1169
Prospective Determination of Tumor Regression Grade with Magnetic Resonance Imaging in Neoadjuvant Chemotherapy for Rectal Adenocarcinoma1Colorectal Cancer Center, Department of General Surgery, West China Hospital, Chendu, China, 2Department of Radiology, West China Hospital, Chendu, China
Synopsis
Keywords: Cancer, Cancer, Rectal cancer; Neoadjuvant chemotherapy; Complete response; Magnetic resonance tumor regression grade; Diffusion-weighted imaging.
Motivation: The role of MRI in evaluating the tumor response following neoadjuvant chemotherapy (NCT) in rectal cancers remains pending.
Goal(s): To investigate the reliability of MRI in assessing the pathological clinical response (pCR) in rectal cancer patients with NCT.
Approach: In two consecutive prospective clinical trials (Clinicaltrials.gov NCT03666442 and NCT04922853), tumor responses to NCT were evaluated using MRI-based models.
Results: 224 patients were enrolled. MR-TRG, DWI, DWImodMR-TRG mriCR, and rNAR score were all associated with pCR. DWImodMR-TRG achieved the highest area under the curve (AUC) of 0.940, with the highest sensitivity of 0.905 and the highest PPV of 0.976.
Impact: MRI-based models were feasible in determining the tumor response in LARC patients following NCT. DWI may improve the predictive performance of MR-TRG. Our findings provide evidence for the determination of tumor response for rectal cancer patients who underwent NCT.
Introduction
Neoadjuvant chemotherapy (NCT) has become increasingly acceptable in the management of local advanced rectal cancer (LARC) without high-risk factors.1-4 However, the role of MRI in evaluating the tumor response following NCT remains pending. This study aimed to investigate the reliability of MRI in assessing the pathological clinical response (pCR) in LARC patients with NCT.Methods
We conducted an imaging substudy within two consecutive prospective clinical trials, the expanded phase II trial (Clinicaltrials.gov NCT03666442)5 and the COPEC trial (Clinicaltrials.gov NCT04922853).6 A surgeon and a radiologist blinded to the clinicopathologic data independently evaluated the tumor response using 5 methods, including magnetic resonance tumor regression grade (MR-TRG) alone, diffusion-weighted imaging (DWI) alone, DWI-modified MR-TRG (DWImodMR-TRG), MRI complete response (mriCR), and radiologic neoadjuvant response (rNAR) score. With pCR serving as the reference, the performance of those methods was tested with positive predictive value (PPV), negative predictive value (NPV), sensitivity, specificity, and receiver operating characteristics (ROC) curves.Restults
A total of 224 patients were enrolled, including 119 from the expanded phase II trial and 105 patients from the COPEC trial. The overall mriCR rate of included patients was 21.9% (49/224), with 23.5% (28/119) in the expanded phase II trial and 20.0% (21/105) in the 4-cycle COPEC group. MR-TRG, DWI, DWImodMR-TRG mriCR, and rNAR score were all associated with pCR (r = 0.526, 0.465, 0.611, 0.714, and 0.350, respectively; p < 0.001). Regarding the performance of different MRI-based tumor response models, the areas under the curve (AUC) were 0.940, 0.898, 0.878 and 0.775 for DWImodMR-TRG, MR-TRG alone, mriCR and DWI alone, respectively. Paired comparisons of different MRI-based tumor response models showed that the DWImodMR-TRG performed outperformance compared with other models, with the highest sensitivity of 0.905 and the highest PPV of 0.976.Discussion
