1177
3D Isotropic Wideband LGE for Supporting Ventricular Tachycardia Ablation in Patients with an Implantable Cardioverter Defibrillator1Northwestern University Feinberg School of Medicine, Chicago, IL, United States, 2Mayo Clinic, Chicago, IL, United States, 3University of Virginia, Charlottesville, VA, United States, 4Hospital of the University of Pennsylvania, Philadelphia, PA, United States
Synopsis
Keywords: Arrhythmia, Tissue Characterization, ventricular tachycardia, catheter ablation
Motivation: Catheter ablation is clinically indicated for targeting re-entrant ventricular tachycardia (VT) in patients with an implantable cardioverter defibrillator (ICD), but its 1-year VT recurrence rate is high. We hypothesize that 3D wideband LGE is useful for guiding VT ablation.
Goal(s): To determine whether 3D wideband LGE correlates with electroanatomic mapping (EAM) in ICD patients.
Approach: To develop a 3D isotropic wideband LGE pulse sequence and validate it against EAM in ICD patients.
Results: While myocardial scars and gray-zones in LGE correlated with the low voltage areas (<1.5 mV) in EAM, mid-myocardial non-ischemic scars was not correlated between LGE and EAM.
Impact: High-resolution 3D isotropic wideband LGE has potential to increase the success rate of catheter ablation for re-entrant ventricular tachycardia in patients with an implantable cardioverter defibrillation, as well as decrease the procedural time by providing a roadmap prior to ablation.
