1176
Single-click joint bright- and black-blood late gadolinium enhancement and T1-rho mapping for improved myocardial scar imaging1IHU LIRYC, Electrophysiology and Heart Modeling Institute, Université de Bordeaux - INSERM, Centre de Recherche Cardio-Thoracique de Bordeaux, U1045, Avenue du Haut Lévêque, Bordeaux, France, 2Department of Cardiovascular Imaging, Hôpital Cardiologique du Haut-Lévêque, CHU de Bordeaux, Bordeaux, France, 3Department of Diagnostic and Interventional Radiology, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland, 4CIBM Center for Biomedical Imaging, Lausanne, Switzerland
Synopsis
Keywords: Myocardium, Quantitative Imaging, Tissue characterization, myocardial infarction, black-blood imaging
Motivation: Bright-blood sequences are used to retrieve information about cardiac anatomy and function, while black-blood sequences have been exploited for focal scar detection. Moreover, contrast agent-free T1-rho (T1ρ) mapping has shown promise for scar quantification, particularly of diffuse nature.
Goal(s): We propose SPOT1ρ, a single-click joint bright-blood, black-blood, and T1ρ mapping sequence providing improved scar localization, detection, and quantification.
Approach: The proposed SPOT1ρ was compared to reference sequences in phantom and patients (three myocardial infarctions, one cardiac amyloidosis and one healthy control).
Results: Excellent correlation was observed between SPOT1ρ and reference T1ρ values, along with co-registered bright- and black-blood images in phantom and patients.
Impact: The proposed single-click SPOT1ρ permits easier and faster planning for MR technicians, more comfort for the patient, promoted by fewer breath-holds, and a simplified interpretation for the radiologists, through co-registered, qualitative, and quantitative images.
Background
Cardiovascular magnetic resonance (CMR) imaging has become pivotal in characterizing myocardial scars. Bright-blood sequences are used to retrieve information about cardiac anatomy and function1. Concurrently, novel black-blood late gadolinium enhancement (LGE) sequences have showcased remarkable potential for scar detection by uncovering scar