1159
Abnormal Cerebral Blood Flow, Brain Volume, Microstructural Tissue Changes in Pediatric Obstructive Sleep Apnea1Anesthesiology, University of California Los Angeles, Los Angeles, CA, United States, 2Head and Neck Surgery, University of California Los Angeles, Los Angeles, CA, United States
Synopsis
Keywords: Neuro, Arterial spin labelling
Motivation: OSA Children show cognitive and behavioral impairments along with brain tissue changes. The status of CBF, which may contribute to brain changes impacting cognitive and behavioral issues in pediatric OSA, is unknown.
Goal(s): Our goal was to examine CBF, brain volume, and microstructural changes in pediatric OSA and evaluate associations between CBF, cognition, and behavioral issues.
Approach: We used ANCOVA to compare CBF and brain tissue changes between OSA and controls, and partial correlations for associations.
Results: We observed reduced CBF in pediatric-OSA and associations of CBF with behavioral and cognitive issues, which may contribute to OSA pathogenesis.
Impact: This study showed altered cerebral blood flow and its associations with abnormal behavioral and cognitive functions in children with OSA, which have never been studied before. The reduced regional flow may lead to further neural damage in the condition.
Purpose
Pediatric obstructive sleep apnea (OSA) is associated with poor neurocognitive performance and behavioral issues. Brain morphological changes and microstructural tissue changes have been reported in children with OSA,1-6 but the pathophysiological mechanisms contributing to altered gray