INTRODUCTION
Catheter ablation is clinically indicated for re-entrant ventricular tachycardia (VT) in patients with myocardial infarction.1 Despite using electroanatomic mapping (EAM) during VT ablation to identify ablation targets or arrhythmogenic substrates, 1-year success rate of VT ablation remains poor (25%-87%).2 High spatial resolution late gadolinium enhanced (LGE) MRI for visualizing arrhythmogenic substrates has been suggested for improving the post-ablation outcomes.3 Many VT ablation candidates, unfortunately, have an implantable cardioverter defibrillator (ICD), which causes significant image artifacts. A previous study reported 3D wideband LGE for ICD patients, but its spatial resolution of 1.4x1.4x4.0mm3 is sensitive to partial volume averaging.4 In this study, we sought to develop a free-breathing (FB), 3D isotropic wideband LGE pulse sequence using a combination of stack-of-stars k-space sampling, 2D self-navigator, and XD-GRASP5 reconstruction, and determine whether wideband LGE correlates with EAM in ICD patients undergoing VT ablation.METHODS
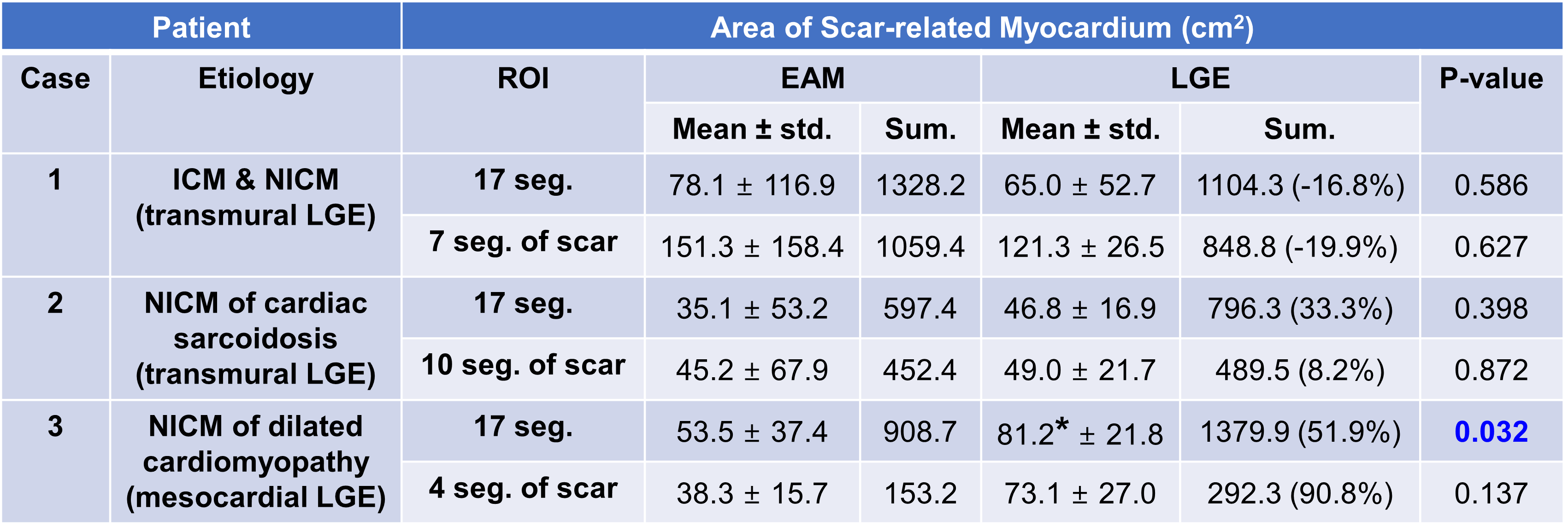
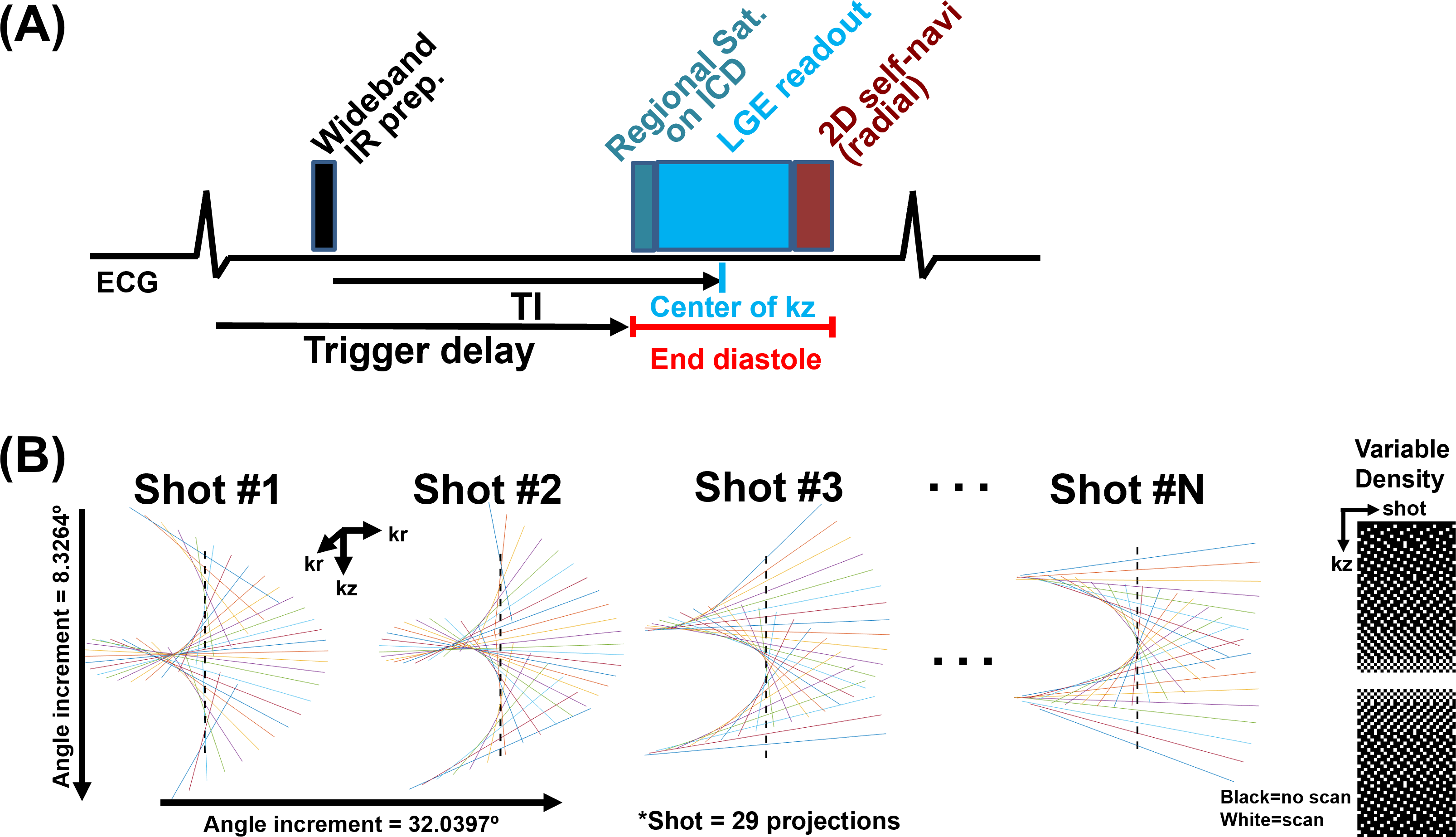
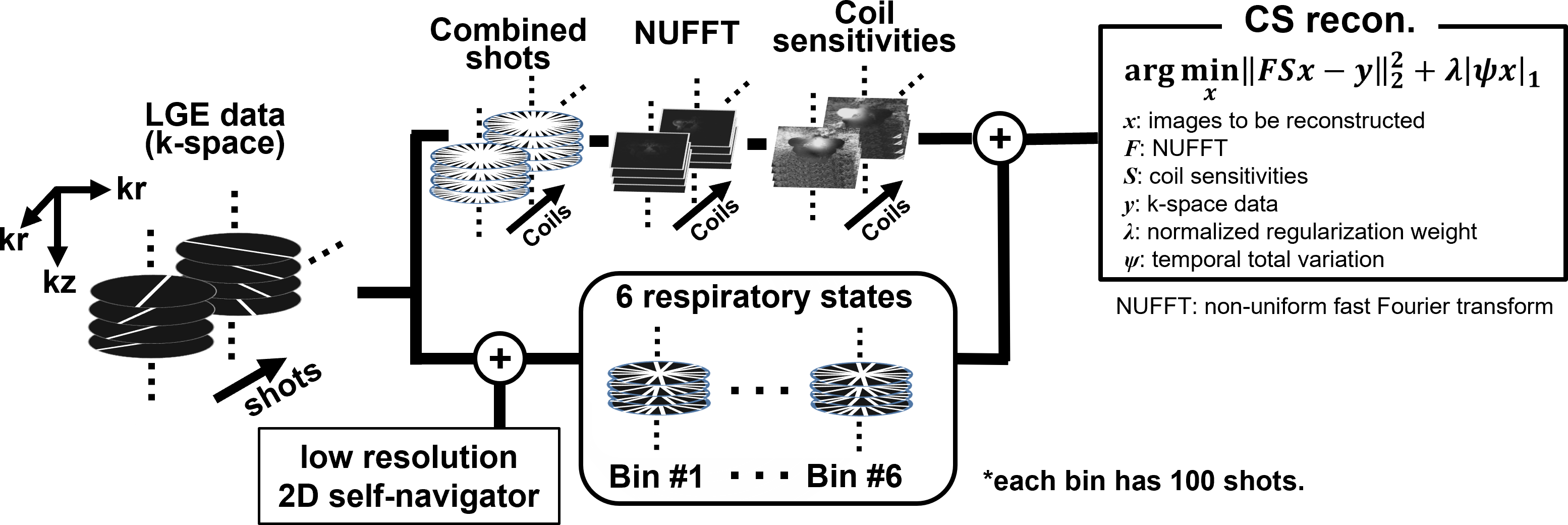
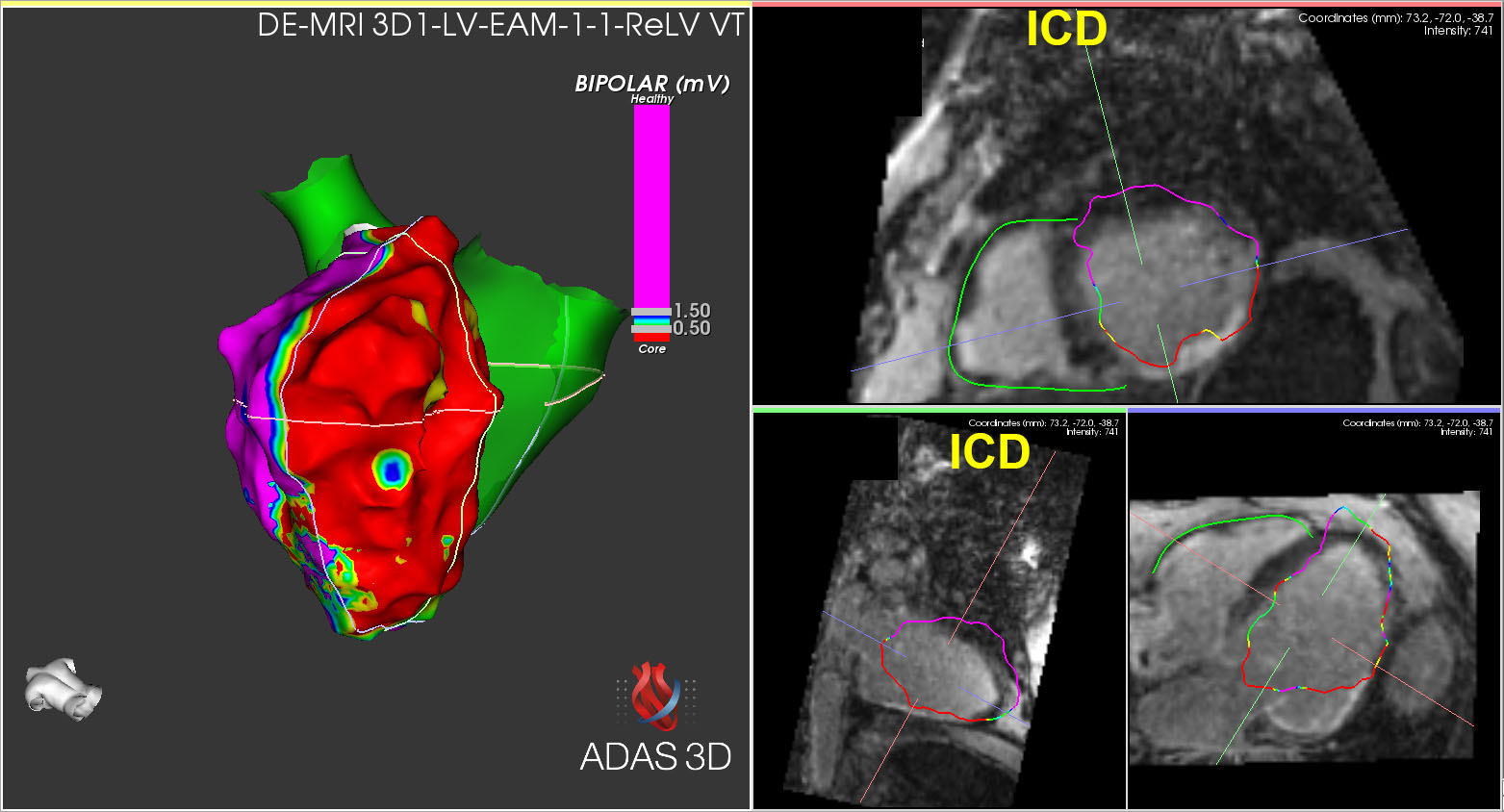
