1175
Multi-Contrast 3D Whole-Heart MRI for Intramyocardial Hemorrhage Stage Assessment in Patients with Myocardial Infarction1Beijing Chaoyang Hosipital, Beijing, China, 2Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, Shenzhen, China, 3China MR Scientific Marketing, Siemens Healthineers, Beijing, China, Beijing, China, 4MR Research Collaborations, Siemens Healthcare Limited, Camberley, UK, Camberley, United Kingdom, 5School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, London, United Kingdom, 6School of Engineering, Pontificia Universidad Católica de Chile, Santiago, Chile, 7Department of Radiology, Beijing Chaoyang Hospital, Capital Medical University, No. 8 Gongti 13 South Road, Chaoyang District, Beijing 100020, China, Beijing, China
Synopsis
Keywords: Myocardium, Cardiovascular
Motivation: Intramyocardial hemorrhage (IMH) staging can serve as a valuable reference point when exploring treatment options for this condition, but methodsfor detecting IMH staging has not been fully examined.
Goal(s): This study investigated whether BOOST, a novel iNAV-based free-breathing, multi-contrast 3D whole-heart MRI sequence could detect and stage IMH.
Approach: The efficacy of BOOST in diagnosing and staging IMH were compared with the performances of conventional T2* sequences.
Results: BOOST, used for IMH detection at 3T, demonstrates superior sensitivity and specificity, along with good quantitative consistency, relative to T2* alone. Additionally, BOOST has substantial potential for IMH staging.
Impact: The BOOST sequence can be used for future IMH staging, which will facilitate precise multi-dimensional IMH assessment, ultimately enabling accurate and targeted IMH treatment.
Introduction
