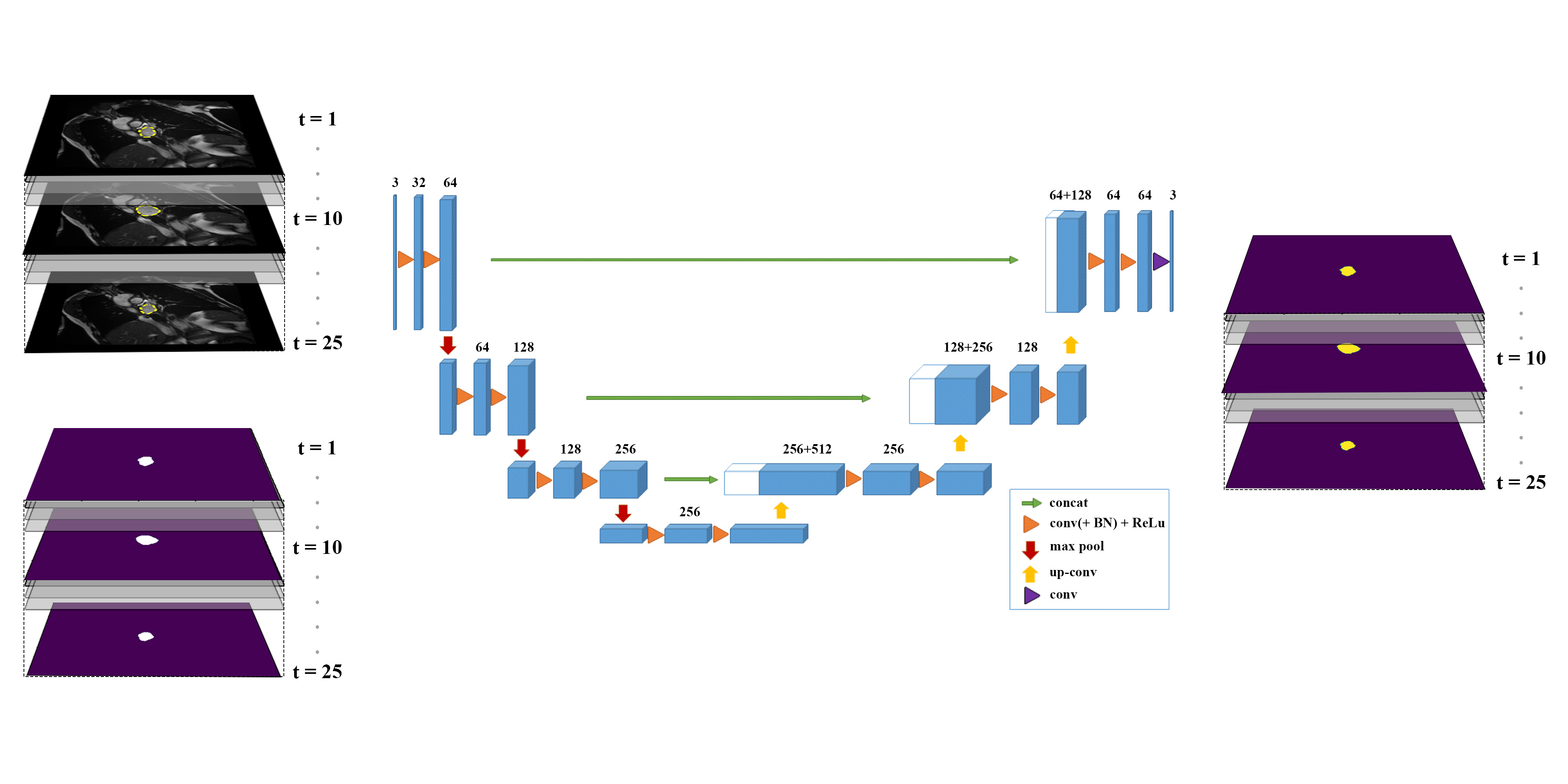
DL architecture and domain-adaptive augmentation: To enable domain adaptation, we employ a stochastic-based temporally constrained augmentation approach combined with 3D UNet architecture [1] (Fig. 1). Each input to the 3D U-net consists of a 2D+time volumetric data stack containing all 25 images of the cardiac cycle. For each 2D+time stack, we employ stochastic-based composite augmentation including rotation, flipping, sharpening, brightness adjustment, Gamma correction, cropping, and zooming. Random combinations of augmentations are chosen with a probability of (p=0.5) in each iteration. All augmentations are applied in 3D to each time-resolved LA stack in the temporal direction. This helps the model to learn a totally different augmented sample at every epoch, improving temporal realism in feature encoding and constraint augmentations to temporally plausible LA variations. We compared the performance of our domain-adaptive 3D U-Net approach to the state-of-the-art LA segmentation DL model which uses 2D U-Net with augmentations [4,5]. Previous DL-based LA segmentation literature focused on training and testing only on 3-time frames. However, for a fairer comparison to our proposed model, we trained and tested the existing literature model [4 ,5 ] on all time points to mitigate any possibility that our improvement is merely because we add more time points.
