1173
High Multiband Factor Highly Accelerated Whole Heart SMILE Perfusion1Cardiovascular Medicine, Stanford University, Stanford, CA, United States
Synopsis
Keywords: Myocardium, Perfusion, SMS, CAIPIRINHA
Motivation: Clinical cardiac perfusion captures a limited number of slices sequentially within each heartbeat, causing incomplete left ventricle coverage and potential quantification variability due to different cardiac phases.
Goal(s): To image multiple slices simultaneously thereby reducing quantification variability and improve heart coverage.
Approach: We apply highly accelerated Simultaneous Multi-slice Imaging via Linear phase modulated Extended field of view (SMILE) acquisition and reconstruction framework to cardiac perfusion.
Results: With a high multiband factor and accelerated rate, SMILE perfusion achieve whole heart coverage and allows for more slices to be in the same cardiac phase. Retrospective and prospective experiments validated its good quality.
Impact: The proposed methods can significantly enhance the heart coverage of clinical cardiac perfusion and potentially benefit reducing variability in quantitative perfusion assessment.
Introduction
Simultaneous multi-slice imaging enjoys volumetric imaging SNR efficiency and is advantageous for time-critical applications[1]. We have previously introduced a novel SMS framework called Simultaneous Multi-slice Imaging via Linear phase modulated Extended field of view (SMILE)[2,3], which adopts an