Intramyocardial hemorrhage (IMH) is a major threat to patients with myocardial infarction because it can cause expansion of the infarcted myocardial area1, leading to unfavorable left ventricular remodeling. Currently, there is no effective treatment for IMH. Accurate IMH staging is expected to provide valuable reference information for developing therapy. The T2/T2* sequences commonly used to evaluate IMH do not provide staging information alone2. To combine T2 and T2* sensitive imaging in a single scan, free-breathing multi-contrast three-dimensional (3D) whole-heart bright-blood and black-blood phase sensitive inversion recovery sequence (iT2prep‐IR BOOST) has been extended to 3T using GRE-Dixon readouts. This study first explored whether iT2prep‐IR BOOST can diagnose and distinguish the IMH phase, and then evaluated the ability of BOOST to identify left ventricular thrombus (LVT).Methods
Cardiac magnetic resonance (CMR) was performed on a 3T scanner (MAGNETOM Prisma, Siemens Healthineers AG, Erlangen, Germany), including a research 3D whole-heart iT2prep‐IR BOOST sequence3 with GRE-Dixon readout, cine, T2-weighted short-tau inversion recovery (T2-STIR), T2* mapping, and late gadolinium enhancement (LGE). iT2prep‐IR BOOST imaging parameters were set as follow: coronal orientation, isotropic spatial resolution 1.4 × 1.4 × 1.4 mm3, FOV = 320 × 320 × 100 mm3, bandwidth = 893 Hz/pixel, repetition time = 4.5 ms, echo time = 1.39/2,82ms, flip angle = 15°, T2prep = 40 ms, TI = 100 ms. Image acquisition was ECG‐triggered and during diastolic quiescent period. The volume of IMH was determined using cvi42 (Circle Cardiovascular Imaging, Calgary, Alberta, Canada).Results
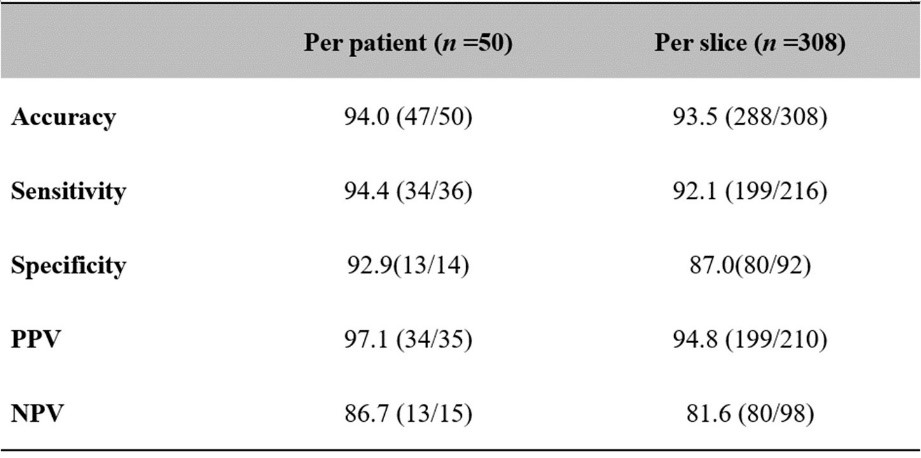
