1178
Association Between Epicardial Adipose Tissue volume and Microvascular Obstruction in Patients with STEMI1Department of Radiology, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, China, Nanjing, China, 2Department of Cardiology, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, China, Nanjing, China, 3Philips Healthcare, Shanghai, China, 4Philips Healthcare, Beijing, China
Synopsis
Keywords: Inflammation, Infiltration, Cardiovascular, CMR
Motivation: Microvascular obstruction (MVO) after primary percutaneous coronary intervention (pPCI) is identifed as an independent risk factor for poor prognosis in patients with acute myocardial infarction (AMI). However, the clinical implications of Epicardial adipose tissue (EAT) in microvascular obstruction formation in patients with ST-segment elevation myocardial infarction (STEMI) remain unclear.
Goal(s): This study aimed to evaluate the correlation between EAT and MVO volume detected by CMR in STEMI patients.
Approach: Cardiac magnetic resonance (CMR) has emerged as the gold standard technique to detect the extent of MVO and evaluate EAT volume.
Results: Left atrioventricular EAT mass index is an independent predictor of MVO.
Impact: Measurement of EAT using CMR could be used for risk stratification and may be a promising target in developing new therapies to reduce myocardial reperfusion injury in patients with STEMI.
Introduction
Epicardial adipose tissue (EAT), a metabolically active fat depot between the visceral pericardium and the outer margin of the myocardium, has gradually emerged as a novel target for risk stratification in coronary artery disease due to its distinctive location and multifaceted metabolic properties. Microvascular obstruction (MVO) following primary percutaneous coronary intervention (pPCI) is identifed as an independent risk factor for poor prognosis in patients with acute myocardial infarction (AMI). However, the clinical implications of EAT in the formation of microvascular obstruction in patients with ST-segment elevation myocardial infarction (STEMI) remain unclear. Recently, cardiac magnetic resonance (CMR) has emerged as the gold standard technique to detect the extent of MVO and evaluate EAT volume. This study aimed to evaluate the correlation between EAT and MVO volume detected by CMR in STEMI patients.Methods
A total of 129 STEMI patients who underwent pPCI successfully were enrolled. Clinical characteristics including demographic characteristics, cardiovascular risk factors, laboratory data and angiographic parameters were recorded from each patient by 1 trained physician. All patients underwent CMR within 1 week following pPCI to evaluate infarct size, MVO volume and EAT distribution. All CMR data were transferred to Q-MASS MR 8.1 imaging system (Medis, Leiden, The Netherlands) and interpreted twice by 2 expert radiologists who were blinded to the angiographic and clinical data of patients.Results
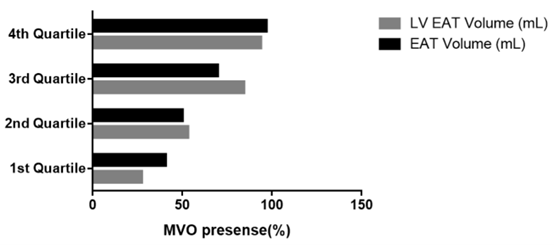
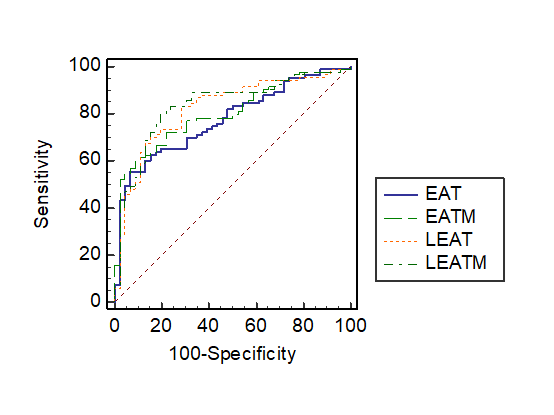
Compared to STEMI patients without MVO, STEMI patients with MVO presented with higher peak troponin T levels, increase of neutrophil lymphocyte ratio (NLR) and C-reactive protein (CRP), larger infarct size and compromised left ventricular ejection fraction (LVEF%). Total EAT volume, EAT mass index, left atrioventricular EAT volume, left atrioventricular EAT mass index and thickness of EAT in the left atrioventricular groove were unanimously associated with the occurrence of MVO. The left atrioventricular EAT mass index in STEMI patients with MVO were significantly larger than that in STEMI patients without MVO (24.72±5.049 g/m2 vs 18.63±3.670 g/m2, P<0.001). Multivariate logistic regression analysis demonstrated that NLR, peak troponin T levels and left atrioventricular EAT mass index were independent predictors of MVO. Left ventricular EAT mass significantly predicted the presence of MVO (area under the curve [AUC]: 0.83 [95% CI: 0.760 to 0.895; P<0.001).Discussion & Conclusions
Left atrioventricular EAT mass index is an independent predictor of MVO. Measurement of EAT using CMR could be used for risk stratification and may be a promising target in developing new therapies to reduce myocardial reperfusion injury in patients with STEMI. A quick identification of high EAT mass index could define a subset of patients in which potential therapeutic strategy, such as GLP-1 or targeted therapy against EAT, could be developed to alleviate myocardial damage.Acknowledgements
No acknowledgement found.References
No reference found.Figures