1174
Quantification of Cyclical Changes in Myocardial Blood Volume Using a Hybrid 3D/2D Sequence with Ferumoxytol-enhanced MRI1Laboratory for Translational Imaging of Microcirculation, Krannert Cardiovascular Research Center, Indiana University School of Medicine, Indianapolis, IN, United States, 2Krannert Cardiovascular Research Center, Indiana University School of Medicine, Indianapolis, IN, United States
Synopsis
Keywords: Myocardium, Pulse Sequence Design, myocardial blood volume, ferumoxytol
Motivation: Intramyocardial blood volume (iMBV) variations during cardiac cycle can be an important marker for detecting ischemic heart disease. However, quantifying the change in iMBV from diastole to systole under MRI has challenges such as through-plane motion or in-flow of unsaturated spins.
Goal(s): Our goal is to perform accurate quantification of iMBV variations from diastole to systole.
Approach: We developed a novel hybrid 3D/2D pulse sequence with continuous golden-angle radial acquisition to suppress the confounding factors for distinguishing diastolic and systolic iMBV.
Results: Our approach successfully showed that cyclic variations in iMBV can be correctly quantified under ferumoxytol-enhanced MRI.
Impact: We introduced, for the first time, an approach to quantify cyclic systolic and diastolic intramyocardial blood volume variations at rest on a clinical scanner with ferumoxytol-enhanced imaging. Our method has the potential to be used for detecting ischemic heart disease
Introduction
