1182
Pre-surgical assessments of CSF flow and brain motion are indicative of improved cerebral dynamics following surgery in Chiari Malformation I1Emory University, Atlanta, GA, United States, 2Northeastern University, Boston, MA, United States
Synopsis
Keywords: Neurofluids, Neurofluids, Neurosurgery, Posterior Fossa Decompression, Chiari Malformation, DENSE, CSF Flow
Motivation: Chiari Malformation I (CM-I) is a condition characterized by cerebellar tonsil herniation, leading to reduced cerebrospinal fluid (CSF) flow and various neurological symptoms. Posterior fossa decompression (PFD) surgery can relieve symptoms, but surgical decision making is often unclear.
Goal(s): Tonsillar descent poorly correlates with symptoms and surgical outcomes. We seek to better characterize the cerebral dynamic effects of CM-I and PFD surgery.
Approach: Measure CSF flow using PCMR, and brain motion using DENSE, before and after PFD surgery.
Results: Surgery showed best improvement in patients with significantly restricted pre-surgical CSF flow or severely increased pre-surgical brain motion, regardless of amount of tonsillar descent.
Impact: Presurgical indicators of an individual’s likelihood of surgical improvement are critical in developing informed care plans. We find that direct measures of cerebral dynamics outperform standard measures of tonsillar decent at predicting improvement from posterior fossa decompression surgery in CM-I.
Introduction
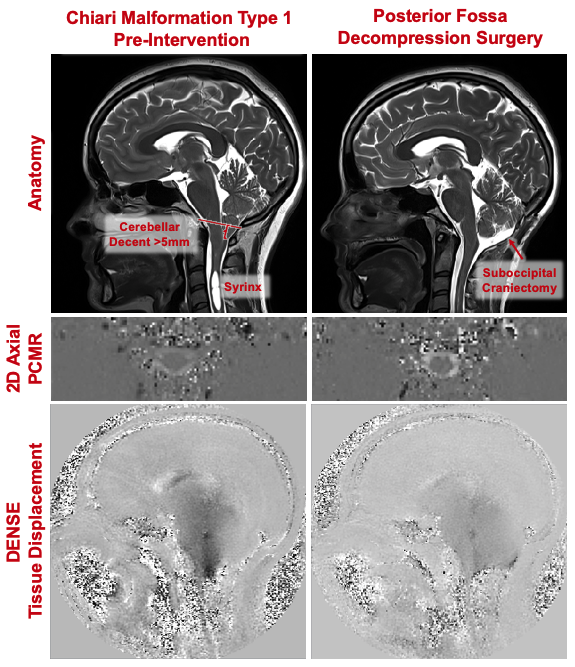
Chiari Malformation I (CM-I) is a condition characterized by cerebellar tonsil herniation of >5mm through the foramen magnum. CM-I causes a reduction of cerebrospinal fluid (CSF) flow[1] and an increase in cardiac-induced brain motion[2](Figure 1), and is associated with headaches, paresthesia, dysphagia, and sleep apnea[3,4]. In symptomatic cases, posterior fossa decompression (PFD) surgery is often performed, which involves removing bone to enlarge the foramen magnum and cervicomedullary junction and establish normal CSF flow[5]. Successful PFDs improves symptoms in ~70-80% of patients[6]. However, the surgery involves risk, and identifying which candidates will benefit from surgery is important. The degree of tonsillar herniation does not correlate with symptom severity or to surgical outcomes[7,8]. Therefore, we seek to use advanced neuroimaging methods to quantify how PFD affects cerebral dynamics. We hypothesize that CSF flow and brain motion will give better insights for which patients will have the greatest likelihood of cerebral dynamic improvements from surgery.Methods
We imaged 89 patients (18-71yrs, mean=37.2yrs; M/F=18/82) with a clinical diagnosis of CM-I on a Siemens 3T PrismaFit. Of these patients, 49%(44 patients) underwent PFD and participated in a three-month follow-up MRI.To measure CSF flow, we collected a retrospectively ECG-gated, 2D-axial PCMR scan at 1.2x1.2x5mm resolution, VENC=5cm/s, with 25 images per cardiac cycle. CSF was manually segmented, and pixel-wise velocity was integrated to output flow at each time-point. Stroke volume was defined as the average of the absolute value of the cranial and caudal flow.