patterns that may be otherwise confounded with blood signal. This is particularly valuable for identifying focal sub-endocardial scars2,3. Moreover, contrast-agent-free T1-rho (T1ρ) mapping has shown promise in quantifying cardiomyopathies, especially those of diffuse nature4.Nowadays, these images are acquired sequentially through multiple breath-holds, which adds to the workload of MR technicians, reduces patient comfort, and hampers image analysis due to spatial misalignment caused by the differences in breath-hold positions.
Here we introduce a unified ‘one-click’ sequence that seamlessly integrates the strengths of black-blood scar detection, bright-blood scar localization, and T1ρ scar quantification.
Methods
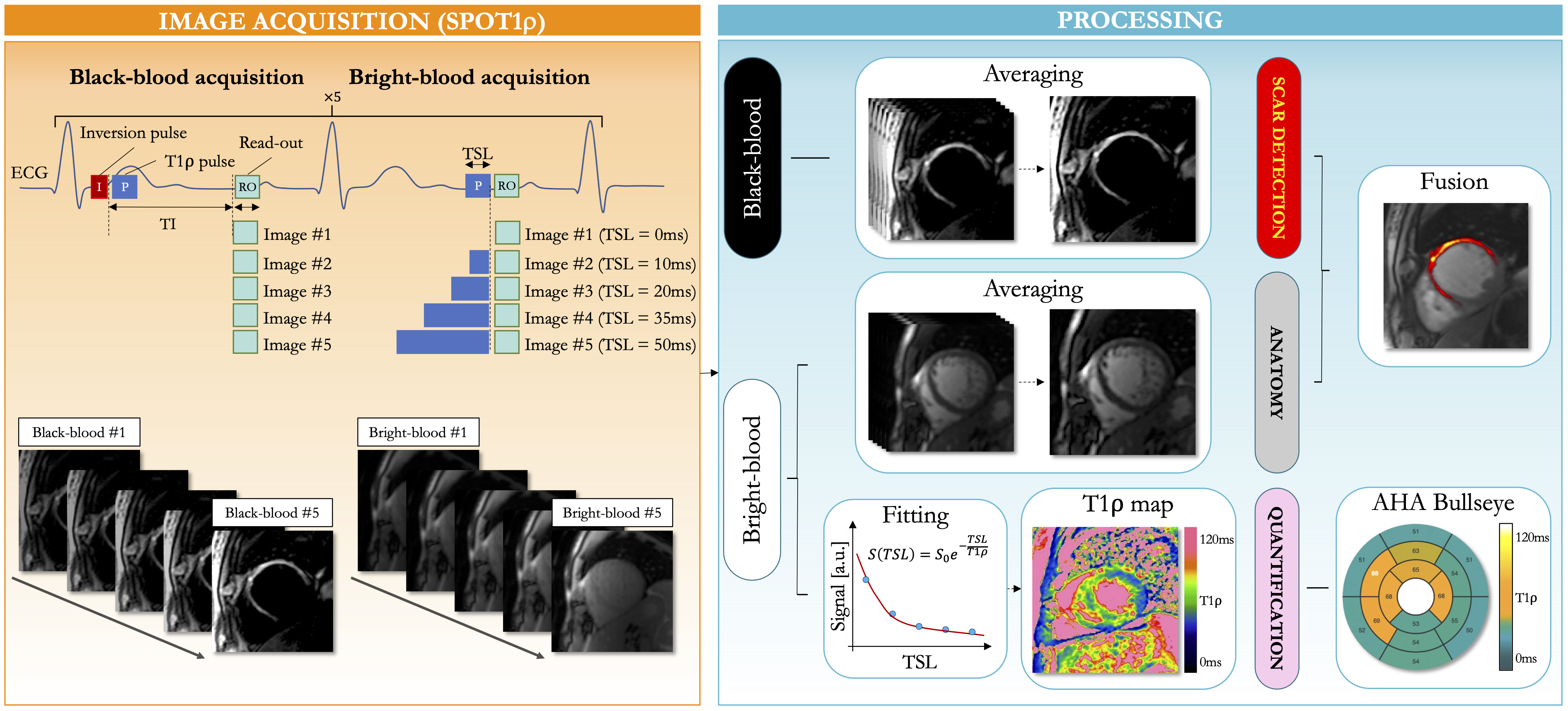
Acquisition: The proposed SPOT1ρ sequence (Fig.1) is a single-shot ECG-triggered 2D balanced steady-state free-precession sequence that collects co-registered black-blood (for scar detection) and bright-blood (for scar localization) images in an interleaved fashion. In odd heartbeats, a 180° non-selective inversion pulse (duration of 10ms) is followed by a T1ρ module5 to generate black-blood contrast. In even heartbeats, only a T1ρ module is played out to generate bright-blood contrast.For each slice position, ten single-shot images (5 bright-blood and 5 black-blood) were acquired in mid-diastole over 10 heartbeats. The T1ρ preparation time was increased ([0, 10, 20, 35, 50]ms) for every bright-blood acquisition to generate a T1ρ map through a 2-parameter curve fitting process5.
Four sets of images were reconstructed and displayed on the scanner console: i) averaged bright-blood images, ii) averaged black-blood images, iii) a coloured fusion of both, and iv) the T1ρ maps.
Scan parameters: Short-axis images were acquired during breath-hold with whole ventricular coverage. Imaging parameters were: 10-20 slices, 5 signal averages, 1.4mmx1.4mm in-plane resolution, 8mm slice thickness, spin-lock frequency=400Hz, FA=60°, GRAPPA x2, ~160ms acquisition window, TE/TR=1.2/2.8ms, bandwidth=870Hz/pixel, inversion time determined from a prior scout acquisition to null both blood and healthy myocardium.