matter volume and microstructural tissue changes in pediatric OSA are unclear. Altered cerebral blood flow (CBF), which can be assessed by MRI based arterial spin labeling (ASL) imaging procedures, may contribute to volumetric and brain tissue changes, mitigating cognitive and behavioral issues in the condition. ASL imaging is a non-invasive approach for assessment of regional brain perfusion changes and has not been used in the evaluation of CBF in pediatric OSA. Voxel-based morphometry (VBM), an automatic quantitative technique, allows whole-brain voxel-wise comparisons of gray matter (GM) volumes between groups. In addition, T2-relaxometry measures free-water content within the tissue by acquiring a series of images at different echo times, and has the potential to detect brain tissue microstructural changes. Our aim was to examine regional CBF (ASL), regional brain volume, and microstructural tissue changes in children with OSA compared to healthy controls and evaluate associations between CBF status and cognition and behavioral issues.Materials and methods
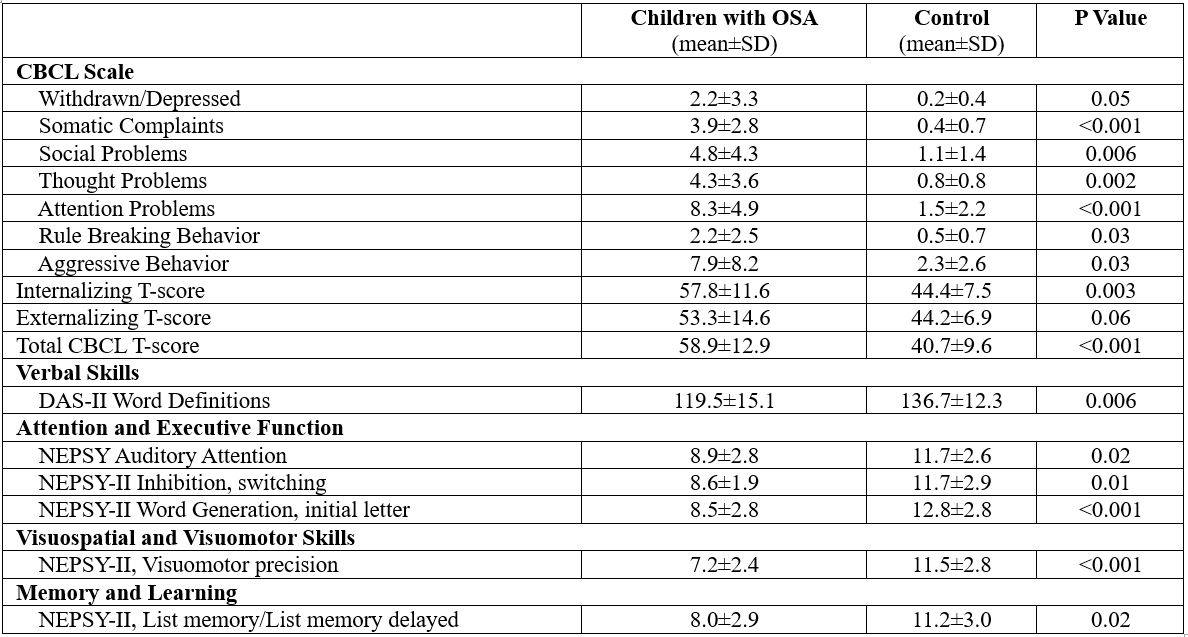
We examined 13 children with OSA (age, 8.7±1.2 years; body-mass-index (BMI), 24.3±5.9 kg/m2; 10 male; apnea-hypopnea index, 5.9±6.2 events/hour), and 11 healthy controls (age, 9.4±1.2 years; BMI, 17.9±0.8 kg/m2; 8 female) using a 3.0-Tesla MRI (Magnetom Prisma Fit; Siemens). Behavioral problems were assessed by the Child Behavior Checklist (CBCL) and cognition status through NEPSY (Developmental Neuropsychological Assessment) and DAS-II (Differential Abilities Scales, 2nd