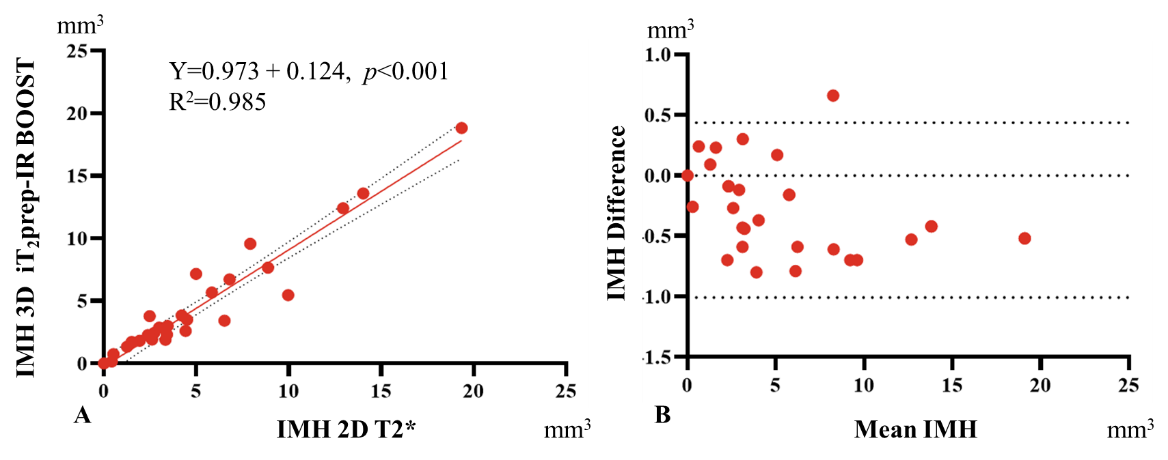
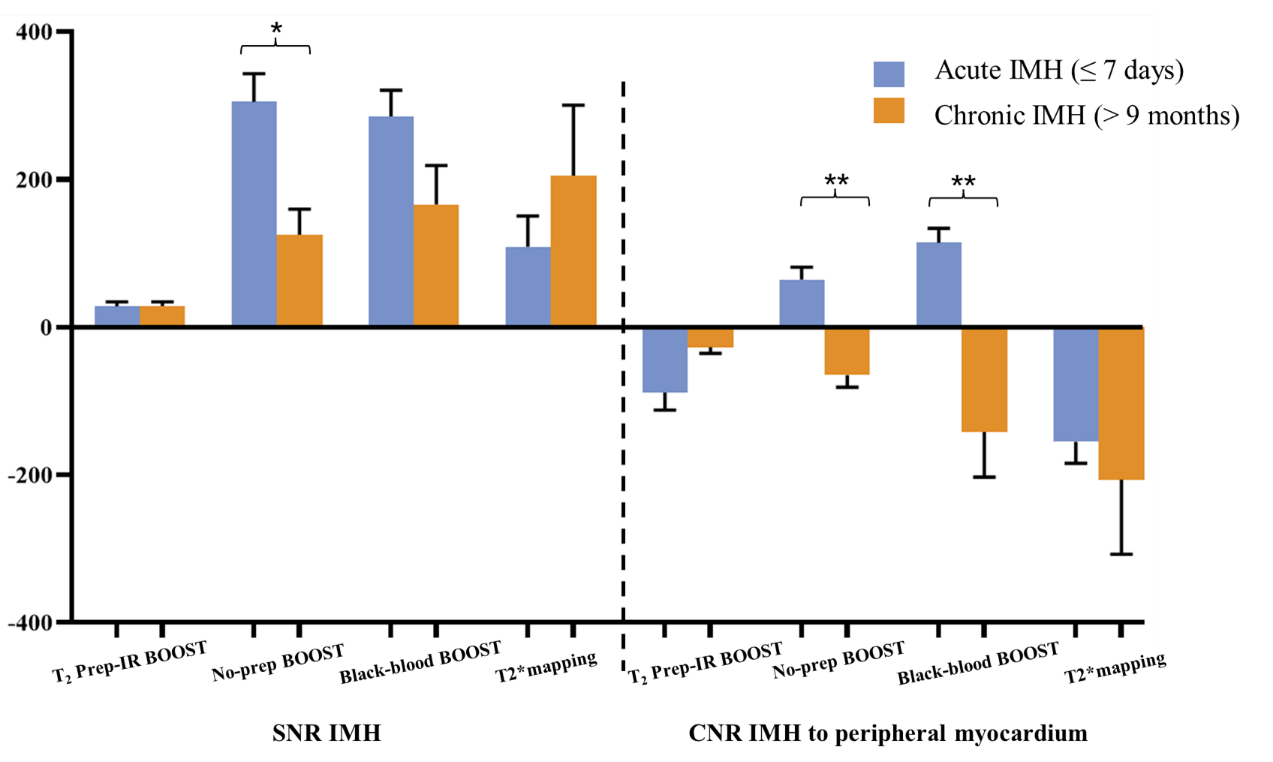
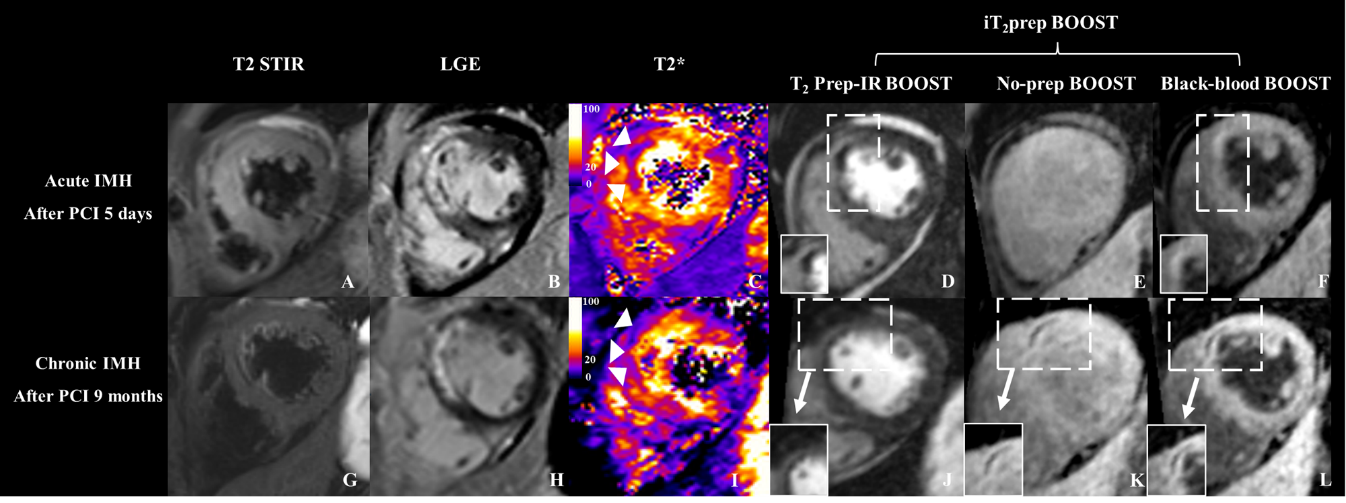
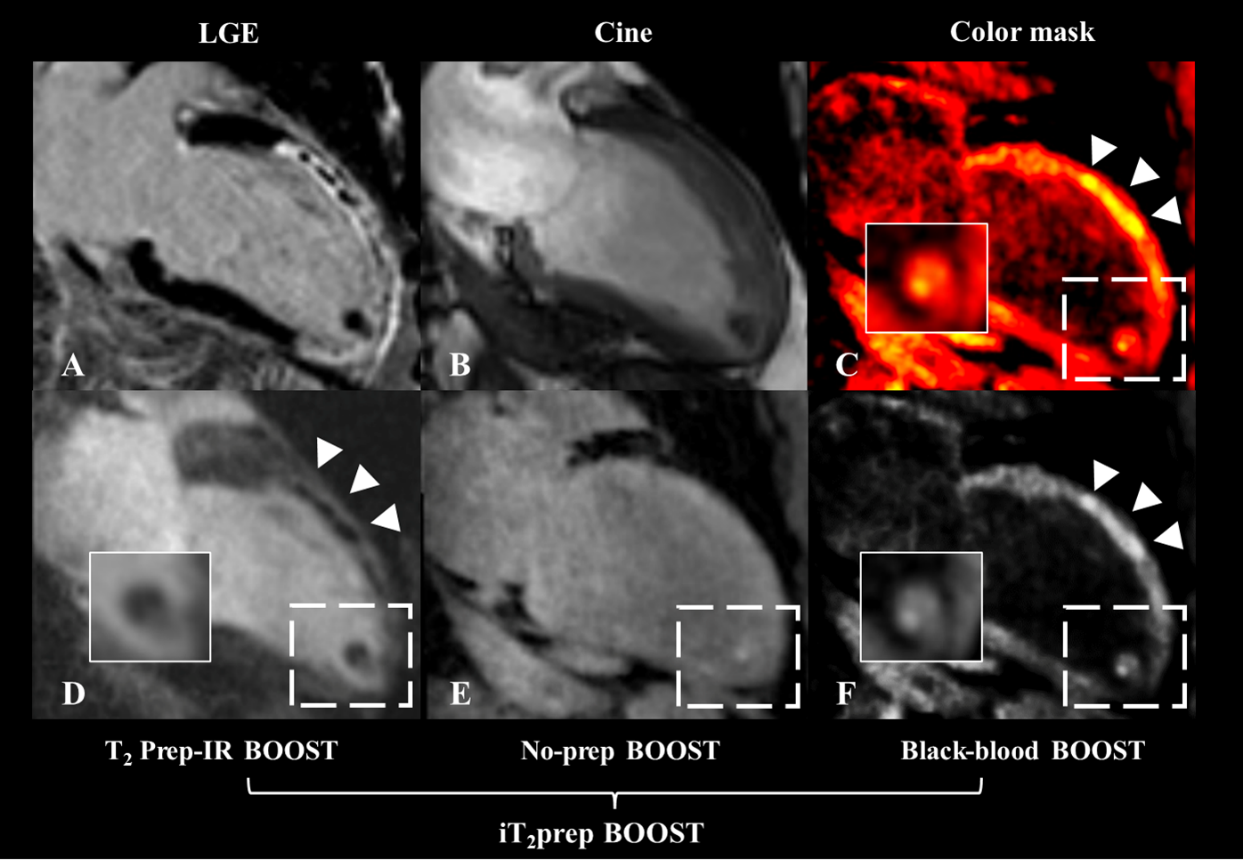
Forty patients (age: 54±12 years; 38 men) with first ST elevation myocardial infarction (STEMI) who underwent successful percutaneous transluminal coronary intervention (PCI) underwent CMR within 7 days after PCI. Ten patients (age: 54±11 years; 10 men) underwent a second CMR scan 9 months later. Fifty patient images were included in the statistical analysis. Qualitative analysis revealed that iT2prep‐IR BOOST had 94% sensitivity and 93% specificity for IMH. Across 308 assessable myocardium levels, iT2prep‐IR BOOST had 92% sensitivity and 87% specificity for IMH (Figure 1). Quantitative analysis showed a strong correlation (regression line: Y=0.97 + 0.12, p<0.001) (Figure 2) between iT2prep‐IR BOOST and T2* mapping in IMH volume measurements. Additionally, acute IMH exhibited low signal intensity on T2prep-IR BOOST images and slightly increased signal intensity on no-prep BOOST and black-blood BOOST. During our follow-up examination of patients with chronic IMH (9 months later), we observed low signal intensity on all three contrast-weighted images. Acute and chronic IMH displayed significant differences in no-prep and black-blood BOOST (p<0.001) (Figure 3). However, this characteristic was not evident on T2* mapping. Figure 4 shows a representative case of IMH in acute and chronic stages. Figure 5 shows a representative case of IMH with apical thrombus. Mixed signals from apical thrombi were observed in patients with anterior myocardial infarction, which could be associated with the thrombus phase and composition.Discussion