Pulse Sequence: For 3D wideband LGE, we incorporated a wideband (~4 kHz) inversion-recovery RF pulse into a stack-of-stars LGE pulse sequence with 2D self-navigator (see Figure 1).6 The relevant imaging parameters were: FOV=320x320x160 mm3 (coronal view), reconstruction matrix=160x160x80, spatial resolution=2.0x2.0x2.0 mm3, 20% oversampling in kz (96 slices in total), flip angle=18°, TE/TR =1.5/3.8 msec, receiver bandwidth=501 Hz/pixel, asymmetric echo (0.77), spoiled gradient-recalled echo readout, 29 radial projections per heartbeat (or shot) along kz with variable density, LGE readout duration=~120 msec, projection angle increment of 8.3264° within a shot and 32.0397° between shots, ECG trigger every heartbeat, total scan duration=600 heartbeats, two regional saturation bands on abdomen and ICD to suppress image artifacts. MRI: We enrolled 3 patients with an ICD (2/1 males/females, mean age=65.3±6.0yrs) undergoing a cardiac MRI on a 1.5T MRI scanner (Avanto, Siemens) prior to VT ablation. Etiology of cardiomyopathy in patients was described in Table 1. We performed ECG-gated, FB 3D isotropic wideband LGE scans at 25 minutes following administration of 0.2 mmol/kg of gadobutrol (Gadavist, Bayer). Image reconstruction: We performed XD-GRASP reconstruction5 after rebinning LGE data into 6 respiratory states based on respiratory motions extracted from low-resolution 2D self-navigator (see Figure 2).6 Image analysis: In the ADAS3D software (version 2.12.1, Barcelona, Spain), the