extended field of view along the phase encoding direction enabling standard parallel-imaging-based reconstruction. Our previous work demonstrated that SMILE can provide bias-free and content-independent reconstruction with a theoretical guarantee, eliminating slice leakage, as long as the calibration region and reconstruction method adopt the appropriate k-space kernel size.In conventional cardiac perfusion imaging, a limited number of single-slice images are acquired sequentially within each heartbeat. Even with a small multiband factor (MB) in SMS, images are collected throughout the cardiac cycle to cover the entire heart. Using a higher MB can expand cardiac perfusion coverage, capturing more images during the same cardiac phase, potentially reducing image quantification variability across different cardiac cycle phases[4].
Methods
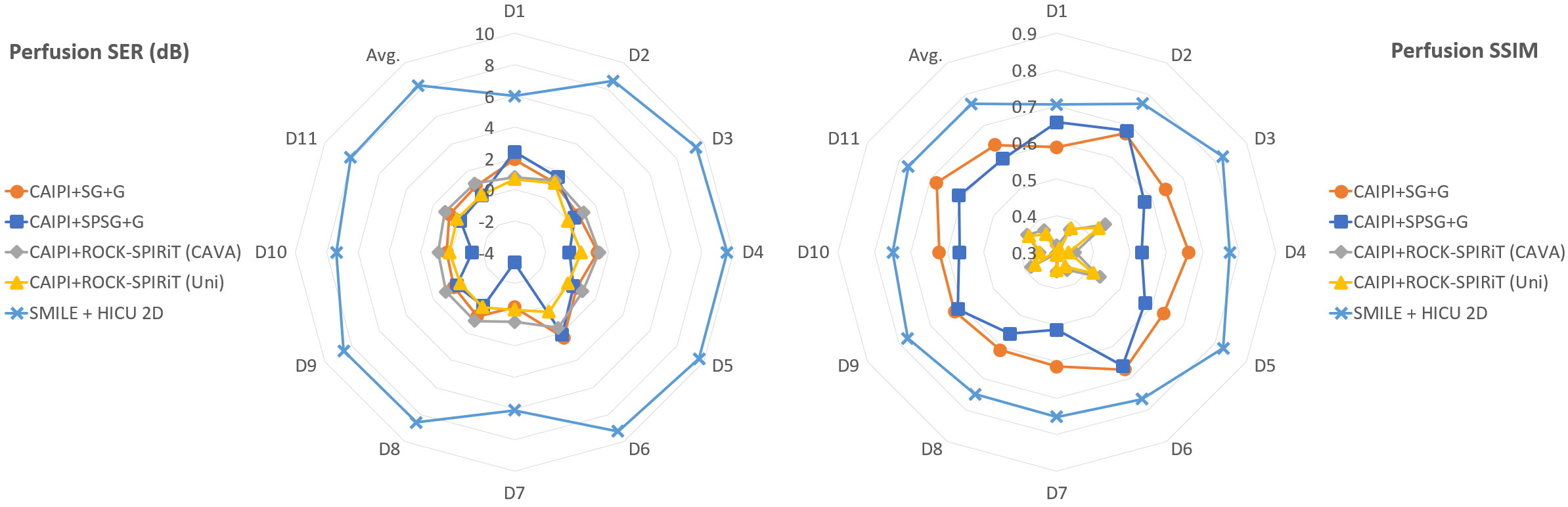
Retrospectively downsampled perfusion study: 11 patient perfusion datasets (D1~D11) comprising five slices, with R=2 uniformly downsampling were collected. Per frame HICU[5] reconstruction (HICU 2D) served as ground truth. The calibration data acquired for each slice were transformed for use in conventional SMS acquisition with CAIPIRINHA phase modulation and SMILE acquisition. Both CAIPIRINHA and SMILE had a simulated net acceleration of R=10. For CAIPIRINHA, R equates to the multiband (MB) factor times in-plane acceleration rate, while for SMILE, R represents total in-plane acceleration. The