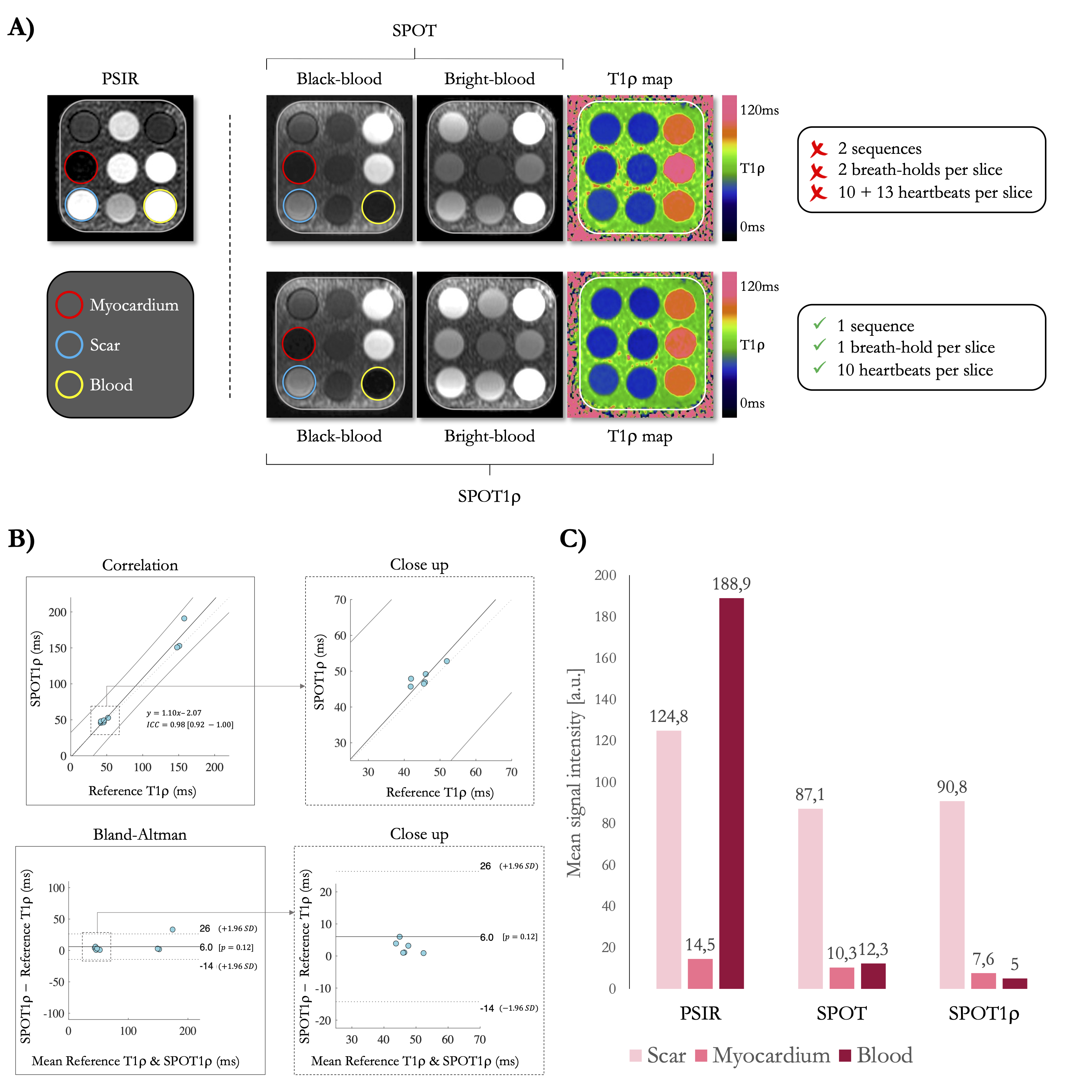
Experiments: The proposed SPOT1ρ was compared to the reference breath-hold phase-sensitive inversion recovery (PSIR)6, to joint bright- and black-blood LGE (SPOT)3 and to T1ρ mapping sequences4 in all experiments. Phantom experiments with the T1MES7 were used to assess T1ρ accuracy and bright- and black-blood performance. The phantom was scanned using a simulated heartrate of 60 bpm. The concordance between the T1ρ values acquired from the reference T1ρ mapping and SPOT1ρ was evaluated with a Bland-Altman analysis and intra-class correlation coefficients (ICC). Mean signal intensities from blood, healthy myocardium, and scar vials were measured and compared between sequences.