To measure brain pulsatile motion, we used displacement-encoding with simulated-echoes (DENSE). Images were acquired in the sagittal plane at the midline using a two-dimensional spiral cine sequence with peripherally pulse unit-gating. 13–29 frames were acquired over the cardiac cycle depending on heart rate. Image resolution was 0.9x0.9x8.0mm[9]. Displacement was calculated pixel-wise over the cardiac cycle from the phase images.
To measure tonsillar descent, we collected a sagittal T2-weighted image. Data was analyzed using both unpaired t-tests, with the pre-surgical group including all patients, and pairwise t-test with just patients who underwent surgery. Pearson correlations were used for continuous variables.
Results
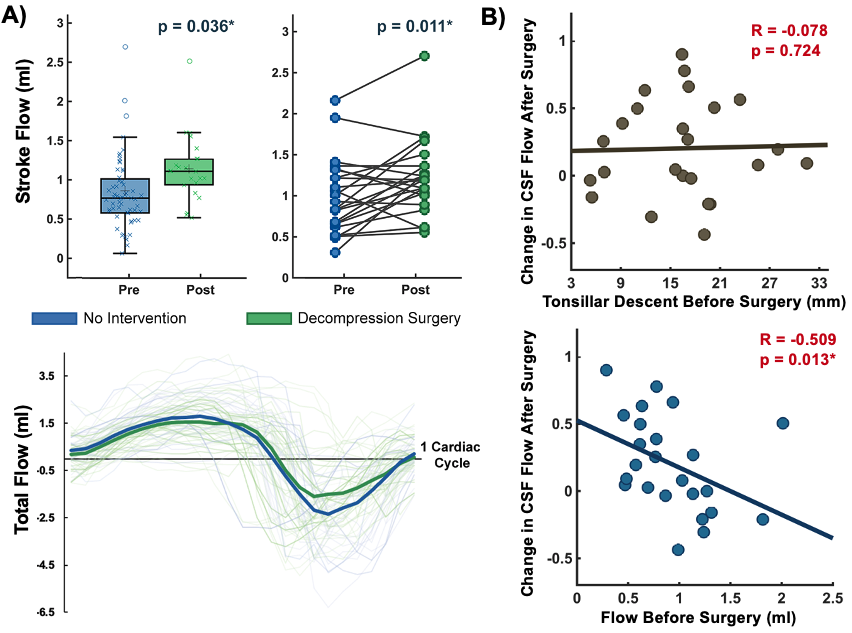
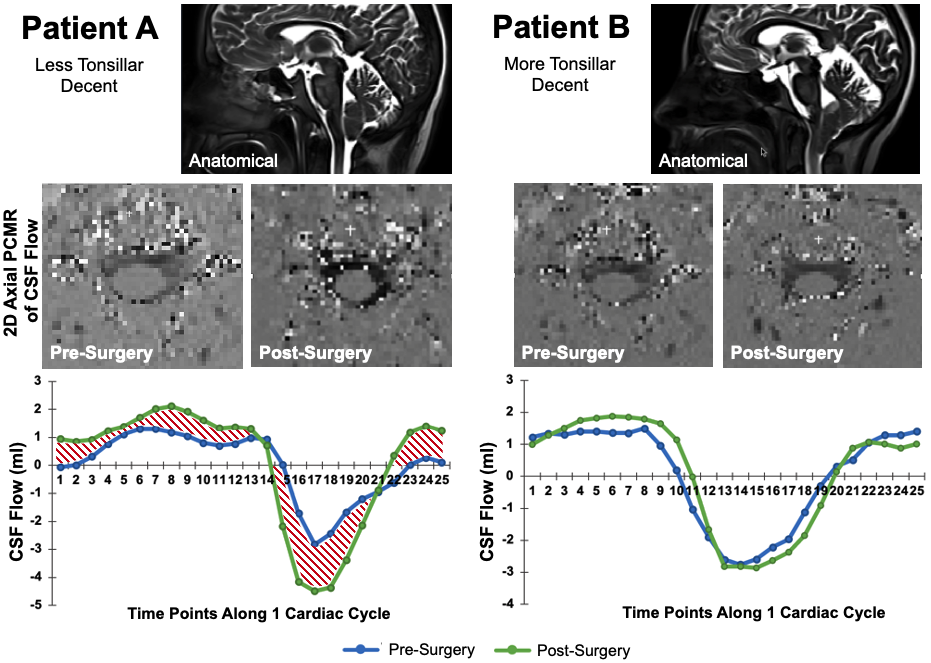
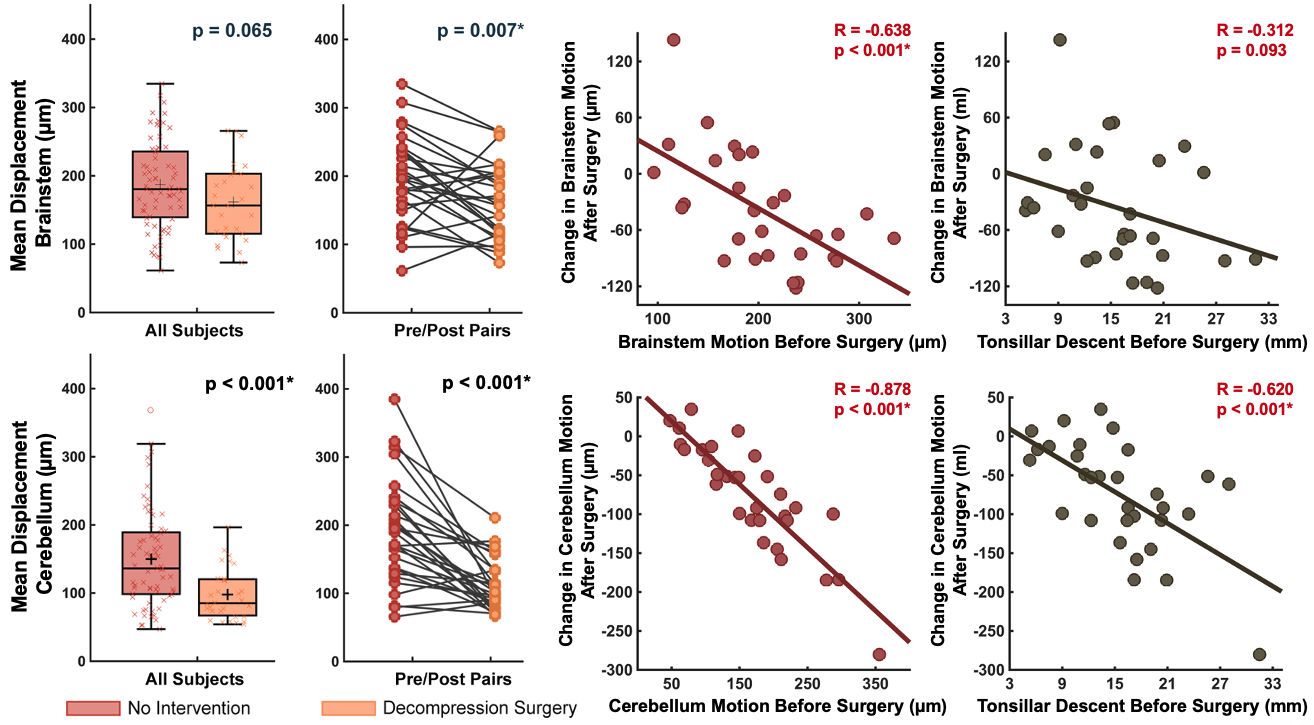
CSF stroke volume was 0.86±0.58ml in CM-I patients. After PDF surgery, CSF stroke volume was 1.14±0.43ml (p=0.036; Figure 2). Pairwise (pre/post-surgery) we saw a 40.5% increase to CSF stroke volume (p=0.011). Notably, we found that CSF flow increases seen after surgery had no relationship to tonsillar descent (R = -0.078, p =0.724), but did relate to amount of pre-surgical flow (R = -0.509, p=0.013; Figure 3). Showing that only subjects with low initial flow had a significant surgical increase in flow, regardless of severity of tonsillar descent.We also found that pulsatile motion decreases significantly after surgery, with brainstem motion decreasing 17.3% (p=0.007) and cerebellum motion decreasing 45.2% with surgery (p<0.001). We again found that improvements were better predicted by the amount of pre-surgical motion (Brainstem: R = -0.638, p<0.001; Cerebellum: R = -0.878, p<0.001) than by tonsillar descent (Brainstem: R = -0.312, p=0.093; Cerebellum: R = -0.620, p<0.001). This implies that subjects with high initial brain motion had a significant post-surgical decrease in motion, regardless of severity of tonsillar descent.