Testing datasets: We have tested our approach trained solely on healthy data in 3 diverse challenging patient datasets (Table 1), including: 1) HCM patients,2) HFrEF patients 3) MVR patients. No patient samples were included in our DL model training or validation.
Results
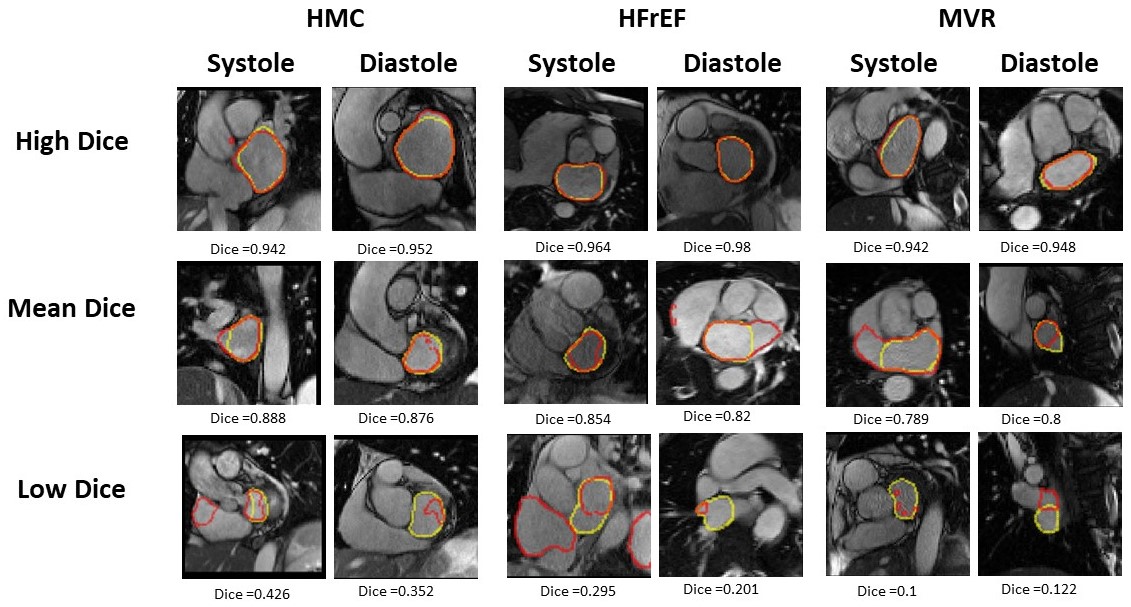
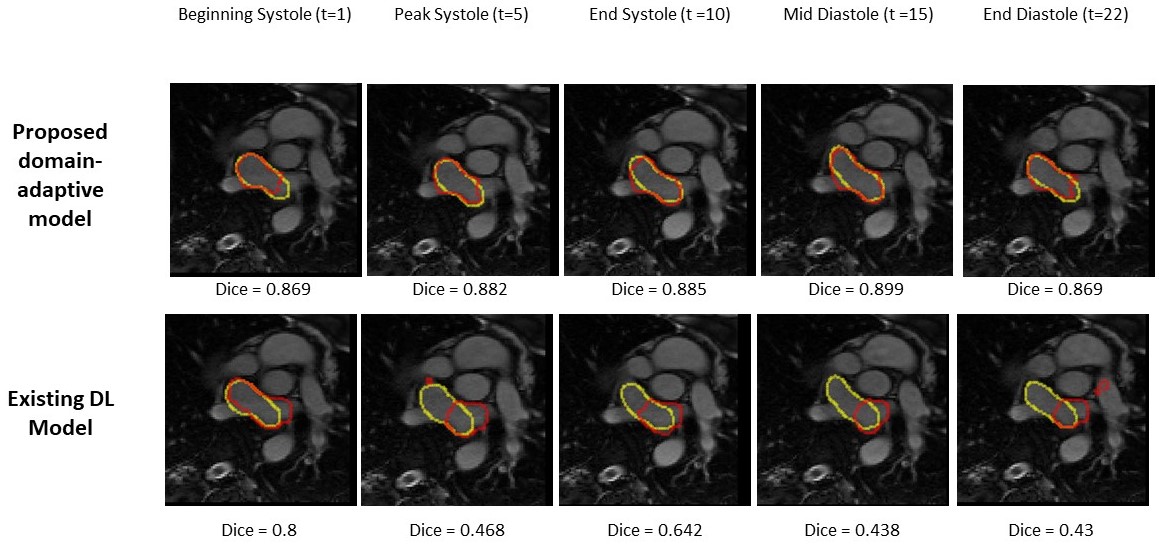
Our proposed volumetric domain-adaptive approach, trained only on healthy data, showed a strong LA segmentation performance in all three patient cohorts (Table 2). For HCM patients, our approach had a Dice score of 0.87±0.25, (Median=0.96). For HFrEF patients, our approach showed a Dice score = 0.783±0.33, (Median=0.93) and a Dice score = 0.798±0.317, (Median=0.946) for the HCM patients. Our domain-adaptive approach significantly outperformed existing DL model with an average dice increase of 9.5±34.4% for HMC, 4±35.3% for HFrEF and 2.7±35.9% for MVR (p<0.001) – see Figure 2. Figure 3 shows patient groups testing samples during mid-systole and mid-diastole, while Figure 4 compares our approach with an Existing 2D-UNet-based model across multiple time points.Discussion and conclusions