Three patients with myocardial infarction, one patient with cardiac amyloidosis and one healthy subject underwent CMR at a 1.5T scanner (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany). Acquisitions were performed in a random order 15min post-injection of 0.2mmol/kg gadoteric acid. Mean T1ρ values were measured in both the remote (areas without LGE) and injured (areas with LGE) myocardium by drawing regions of interest over the maps. Acquisition times were recorded.
Results
Acquisition times for PSIR, SPOT, T1ρ mapping and SPOT1ρ were 10, 10, 13, and 10 heartbeats per slice, respectively.In the phantom, an excellent correlation was observed between the reference T1ρ values and those obtained using the SPOT1ρ sequence (ICC=0.98 [0.92-1.0]). PSIR effectively reduced the signal from healthy myocardium while enhancing the scar signal, which stayed close to the blood signal. SPOT and SPOT1ρ efficiently attenuated signals for both blood and healthy myocardium on black-blood images. Excellent visual and qualitative agreements were obtained between SPOT1ρ and the original SPOT sequence (Fig.2).
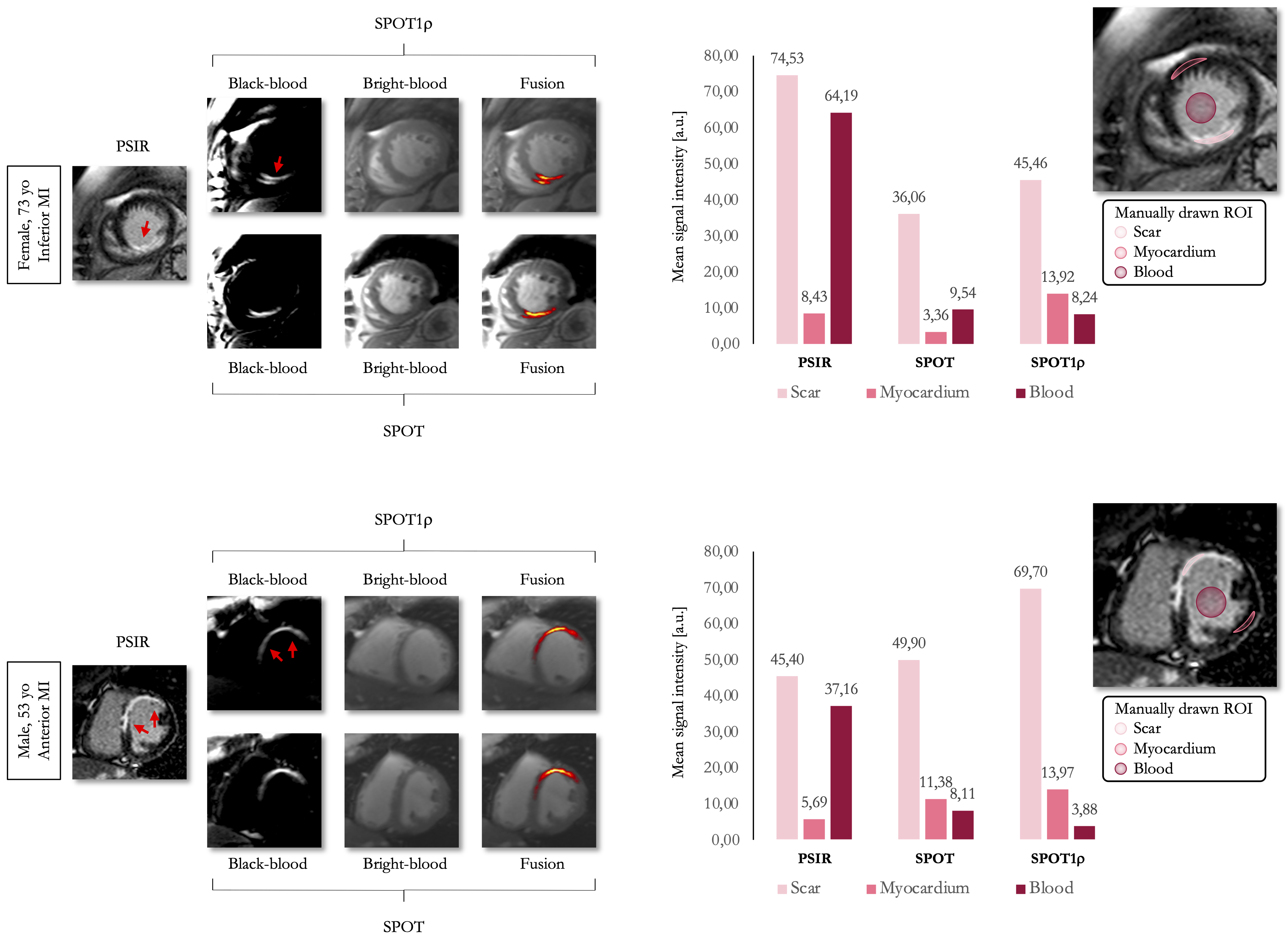
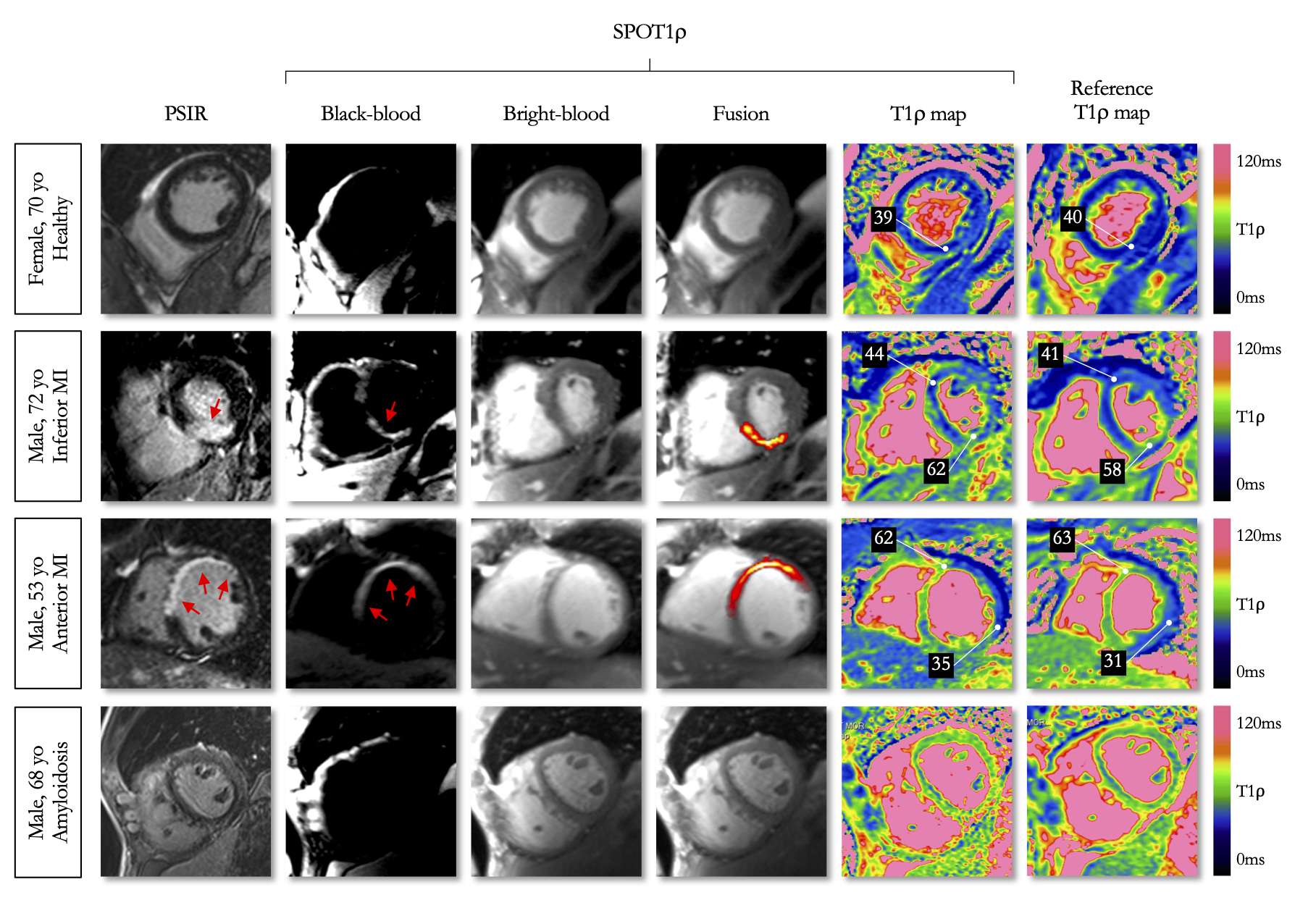
In patients, similar observations were made, with the added benefit of having a coloured fusion of both bright- and black-blood images for optimal scar detection and localisation (Fig.3). Elevated myocardial T1ρ values were observed in injured areas compared to remote areas (35±3ms vs. 62±7ms), closely matching values obtained from the reference T1ρ mapping sequence (31±3ms vs. 63±5ms) (Fig.4).