reconstruction methods include Slice GRAPPA (SG)[6], Split-Slice GRAPPA (SPSG)[7], ROCK-SPIRIT[8], and HICU. SG and SPSG were exclusively compatible with uniform downsampling and were followed by in-plane GRAPPA reconstruction (G). For other reconstruction methods, we also utilized a variable density sampling CAVA[9]. Images were compared based on reconstruction signal to error ratio (SER) and structural similarity index (SSIM), where SER is defined as $$$\frac{ \|\hat{\mathbb{K}} - \mathbb{K} \|_\textsf{F}}{\|\mathbb{K}\|_\textsf{F}}$$$, $$$\hat{\mathbb{K}}$$$ is the reconstructed k-space and $$$\|\cdot\|_\textsf{F}$$$ denotes Frobenius norm.Prospectively downsampled perfusion study: We performed SMILE perfusion imaging on 8 patients using a 3T Siemens Skyra Scanner, with MB = 5 and net R = 10. We acquired 10 slices with 1.5 mm in-plane resolution for whole-heart coverage using the CAVA pattern. Images were reconstructed using 2D+t HICU reconstruction (HICU). Temporal fidelity was assessed with per-frame 2D HICU reconstruction (HICU 2D), considered as the gold standard as per-frame reconstruction should not disrupt temporal fidelity. Images were graded by a cardiologist on a 5-point scale (1 poor to 5 excellent).
Results
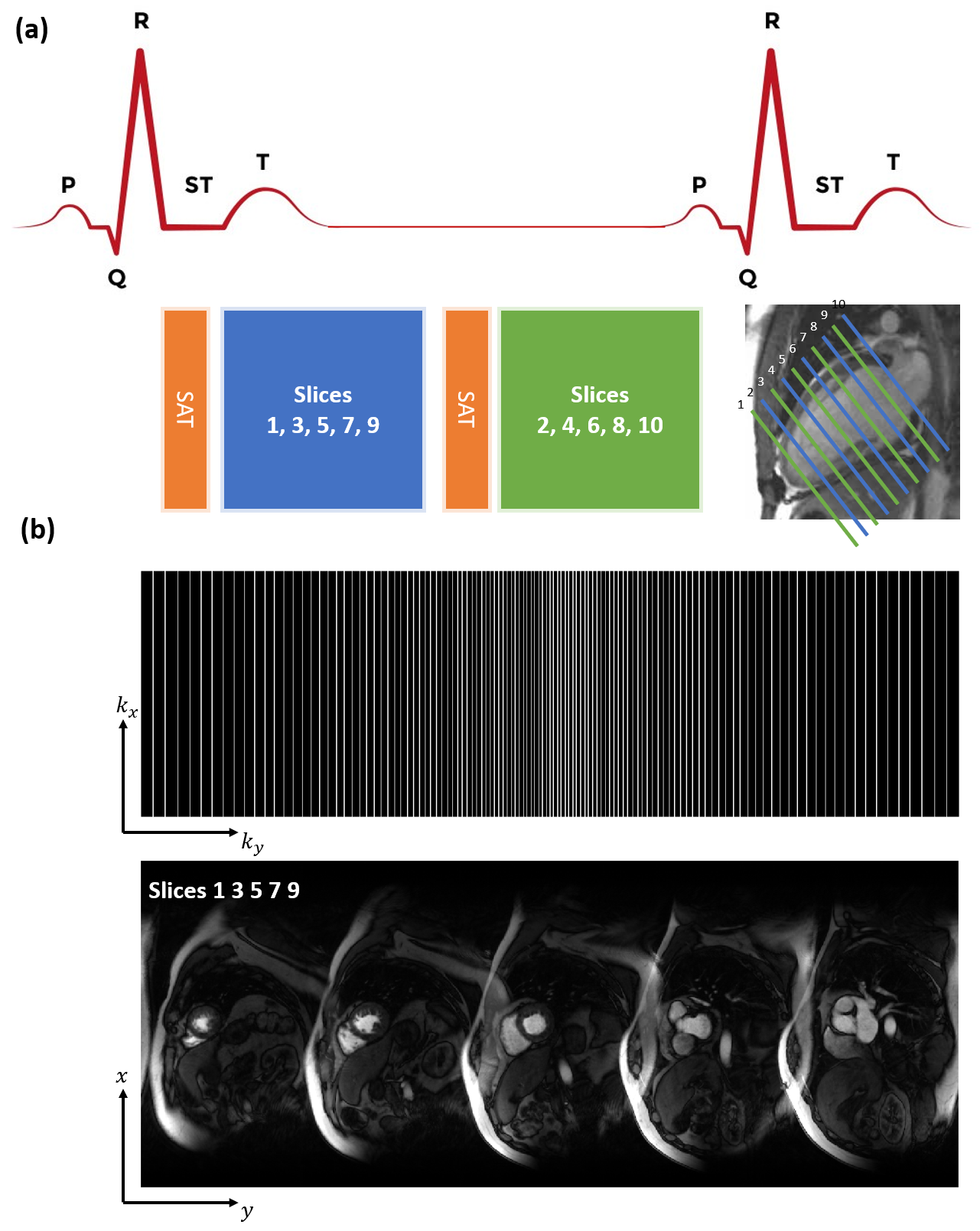
Figure.1 depicts the SMILE perfusion acquisition pipeline for a MB=5 acquisition.Figure.2 shows the radar plots of SER and SSIM, SMILE + HICU 2D reaches the highest reconstruction quality in both metrics.