This study showed that the iT2prep-IR BOOST sequence provides non-enhanced, multi-contrast 3D whole-heart visualization of IMH in patients with STEMI on a 3T scanner. First, iT2prep-IR BOOST sequence relies on its multi-contrast imaging, demonstrating its ability to stage IMH in a manner that cannot be achieved with T2* mapping. Previous studies of IMH staging primarily focused on the period of myocardial infarction4. However, our method allows direct observation of IMH signal evolution at various time points. In this study, patients with residual IMH lesions at 9 months exhibited a gradual decrease in cardiac function, which may be related to persistent myocardial inflammation caused by hemosiderin deposits5. Second, iT2prep-IR BOOST provides a superior representation of IMH compared with T2* mapping. In T2*-weighted magnetic resonance images, IMH tissue displays lower regional signal intensity because of magnetic changes involving hemoglobin degradation products. However, IMH occurs adjacent to edema, which substantially increases T2-relaxation, while T2 in IMH zones is known to be significantly shortened early after MI2. The iT2prep-IR BOOST magnetic resonance imaging sequence with GRE-Dixon readout can capture information about both T2 and T2* during the first heartbeat and T1 and T2* during the second heartbeat. When there is increased swelling or fluid accumulation in the heart muscle (i.e., edema), this imaging method shows greater signal differences between regions of reperfusion-induced injury and unaffected healthy tissue. Furthermore, the iT2prep-IR BOOST sequence does not require breath-holding, and, being an isotropic-resolution 3D whole-heart sequence, is expected to have a high sensitivity for thrombus detection.Conclusion