whole LV was contoured using an AI tool followed by manual correction. For the classification of normal and scarred myocardium, we adjusted two thresholds for normal and scar image intensity, respectively, by using a full-width half-maximum method. We also quantified the area of healthy and infarct using the AHA 17-segment model. Merging EAM onto LGE: Using 48-electrode catheter (OPTRELL, Biosense Webster), bipolar voltages of EAM on endo- and epi-LV myocardium were recorded during VT ablation (CARTO, Biosense Webster) and imported into ADAS3D. Also, left and right coronary cusp and LV morphologies were imaged by echocardiography and used as landmarks for accurate registration onto LGE. After merging, we quantified the surface area of normal (≥1.5 mV) and scar-related (<1.5 mV) measurements using the 17-segment model: surface area = the number of measured EAM points × 0.9 mm2 surface area of an electrode7. Note that the duplicated points were eliminated. Statistical Analysis: We compared the area of scar-related myocardium between LGE (scar+grayzone) and EAM (<1.5mV) using a paired t-test. P<0.05 was considered statistically significant.RESULTS
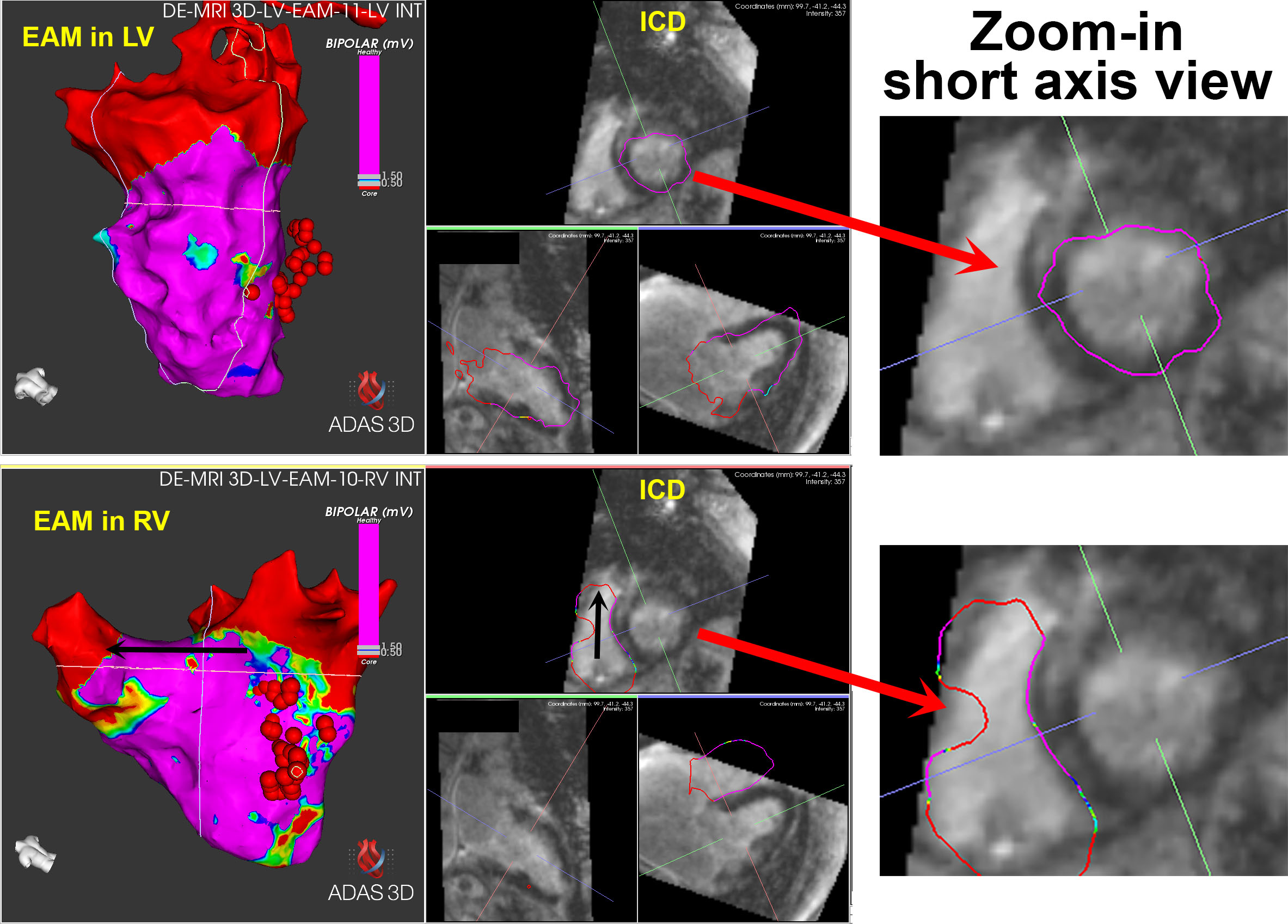