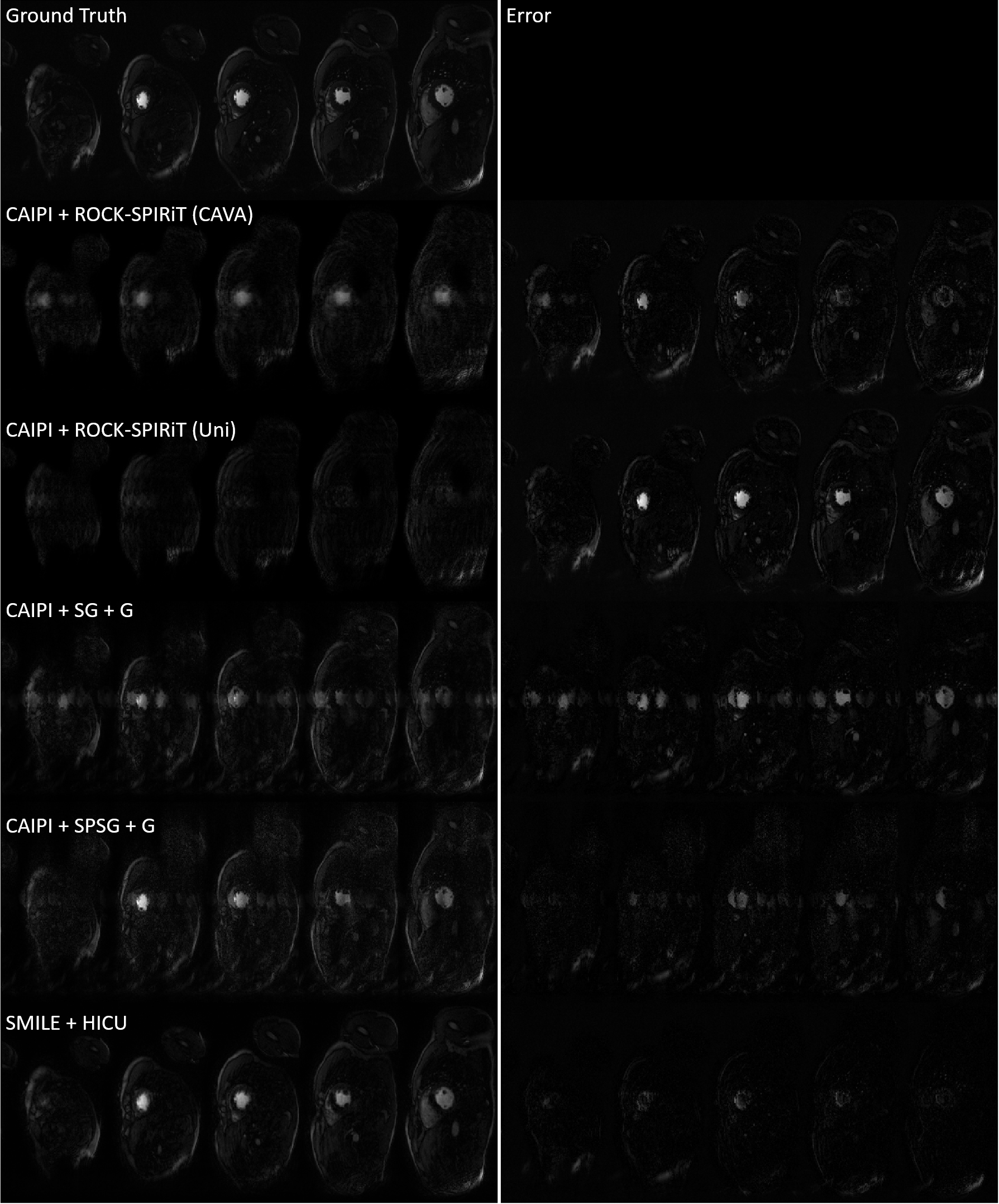
Figure.3 shows one representative frame comparing the reconstruction results of different acquisition and reconstruction combinations. We can observe severe slice leakage for CAIPIRINHA regardless of the reconstruction methods.