Intramyocardial blood volume (iMBV) provides important information about the health of coronary microcirculation and its change, from resting state to pharmacological or exercise stress, can be used as a biomarker for detecting ischemic heart disease.1-3 Preclinical studies have shown that iMBV changes during the cardiac cycle primarily due to the mechanical forces in the systolic contraction phase.4,5 Recent work with nuclear (SPECT) imaging has shown that the cyclic dynamics of iMBV change from its peak at end-diastole (ED) to its trough at end-systole (ES) can be quantified noninvasively in humans with potential clinical applications.6 MRI-based investigation of cyclic iMBV dynamics, however, has so far been limited to small animals using non-clinical scanners and investigational contrast agents that are not commercially available. Here we introduce, for the first time, an approach that can be readily translated to a clinical setting. Specifically, we propose a novel hybrid 3D/2D pulse sequence without magnetization preparation using radial spoiled GRE (SPGR) readouts to quantify cyclic ED-to-ES iMBV variations on a clinical scanner with Ferumoxytol-enhanced imaging.Methods
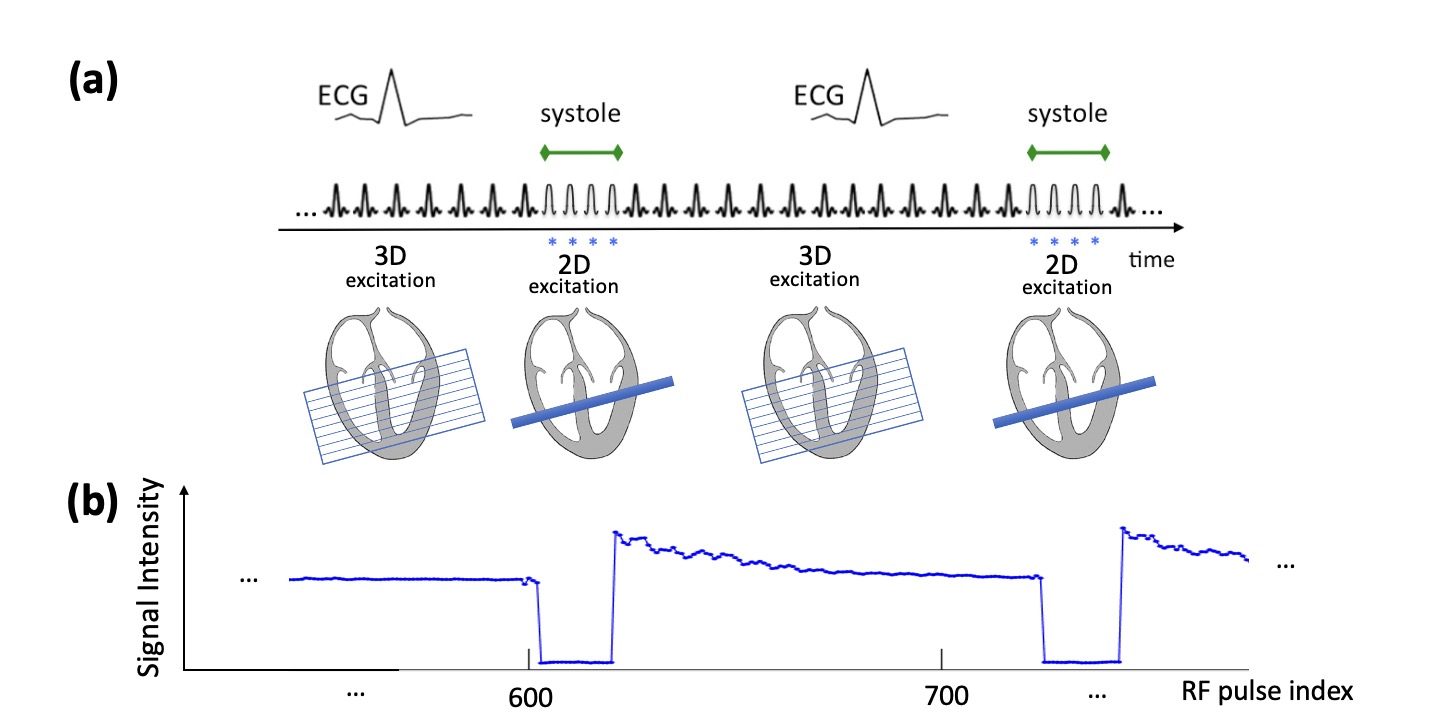
The T1-weighted signal in fast SPGR sequences is confounded by through-plane motion and in-flow effects. To overcome these, we developed a "hybrid" SPGR sequence consisting of slice-exciting (2D) and slab-exciting (3D) RF pulses with continuous golden-angle radial acquisition (3T Siemens scanner). As shown in Fig. 1(a), the sequence switches between 2D and 3D pulses based on a user-defined “2D imaging” interval that is synchronized with the R-wave to enable ES (Fig. 1) or ED imaging (not shown). Of note, as shown in Fig 1(b), the 3D pulses in the designed sequence ensure that the out-of-slice