edition). High-resolution T1-weighted image series was collected using the magnetization-prepared rapid acquisition gradient-echo pulse sequence [TR=2200ms; TE=2.41ms; inversion time=900 ms; FA= 9°; matrix size=320×320; FOV=230×230mm2; slice thickness=0.9mm)]. Proton density (PD) and T2-weighted images were acquired using a dual-echo turbo spin-echo sequence in the axial plane [TR=10,000 ms; TE1, TE2=12, 124 ms; FA=130°; matrix size=256 × 256; FOV=230 × 230 mm; slice thickness=3.5 mm; inter-slice gap=no]. 3D pseudo-continuous ASL [pCASL] (TR=4,000 ms, TE= 6.7 ms, FA=120°, bandwidth=2365 Hz/pixel, matrix size=96×96, FOV=240×240 mm, slice thickness=2.5 mm) data were collected. High-resolution T1-weighted images were partitioned into gray matter, white matter, and cerebrospinal fluid (CSF) tissue types and DARTEL toolbox was used to normalize and smooth GM maps. Using PD and T2-weighted images, whole-brain pixel-by-pixel T2-relaxation values were calculated, normalized, and smoothed. The labeled and non-labeled ASL brain volumes were used to compute perfusion images and whole-brain CBF maps and were normalized and smoothed. The smoothed GM maps, T2-relaxation, and CBF maps were compared between groups using analysis of covariance (ANCOVA, SPM12; covariates, age and sex). Also, whole-brain CBF maps were correlated voxel-by-voxel with CBCL, DAS-II, and NEPSY scores in children with OSA using partial correlations (SPM12; covariates, age and sex).Results
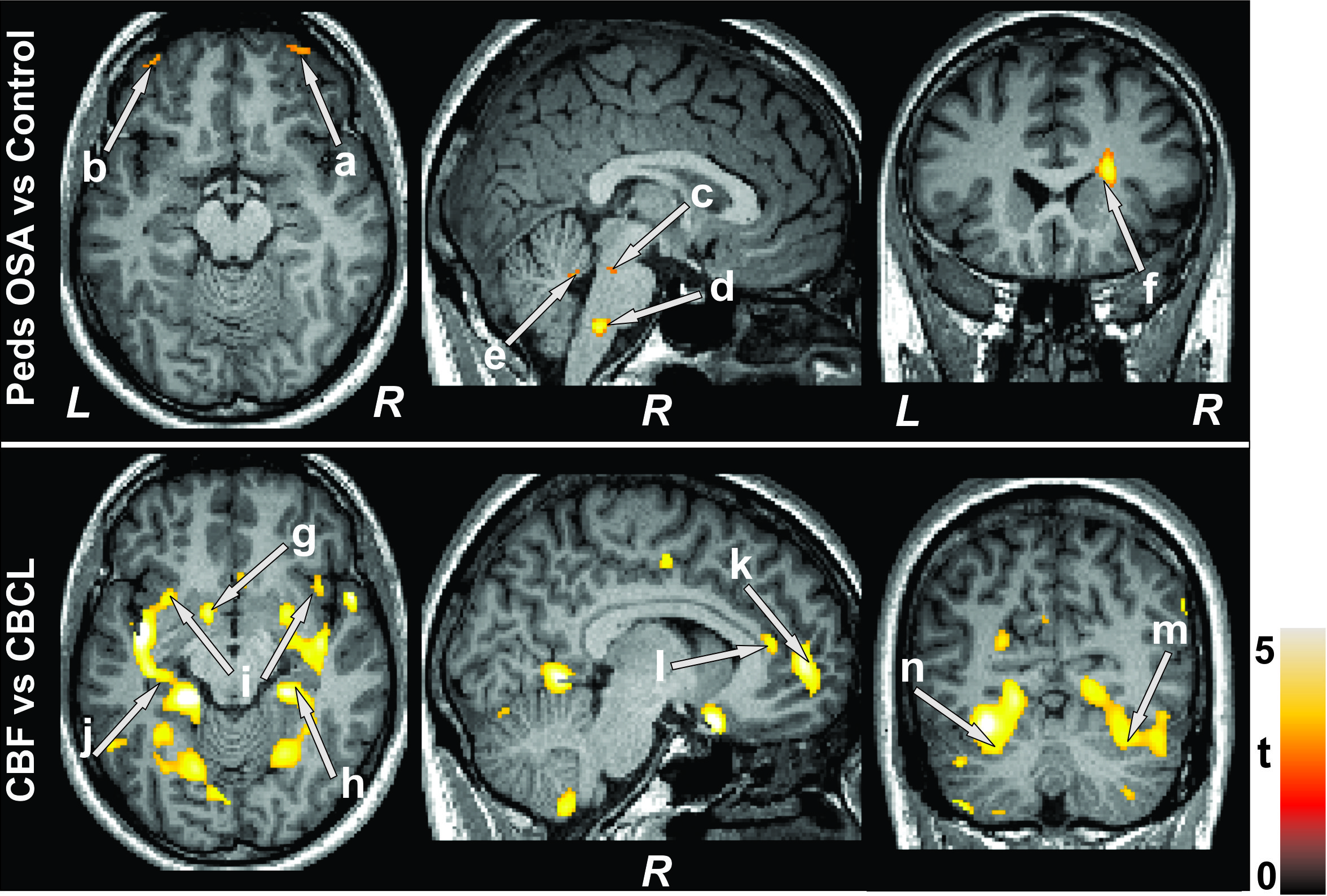
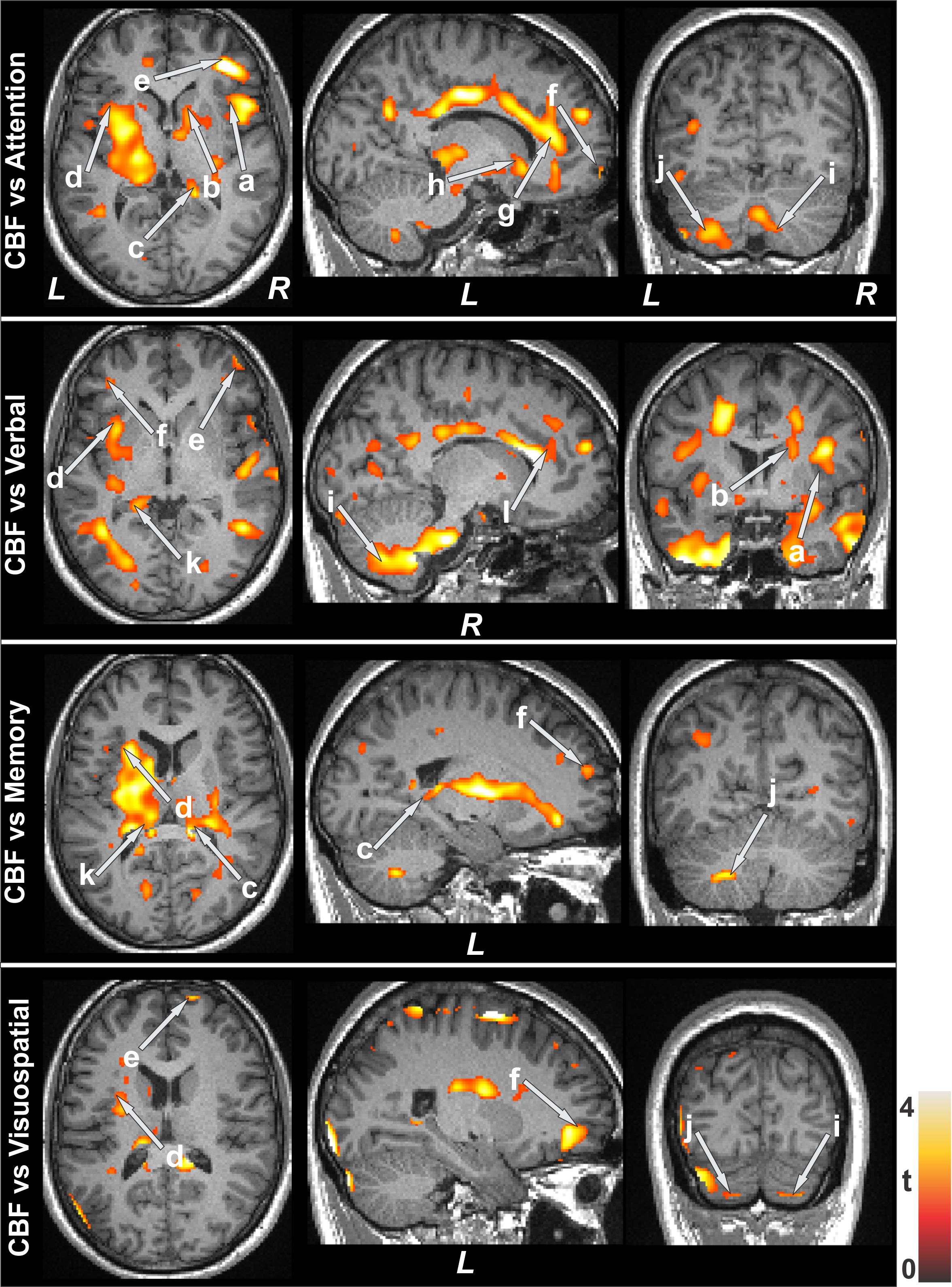
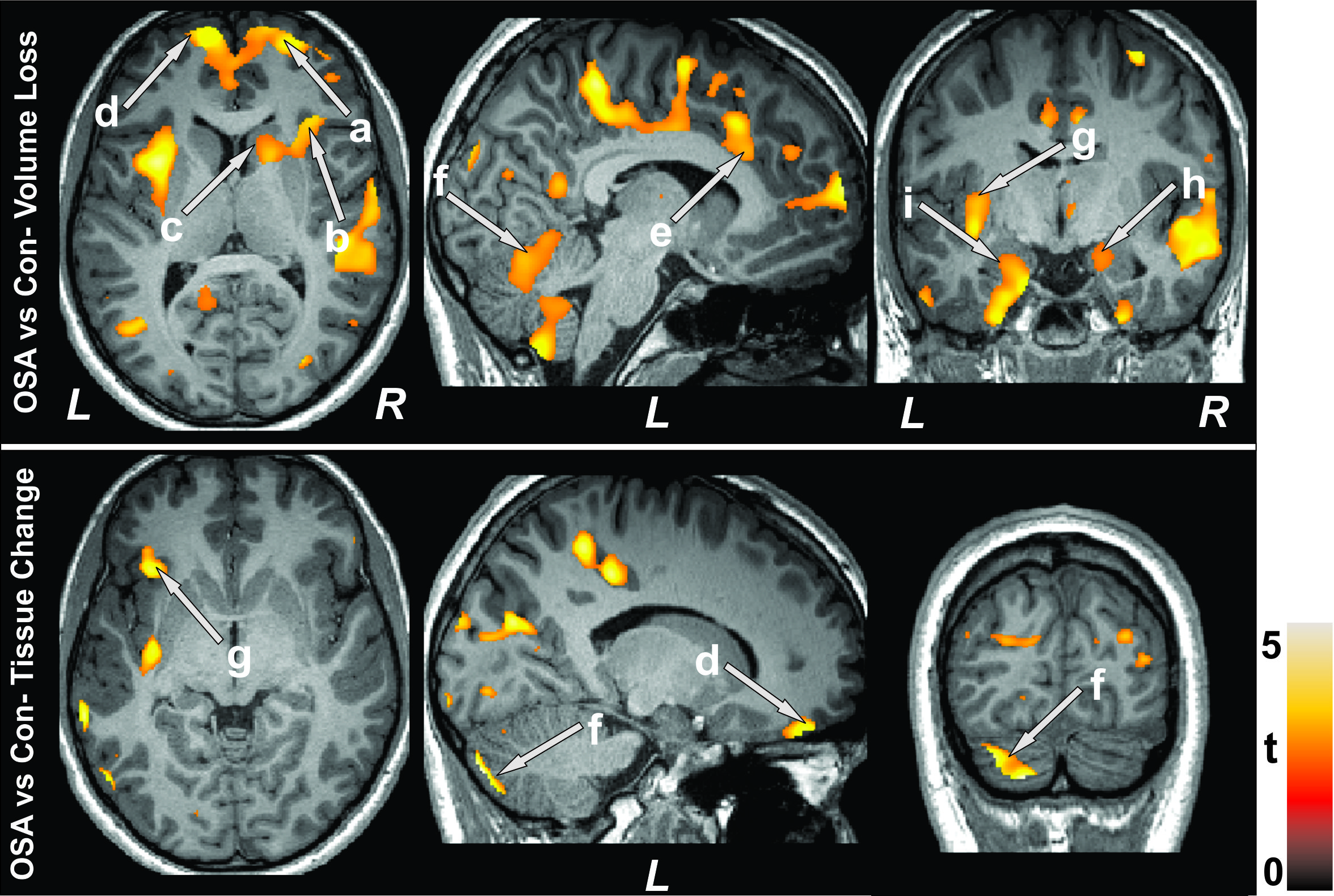