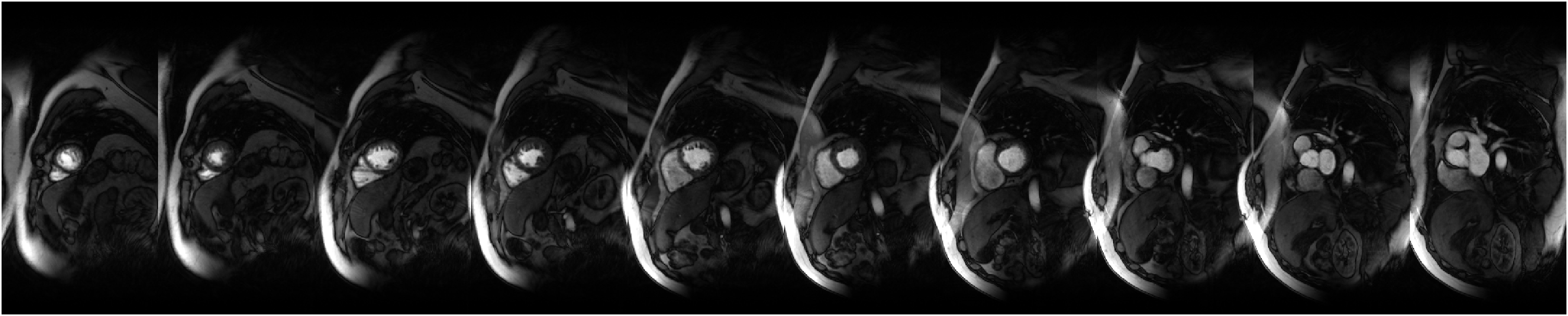
Figure.4 shows one of the representative frames of prospectively undersampled SMILE perfusion at MB=5, R=10. Two slice groups of 5 slices within one heartbeat are reorganized following apical to basal direction to be horizontally concatenated for illustration.
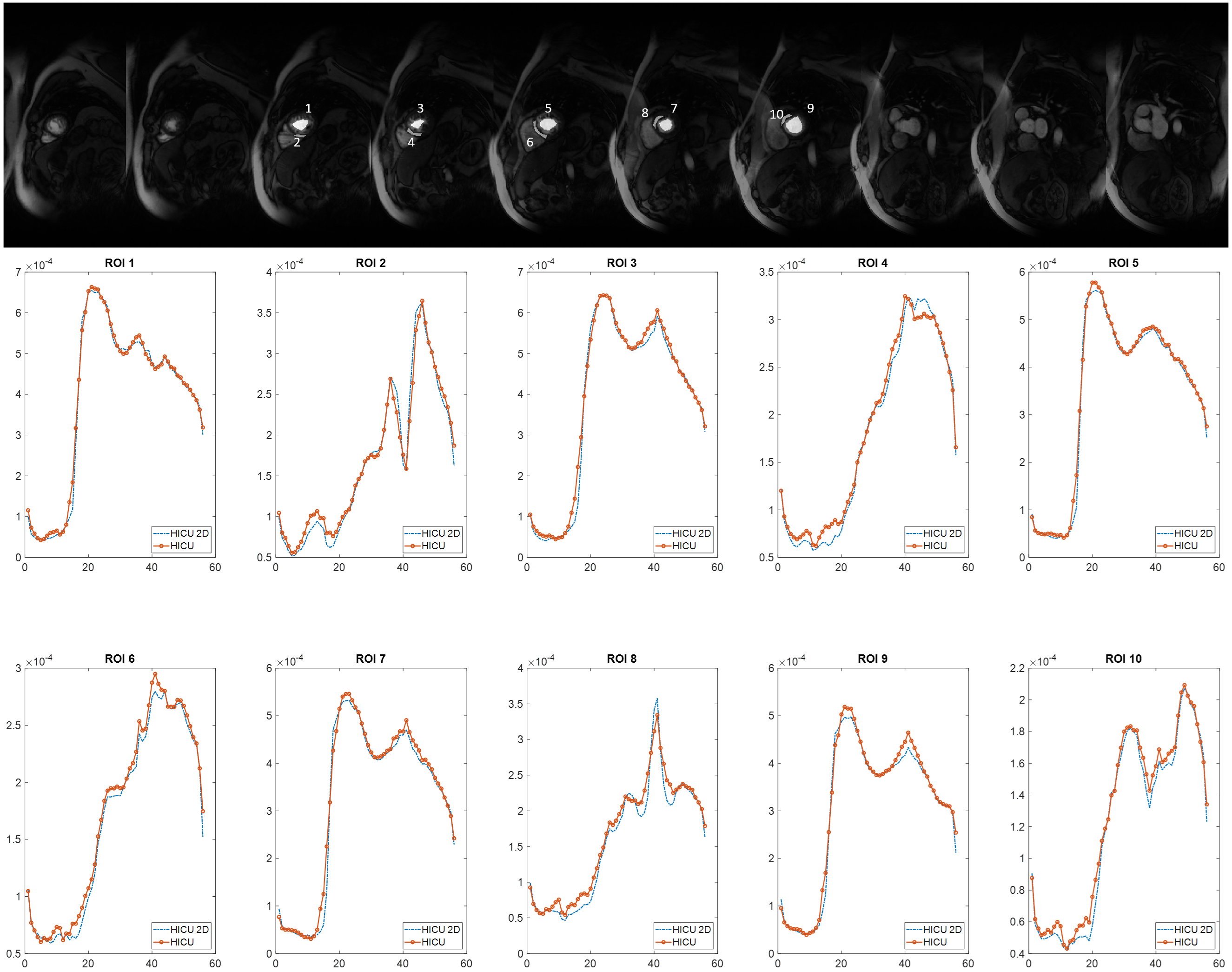
Figure.5 shows the temporal fidelity of the 2D+t HICU reconstruction compared with HICU 2D, of different regions of interest (ROI), HICU reconstruction is of good agreement with the HICU 2D reconstruction in terms of temporal fidelity. Image quality scores for the 8 HICU reconstruction is 4.1 $$$\pm$$$ 0.6.
Discussion and Conclusions
Perfusion imaging presents challenges for SMS due to significant signal intensity changes between perfusion frames and calibration data. Notably, there is pronounced slice leakage in frames acquired before the contrast agent arrives for CAIPIRINHA acquisition. However, experimental validation has shown that SMILE perfusion, even with high multiband factors and substantial acceleration rates and variable density sampling pattern, produces high-quality images without slice leakage, allowing for comprehensive coverage of the entire heart. This approach enables the acquisition of five slices during a single phase of the cardiac cycle, facilitating future quantitative perfusion analysis.Acknowledgements
This project is funded by NIH R01 HL131919, NIH R01 HL155962-01.References
1. Barth, Markus, et al. "Simultaneous multislice (SMS) imaging techniques." Magnetic resonance in medicine 75.1 (2016): 63-81.