The results of this study demonstrate the strong performance of our innovative domain-adaptive healthy-to-patients LA segmentation approach. Our novel approach is based on training data exclusively on healthy data and tested it on three complex patient cohorts. We introduce stochastic-based temporal composite volumetric augmentations encoding the underlying space of plausible temporal anatomical LA variations that may occur in patients. Our domain-adaptive approach showed significant improvement over the state-of-the-art LA segmentation model, which also involves augmentations. Our approach enables LA segmentation of all time frames of the cardiac cycle (here 22 frames) versus only 3 frames in prior studies [4,5]. Our study highlights the potential of using healthy datasets to train versatile domain-adaptive models. Further studies are needed to evaluate the generalizability in multi-center and multi-vendor datasets.Acknowledgements
No acknowledgement found.References
[1] Çiçek, Özgün, et al. MICCAI Part II 19 (2016): 17-21.
[2] Ronneberger, O., et al. MICCAI Part III 18 (2015): 234-241.
[3] Zhang, Ling, et al. IEEE transactions on medical imaging 39.7 (2020): 2531-2540.
[4] Uslu, Fatmatülzehra, et al. IEEE transactions on medical imaging 41.2 (2021): 456-464.
[5] Uslu, Fatmatülzehra, et al. IEEE 18th International Symposium on Biomedical Imaging (ISBI) (2021): 766-769.
Figures