The mean scan time of 3D wideband LGE was 8.5 ± 0.3 min; the mean XD-GRASP reconstruction time was 141.7 ± 12.6 min using a GPU workstation (12 GB Tesla P100, NVIDIA). As summarized in Table 1, the scar-related area was not significantly different between EAM and LGE in two patients with transmural scar (see Figure 3 as an example), whereas the area was significantly different in one patient with mid-myocardial scar (see Figure 4).DISCUSSION
This study demonstrates the feasibility of performing 3D isotropic wideband LGE for guiding VT ablation in ICD patients, particularly for patients in whom the conventional EAM is likely to miss mid-myocardial scarring. A future study included a large cohort of ICD patients is warranted to fully validate the clinical utility of 3D wideband LGE for supporting VT ablation.CONCLUSION
3D isotropic wideband LGE correlates with EAM in ICD patients with myocardial scar and may guide VT ablation.Acknowledgements
This work is supported by the National Institutes of Health (R01HL116895, 1R01HL167148‐01A1, R01HL151079, R21EB030806A1), the Radiological Society of North America (EILTC2302) and the American Heart Association (19IPLOI34760317, 949899).References
1. Roderick Tung, et al. Freedom from recurrent ventricular tachycardia after catheter ablation is associated with improved survival in patients with structural heart disease: An International VT Ablation Center Collaborative Group study. Heart Rhythm 2015;12:1997–2007.
2. Liang JJ, Santangeli P, Callans DJ. Long-term Outcomes of Ventricular Tachycardia Ablation in Different Types of Structural Heart Disease. Arrhythm Electrophysiol Rev. 2015 Dec;4(3):177-83. doi: 10.15420/aer.2015.4.3.177. Epub 2015 Dec 1. PMID: 26835122; PMCID: PMC4732176.