2. Zhao, S., Wang, X., Wang, J., Salerno, M. “Simultaneous Multislice Imaging via Linear Phase Modulated Extended Field of View (SMILE) for Cardiac Cine and Perfusion.” Proc. 26th SCMR Scientific Session. 2023
3. Zhao, S., Wang, J., Salerno, M. “Accelerated Simultaneous Multislice Imaging via Linear Phase Modulated Extended Field of View (SMILE)” Proc. 32nd ISMRM Meeting & Exhibition, Toronto, Canada, 2023, p. 0869.
4. Motwani, Manish, et al. "Quantitative three-dimensional cardiovascular magnetic resonance myocardial perfusion imaging in systole and diastole." Journal of Cardiovascular Magnetic Resonance 16 (2014): 1-11.
5. Zhao, Shen, Lee C. Potter, and Rizwan Ahmad. "High‐dimensional fast convolutional framework (HICU) for calibrationless MRI." Magnetic Resonance in Medicine 86.3 (2021): 1212-1225.
6. Setsompop, Kawin, et al. "Blipped‐controlled aliasing in parallel imaging for simultaneous multislice echo planar imaging with reduced g‐factor penalty." Magnetic resonance in medicine 67.5 (2012): 1210-1224.
7. Cauley, Stephen F., et al. "Interslice leakage artifact reduction technique for simultaneous multislice acquisitions." Magnetic resonance in medicine 72.1 (2014): 93-102.
8. Demirel, Omer Burak, et al. "Improved simultaneous multislice cardiac MRI using readout concatenated k‐space SPIRiT (ROCK‐SPIRiT)." Magnetic resonance in medicine 85.6 (2021): 3036-3048.
9. Rich, Adam, et al. "CArtesian sampling with Variable density and Adjustable temporal resolution (CAVA)." Magnetic resonance in medicine 83.6 (2020): 2015-2025.
Figures