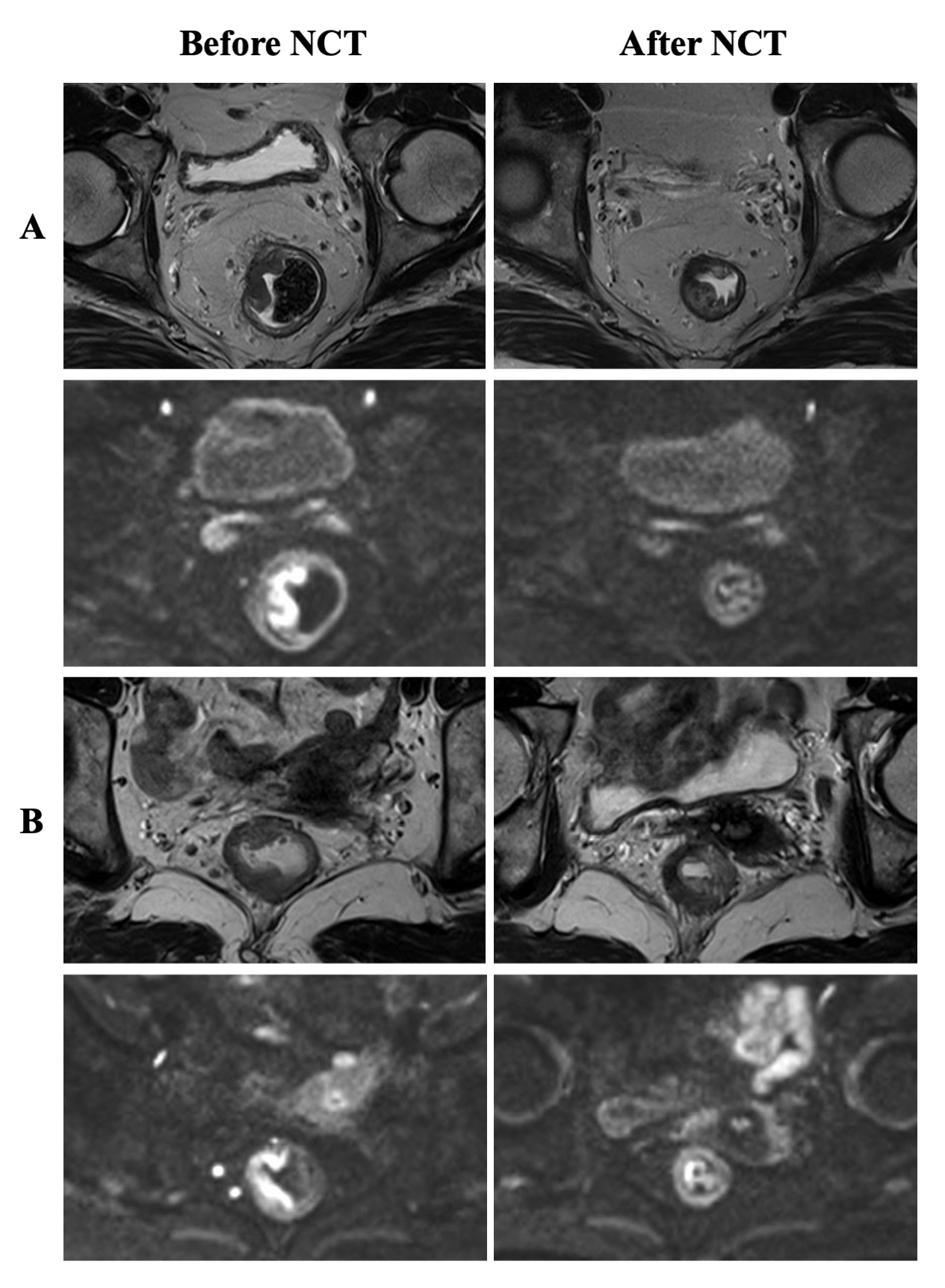
Like NRG-GI002 substudy7, all tested MRI-based tumor response models show a remarkably high specificity and PPV, suggesting that MRI has an almost unquestionable ability to identify tumor remnants. The summarized PPV of MR-TRG in determining pCR was 0.828 in two prospective studies, which is almost double compared to the recently reported 42% in the NRG-GI002 substudy7. We speculate that the gap difference lies in the variation of neoadjuvant treatment strategies since the NRG-GI002 substudy mentioned that multiple radiologists reached similar conclusions after chemotherapy alone and less agreement after radiotherapy. Radiotherapy may lead to significant tumor fibrosis, which brings difficulties in differentiating the radiological stages based on T2 imaging.8 Previous study reported that T2-weighted MRI tends to overestimate the presence of tumor residual, mainly because when the completely regressed bowel shows an atypical mixed signal (typically it shows a dark homogeneous fibrotic aspect), it may mislead radiologists to interpret the thickening at the former tumor location as a residual tumor.9 This may also explain why one-third of pCR were distinguished as MR-TRG2 in the current study.DWI imaging can help to differentiate between scar bowel wall and residual tumor, as tissues with diffusion restriction are suspicious for the presence of residual tumors.10A meta-analysis reporting assessment of rectal tumor response to chemoradiotherapy showed that the addition of DWI significantly improved the sensitivity of cCR determination from 50% with T2 sequence alone to 84% with DWI.11 Among 49 patients who were interpreted as mriCR, MR-TRG (mainly based on T2 sequences) identified 28 cases (57.1%) while DWI identified 45 cases (91.8%), indicating that the addition of DWI can help avoid missing mriCR after NCT. However, we still recognized 5 pCR patients as residual focal diffusion signal abnormalities (DWI positive) and 6 pCR patients as DWI uncertain. Perhaps this can be partly explained by the persisting T2 signals from the rental wall which failed to be entirely suppressed on DWI imaging or the potential histological reactive changes such as ulcers which may also cause a false high signal on DWI.9
We further explored the combination of T2 and DWI sequences for modifications of the MRI-based tumor response models. DWImodMR-TRG integrated the advantages of two regression modes and reduced the possible misinterpretation of potential mriCR as tumor residual. By recognition of restricted diffusion on additional DWI sequences, the misclassified MR-TRG2 may downgraded to DWImodMR-TRG1 and reclassified as a complete response. In this way, DWImodMR-TRG improved the sensitivity from 0.571 to 0.905 and performed best in the relevant 4 MRI-based tumor response models with an AUC of 0.940, which is even higher than the previously reported 0.874 in a retrospective study including patients with LARC treated with NCRT.12
Conclusion
MRI-based models were feasible in determining tumor response in LARC patients following NCT. DWI may have the potential to improve the predictive performance of MR-TRG.Acknowledgements