magnetization (which is disrupted due the switching to 2D excitation) returns to steady state before the next 2D-imaging interval. To generate T1 maps with our sequence, we acquired images with low flip angle (FA), primarily proton-density weighted, and high FA (T1-weighted), and used a look-up table (Bloch equation simulations). Notably, the low FA images were used to normalize the high FA image which, in turn, eliminates T2*- and coil-weighting effects as part of the T1 fitting process. To verify the accuracy of our T1 mapping technique, we conducted phantom studies (Ferumoxytol -doped agar bottles). Next, we acquired in-vivo data in pigs (n=10) before and after Ferumoxytol infusion (single short-axis slice; resolution: 1.4x1.4x8 mm3) to estimate iMBV maps from separate ES and ED scans.7 For comparison, we also acquired MOLLI T1 maps at systolic and diastolic phases to estimate MOLLI-derived iMBV maps for each phase.Results
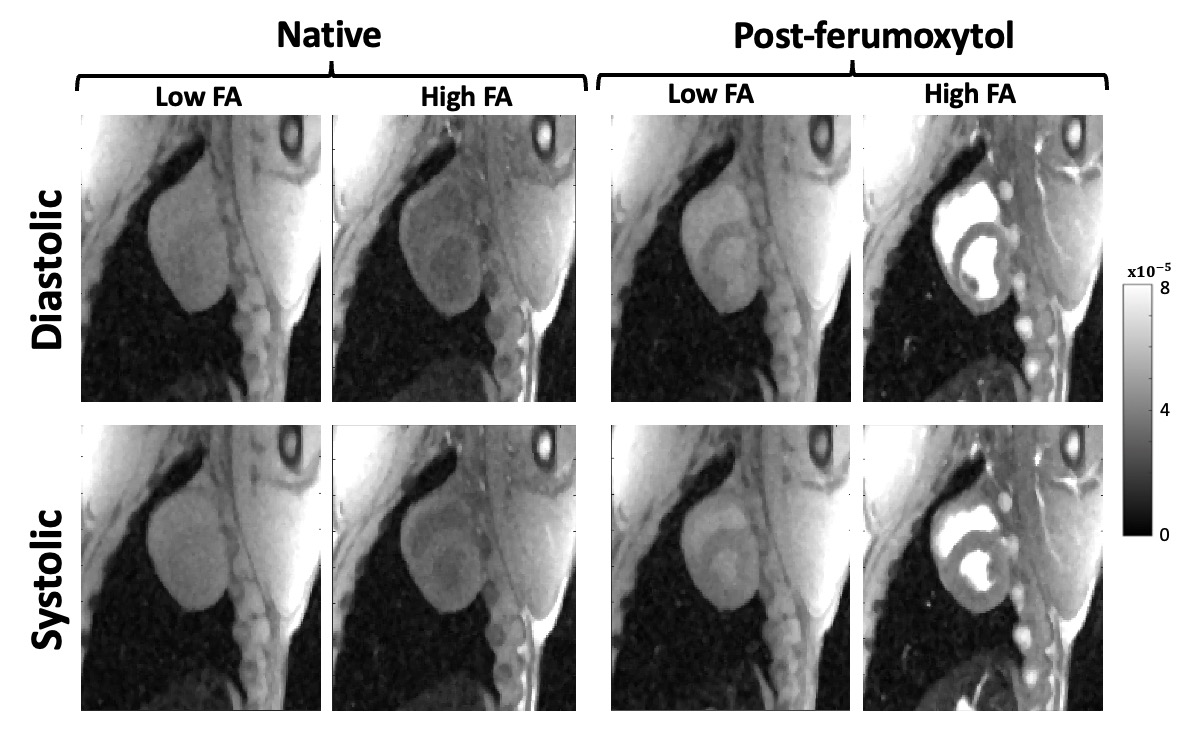
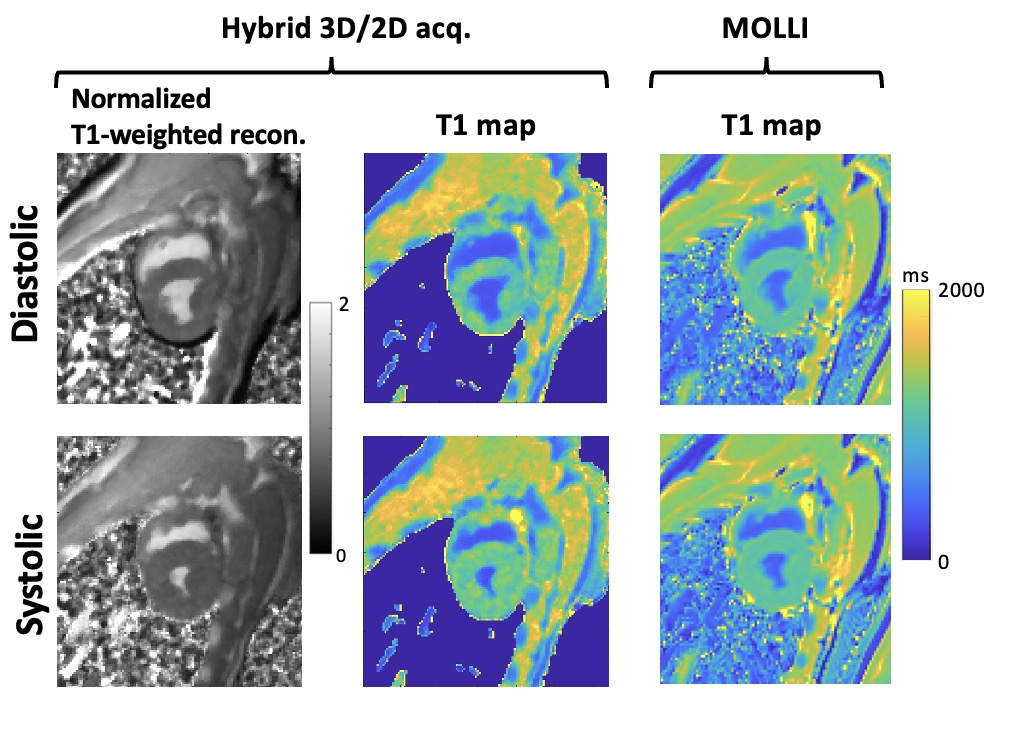
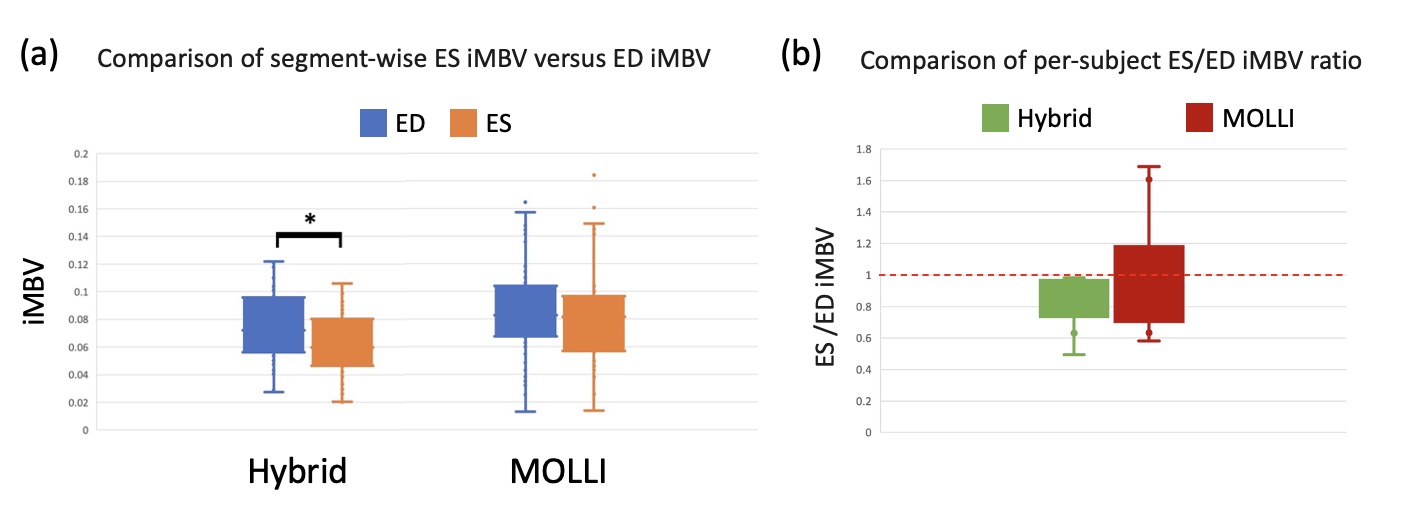
Phantom results showed a strong correlation between T1 values derived using the proposed hybrid 3D/2D sequence and MOLLI (R2 = 0.92, p < 10-4). Figure 2 shows representative images for ED and ES phases before and after Ferumoxytol infusion. Figure 3 shows another representative case with the normalized high FA image for the hybrid method (left column) and corresponding post-Ferumoxytol T1 maps for both the hybrid method and MOLLI. A summary of the systolic/diastolic iMBV values is shown in Figure 4. With segment-wise analysis, the proposed method resulted in a significant difference between iMBV at ED