Children with OSA showed behavioral issues and cognitive deficits in multiple domains (Fig.1). Reduced CBF was observed in children with OSA compared to control subjects (Fig.2) in several areas, including the prefrontal cortices, pons, brain stem, cerebellum, and caudate. Also, increased CBF was noticed in some brain regions. Cognitive sub-domains, including attention, verbal, memory, and visuospatial were positively correlated with CBF in pediatric OSA in the insula, caudate, hippocampus, prefrontal cortices, anterior cingulate, and cerebellum (Fig. 3). Negative associations were found between CBF and total CBCL scores in children with OSA in the prefrontal cortices, cerebellum, caudate, hippocampus, insular cortices, and anterior cingulate (Fig 2). Multiple brain areas showed reduced gray matter volumes and microstructural tissue changes in children with OSA, including the prefrontal cortices, insula, caudate, anterior cingulate, cerebellum, and hippocampus (Fig. 4).Discussion
Children with OSA showed predominantly reduced CBF and was associated with behavioral and cognitive issues. Some sites showed increased CBF, which might be due to acute hypoxia changes that stimulate cerebral vasodilation and increases CBF as a compensatory mechanism. The results suggested that reduced CBF and reduce GM volume and tissue changes are mainly located in the prefrontal cortices, insula, caudate, anterior cingulate, cerebellum, and hippocampus, areas that mediate closely in behavioral and cognition functions.Conclusions