Conclusion and Discussion
This work aimed to integrate improved scar detection, scar localization and tissue characterization into a single sequence while promoting time efficiency and patient comfort. Results obtained in-vitro and in-vivo in patients showcase the potential of SPOT1ρ to offer accurate T1ρ values. The produced bright-blood and black-blood images closely matched those generated by the original sequential sequences, suggesting that we can efficiently substitute these sequences with a simplified one-click approach. More clinical validations in larger cohort of patients with various ischemic, non-ischemic, focal, and diffuse cardiomyopathies are now warranted.Acknowledgements
This work was supported by funding from the French National Research Agency under grant agreements Equipex MUSIC ANR-11-EQPX-0030, ANR-21-CE17-0034-01, Programme d’Investissements d’Avenir ANR-10-IAHU04-LIRYC, ANR-22-CPJ2-0009-01, and from the European Research Council (ERC) under the European Union’s Horizon 2020 research and innovation program (grant agreement N°101076351).References
1. Kuruvilla S, Adenaw N, Katwal AB, Lipinski MJ, Kramer CM, Salerno M. Late Gadolinium Enhancement on Cardiac Magnetic Resonance Predicts Adverse Cardiovascular Outcomes in Nonischemic Cardiomyopathy: A Systematic Review and Meta-Analysis. Circ: Cardiovascular Imaging. 2014;7(2):250-258. doi:10.1161/CIRCIMAGING.113.001144
2. Henningsson M, Malik S, Botnar R, Castellanos D, Hussain T, Leiner T. Black-Blood Contrast in Cardiovascular MRI. Journal of magnetic resonance imaging : JMRI. 2022;55(1):61-80. doi:10.1002/jmri.27399
3. Bustin A, Sridi S, Kamakura T, Jais P, Stuber M, Cochet H. Free-breathing joint bright- and black-blood cardiovascular magnetic resonance imaging for the improved visualization of ablation-related radiofrequency lesions in the left ventricle. EP Europace. 2022;24(Supplement_1):euac053.594. doi:10.1093/europace/euac053.594
4. Bustin A, Witschey WRT, Van Heeswijk RB, Cochet H, Stuber M. Magnetic resonance myocardial T1ρ mapping: Technical overview, challenges, emerging developments, and clinical applications. J Cardiovasc Magn Reson. 2023;25(1):34. doi:10.1186/s12968-023-00940-1
5. Bustin A, Toupin S, Sridi S, et al. Endogenous assessment of myocardial injury with single-shot model-based non-rigid motion-corrected T1 rho mapping. J Cardiovasc Magn Reson. 2021;23(1):119. doi:10.1186/s12968-021-00781-w
6. Kellman P, Arai AE, McVeigh ER, Aletras AH. Phase-sensitive inversion recovery for detecting myocardial infarction using gadolinium-delayed hyperenhancement. Magnetic resonance in medicine. 2002;47(2):372-383. doi:10.1002/mrm.10051
7. Captur G, Gatehouse P, Keenan KE, et al. A medical device-grade T1 and ECV phantom for global T1 mapping quality assurance—the T1 Mapping and ECV Standardization in cardiovascular magnetic resonance (T1MES) program. J Cardiovasc Magn Reson. 2016;18(1):58. doi:10.1186/s12968-016-0280-z
Figures