versus ES (ED = 7.7±2.7%, ES = 6.2 ±2.2%, p < 10-4) whereas MOLLI-derived iMBV did not show a significant difference (ED = 8.6±3.6%, ES = 8.1±3.2%, p = 0.3). Moreover, the hybrid method consistently showed ES iMBV (mean value for the acquired slice) to be lower than ED iMBV (as expected from physiology) whereas, for MOLLI-derived values, ES iMBV was higher than ED for 3 of the 10 studies.Discussion
Our results indicate that the proposed hybrid 3D/2D SPGR approach is capable of capturing “instantaneous” T1 maps thanks to its steady-state T1 contrast which, in turn, enables it to quantify iMBV at a specific cardiac phase. Our results show on average 19.5% drop in iMBV from ED to ES which is consistent with recent SPECT studies.5,6 In contrast, MOLLI-derived iMBV did not show a significant difference between ES iMBV versus ED iMBV. This can be attributed to the fact that, unlike the proposed method which uses steady-state contrast that can capture “instantaneous” T1 maps, the magnetization preparation pulses in MOLLI effectively “mix” the T1-weighting between ES and ED phases regardless of whether the readout occurs in ES or ED. Unlike prior work in this area, our proposed ES/ED iMBV quantification method has the advantage that it can be readily translated to a clinical setting since it uses Ferumoxytol as the intravascular agent and has been implemented and tested on a clinical scanner with promising results, showing the ES/ED differences in the expected physiologic range.Acknowledgements
This work was supported by the NIH grant R01-HL153430 and the Lilly Endowment INCITE award.References