This study suggested that children with OSA had reduced CBF, particularly in the prefrontal cortices and cerebellum, and were closely related to abnormal behavior and cognitive functions, which may contribute to the pathogenesis of OSA. The reduced CBF, and altered GM volume and tissue changes may be caused by hypoxia, which could lead to abnormal cognitive function and psychological status. Also, the increased CBF may be a compensatory response to the volume reduction and tissue changes in pediatric OSA.Acknowledgements
This work was supported by National Institutes of Health R21 HD102544-01A1.References
1. Philby MF, Macey PM, Ma RA, et al. Reduced regional grey matter volumes in pediatric obstructive sleep apnea. Sci Rep.2017;7:44566.
2. Macey PM, Kheirandish-Gozal L, Prasad JP, et al. Altered regional brain cortical thickness in pediatric obstructive sleep apnea. Front Neurol. 2018;9:4.
3. Musso MF, Lindsey HM, Wilde EA, et al. Volumetric brain magnetic resonance imaging analysis in children with obstructive sleep apnea. Int J Pediatr Otorhinolaryngol. 2020;138:110369.
4. Isaiah A, Ernst T, Cloak C, et al. Associations between frontal lobe structure, parent-reported obstructive sleep disordered breathing and childhood behavior in the ABCD dataset. Nat Commun.2021;12:2205.
5. Cha J, Zea-Hernandez JA, Sin S, et al. The effects of obstructive sleep apnea syndrome on the dentate gyrus and learning and memory in children. J Neurosci. 2017;37:4280–8.
6. Horne RSC, Roy B, Walter LM, et al. Regional brain tissue changes and associations with disease severity in children with sleep-disordered breathing. Sleep. 2018;41:zsx203.
Figures