3. Hennig A, Salel M, Sacher F et al. High-resolution three-dimensional late gadolinium-enhanced cardiac magnetic resonance imaging to identify the underlying substrate of ventricular arrhythmia. Europace 2018;20(Fi2):f179–f191.
4. Rashid S, Rapacchi S, Shivkumar K, Plotnik A, Finn JP, Hu P. Modified wideband three-dimensional late gadolinium enhancement MRI for patients with implantable cardiac devices. Magn Res Med 2016;75:572–584.
5. Feng L, Axel L, Chandarana H, Block KT, Sodickson DK, Otazo R. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magn Reson Med 2016;75(2):775-88.
6. Hong K, Gunasekaran S, Elbaz M, et al. 2D self-navigation improves respiratory motion tracking compared with 1D self-navigation in 3D left atrial LGE using XD-GRASP reconstruction. In preceedings of 2023 ISMRM, Toronto, Canada, program 1013.
7. Tan JL, Guandalini GS, Hyman MC, Arkles J, Santangeli P, Schaller RD, Garcia F, Supple G, Frankel DS, Nazarian S, Lin D, Callans D, Marchlinski FE, Markman TM. Substrate and arrhythmia characterization using the multi-electrode Optrell mapping catheter for ventricular arrhythmia ablation-a single-center experience. J Interv Card Electrophysiol. 2023 Aug 18. doi: 10.1007/s10840-023-01618-5. Epub ahead of print. PMID: 37592198.
Figures