This work was supported by the National Natural Science Foundation of China (82103541, 82203474 and 82203394), Department of Science and Technology of Sichuan Province (No. 2022YFS0162, 2021YFS0025 and 2022YFS0209), 1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University (No. 20HXJS003 and ZYJC21017), 1·3·5 project for disciplines of excellence-Clinical Research Incubation Project, and West China Hospital, Sichuan University (No. 22HXFH001 and 2019HXFH031).References
1. Taylor FG, Quirke P, Heald RJ, Moran B, Blomqvist L, et al. Preoperative high-resolution magnetic resonance imaging can identify good prognosis stage I, II, and III rectal cancer best managed by surgery alone: a prospective, multicenter, European study. Annals of surgery 2011:253:711-719.
2. Bossé D, Mercer J, Raissouni S, Dennis K, Goodwin R, et al. PROSPECT Eligibility and Clinical Outcomes: Results From the Pan-Canadian Rectal Cancer Consortium. Clin. Colorectal Cancer 2016:15:243-249.
3. Deng X, Liu P, Jiang D, Wei M, Wang X, et al. Neoadjuvant Radiotherapy Versus Surgery Alone for Stage II/III Mid-low Rectal Cancer With or Without High-risk Factors: A Prospective Multicenter Stratified Randomized Trial. Annals of surgery 2020:272:1060-1069.
4. Schrag D, Shi Q, Weiser MR, Gollub MJ, Saltz LB, et al. Preoperative Treatment of Locally Advanced Rectal Cancer. N. Engl. J. Med. 2023.
5. Shen Y, Wu Q, Meng W, Wei M, Deng X, et al. Neoadjuvant chemotherapy (CAPOX) alone for low- and intermediate-risk stage II/III rectal cancer: Long-term follow-up of a prospective single-arm study. Eur. J. Surg. Oncol. 2023:49:107115.
6. Shen Y, Shi W, Huang C, Gong X, Wei M, et al. Comparison of the pathological response to 2 or 4 cycles of neoadjuvant CAPOX in II/III rectal cancer patients with low/intermediate risks: study protocol for a prospective, non-inferior, randomized control trial (COPEC trial). Trials 2023:24:397.
7. Hall WA, Li J, You YN, Gollub MJ, Grajo JR, et al. Prospective Correlation of Magnetic Resonance Tumor Regression Grade With Pathologic Outcomes in Total Neoadjuvant Therapy for Rectal Adenocarcinoma. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 2023:Jco2202525.
8. Pang X, Xie P, Yu L, Chen H, Zheng J, et al. A new magnetic resonance imaging tumour response grading scheme for locally advanced rectal cancer. Br. J. Cancer 2022:127:268-277.
9. van der Sande ME, Beets GL, Hupkens BJ, Breukink SO, Melenhorst J, et al. Response assessment after (chemo)radiotherapy for rectal cancer: Why are we missing complete responses with MRI and endoscopy? European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology 2019:45:1011-1017.
10. Lambregts DM, Vandecaveye V, Barbaro B, Bakers FC, Lambrecht M, et al. Diffusion-weighted MRI for selection of complete responders after chemoradiation for locally advanced rectal cancer: a multicenter study. Annals of surgical oncology 2011:18:2224-2231.
11. van der Paardt MP, Zagers MB, Beets-Tan RG, Stoker J, Bipat S Patients who undergo preoperative chemoradiotherapy for locally advanced rectal cancer restaged by using diagnostic MR imaging: a systematic review and meta-analysis. Radiology 2013:269:101-112.
12. Chandramohan A, Siddiqi UM, Mittal R, Eapen A, Jesudason MR, et al. Diffusion weighted imaging improves diagnostic ability of MRI for determining complete response to neoadjuvant therapy in locally advanced rectal cancer. Eur J Radiol Open 2020:7:100223.
Figures