iT2prep‐IR BOOST for IMH detection at 3T exhibits higher sensitivity and specificity, along with good quantitative consistency, relative to T2* mapping alone. Furthermore, iT2prep‐IR BOOST has substantial potential for visualization in IMH and LVT staging.Acknowledgements
We thank the Scientific Research Department of the Siemens Company for invaluable technical support.References
1. Liu T, Howarth AG, Chen Y, Nair AR, Yang HJ, Ren D, et al. Intramyocardial hemorrhage and the "wave front" of reperfusion injury compromising myocardial salvage. J Am Coll Cardiol. 2022;79:35-48
2. Payne AR, Berry C, Kellman P, Anderson R, Hsu LY, Chen MY, et al. Bright-blood t(2)-weighted mri has high diagnostic accuracy for myocardial hemorrhage in myocardial infarction: A preclinical validation study in swine. Circ Cardiovasc Imaging. 2011;4:738-745
3. Milotta G, Ginami G, Cruz G, Neji R, Prieto C, Botnar RM. Simultaneous 3d whole-heart bright-blood and black blood imaging for cardiovascular anatomy and wall assessment with interleaved t(2) prep-ir. Magn Reson Med. 2019;82:312-325
4. Wang G, Yang HJ, Kali A, Cokic I, Tang R, Xie G, et al. Influence of myocardial hemorrhage on staging of reperfused myocardial infarctions with t(2) cardiac magnetic resonance imaging: Insights into the dependence on infarction type with ex vivo validation. JACC Cardiovasc Imaging. 2019;12:693-703
5. Bulluck H, Rosmini S, Abdel-Gadir A, White SK, Bhuva AN, Treibel TA, et al. Residual myocardial iron following intramyocardial hemorrhage during the convalescent phase of reperfused st-segment-elevation myocardial infarction and adverse left ventricular remodeling. Circ Cardiovasc Imaging. 2016;9:e004940
Figures