1. McCommis KS, Goldstein TA, Zhang H, Misselwitz B, Gropler RJ, Zheng J. Quantification of myocardial blood volume during dipyridamole and doubtamine stress: a perfusion CMR study. J Cardiovasc Magn Reson. 2007;9:785-792. doi: 10.1080/10976640701545206
2. van Assen M, van Dijk R, Kuijpers D, Vliegenthart R, Oudkerk M. T1 reactivity as an imaging biomarker in myocardial tissue characterization discriminating normal, ischemic and infarcted myocardium. Int J Cardiovasc Imaging. 2019;35:1319-1325. doi: 10.1007/s10554-019-01554-4
3. Colbert CM, Le AH, Shao J, Currier JW, Ajijola OA, Hu P, Nguyen KL. Ferumoxytol-enhanced magnetic resonance T1 reactivity for depiction of myocardial hypoperfusion. NMR Biomed. 2021;34:e4518. doi: 10.1002/nbm.4518
4. Judd RM, Levy BI. Effects of barium-induced cardiac contraction on large- and small-vessel intramyocardial blood volume. Circ Res. 1991;68:217-225. doi: 10.1161/01.res.68.1.217
5. Mohy-Ud-Din H, Boutagy NE, Stendahl JC, Zhuang ZW, Sinusas AJ, Liu C. Quantification of intramyocardial blood volume with (99m)Tc-RBC SPECT-CT imaging: A preclinical study. J Nucl Cardiol. 2018;25:2096-2111. doi: 10.1007/s12350-017-0970-4
6. Yousefi H, Shi L, Soufer A, Tsatkin V, Bruni W, Avendano R, Greco K, McMahon D, Thorn S, Miller E, et al. Quantification of intramyocardial blood volume using (99m)Tc-RBC SPECT/CT: a pilot human study. J Nucl Cardiol. 2023;30:292-297. doi: 10.1007/s12350-022-03123-0
7. Donahue KM, Weisskoff RM, Chesler DA, Kwong KK, Bogdanov AA, Jr., Mandeville JB, Rosen BR. Improving MR quantification of regional blood volume with intravascular T1 contrast agents: accuracy, precision, and water exchange. Magn Reson Med. 1996;36:858-867. doi: 10.1002/mrm.1910360608
Figures