Discussion
The Monroe-Kellie Doctrine dictates that to maintain normal intracranial pressure, the cranial cavity must maintain consistent volume, and therefore when the arterial pulse leads to systolic expansion of brain tissue, CSF is passively pushed out of the skull[10]. However, in CM-I, the passive flow of CSF is obstructed, and to compensate, the brainstem and cerebellum must displace more to maintain cerebral homeostasis[11,12]. These changes to cerebral dynamics are presumed to cause clinical symptoms[13]. With the creation of adequate space for CSF flow through PFD surgery, CSF flow increases and brain motion decreases towards normal.While amount of tonsillar decent is the standard imaging marker, it has proven to be a poor measure of CM-I severity, as other factors like foramen magnum size and crowding also affect cerebral dynamics. Here we instead directly measured cerebral dynamics. We showed that only the patients who had severely impacted CSF flow and brain motion realized improved cerebral dynamic improvements with surgery, regardless of tonsillar descent. CSF flow is frequently assessed in PFD, but almost always using either qualitative assessments of geometric images, or with PCMR acquired in a sagittal plane, which is inadequate to characterize flow. Brain motion is only recently been measured in CM-I, and therefore work in this area is extremely limited[2,14].
Conclusion
We showed pre-surgical CSF flow and brain motion in CM-I are important indicators of potential benefits from PFD surgery. Further research is needed to determine how cerebral dynamics affect clinical outcome measures.Acknowledgements
Conquer Chiari FoundationReferences
- Ramón C, Gonzáles-Mandly A, Pascual J. What differences exist in the appropriate treatment of congenital versus acquired adult Chiari type I malformation? Curr Pain Headache Rep. 2011;15(3):157-163.
- Eppelheimer MS, Nwotchouang BST, Pahlavian SH, et al. Cerebellar and brainstem displacement measured with DENSE MRI in chiari malformation following posterior fossa decompression surgery. Radiology. 2021;301(1):187-194.
- Langridge B, Phillips E, Choi D. Chiari Malformation Type 1: A Systematic Review of Natural History and Conservative Management. World Neurosurg. 2017;104:213-219.
- Chavez A, Roguski M, Killeen A, Heilman C, Hwang S. Comparison of operative and non-operative outcomes based on surgical selection criteria for patients with Chiari i malformations. J Clin Neurosci. 2014;21(12):2201-2206.
- Tubbs RS, Elton S, Grabb P, Dockery SE, Bartolucci AA, Oakes WJ. Analysis of the posterior fossa in children with the Chiari 0 malformation. Neurosurgery. 2001;48(5):1050-1055.
- de Oliveira Sousa U, de Oliveira MF, Heringer LC, Barcelos ACES, Botelho RV. The effect of posterior fossa decompression in adult Chiari malformation and basilar invagination: a systematic review and meta-analysis. Neurosurg Rev. 2018;41(1):311-321.
- Bejjani GK. Definition of the adult Chiari malformation: a brief historical overview. Neurosurg Focus. 2001;11(1):1-8.
- Ventureyra ECG, Aziz HA, Vassilyadi M. The role of cine flow MRI in children with Chiari I malformation. Child’s Nerv Syst. 2003;19(2):109-113.
- Pahlavian SH, Oshinski J, Zhong X, Loth F, Amini R. Regional Quantification of Brain Tissue Strain Using Displacement-Encoding With Stimulated Echoes Magnetic Resonance Imaging. J Biomech Eng. 2018;140(8):081010.
- Zhong X, Meyer CH, Schlesinger DJ, et al. Tracking brain motion during the cardiac cycle using spiral cine-DENSE MRI. Med Phys. 2009;36(8):3413-3419.
- Wilson MH. Monro-Kellie 2.0: The dynamic vascular and venous pathophysiological components of intracranial pressure. J Cereb Blood Flow Metab. 2016;36(8):1338-1350.
- Mokri B. The Monro-Kellie hypothesis. Neurology. 2001;56(12):1746-1748.
- Ciaramitaro P, Ferraris M, Massaro F, Garbossa D. Clinical diagnosis—part I: what is really caused by Chiari I. Child’s Nerv Syst. 2019;35(10):1673-1679.
- Leung V, Magnussen JS, Stoodley MA, Bilston LE. Cerebellar and hindbrain motion in Chiari malformation with and without syringomyelia. J Neurosurg Spine. 2016;24(4):546-555.
Figures