1156
A Quantitative and Non-Invasive MR-based Method to Analyze Ventricular Shunt Flow in Patients with Hydrocephalus1Neurosurgery, Children's Hospital Los Angeles, Los Angeles, CA, United States, 2Pediatrics, Children's Hospital Los Angeles, Los Angeles, CA, United States, 3Radiology, Children's Hospital Los Angeles, Los Angeles, CA, United States, 4Children's Hospital Los Angeles, Los Angeles, CA, United States
Synopsis
Keywords: Neuro, Brain, shunt, hydrocephalus
Motivation: We investigate a new approach to evaluating ventricular shunt function using phase-contrast magnetic resonance imaging (PC-MRI).
Goal(s): Our goal was to demonstrate the rapid (96-second) sequence as a practical adjunct for determining shunt function non-invasively.
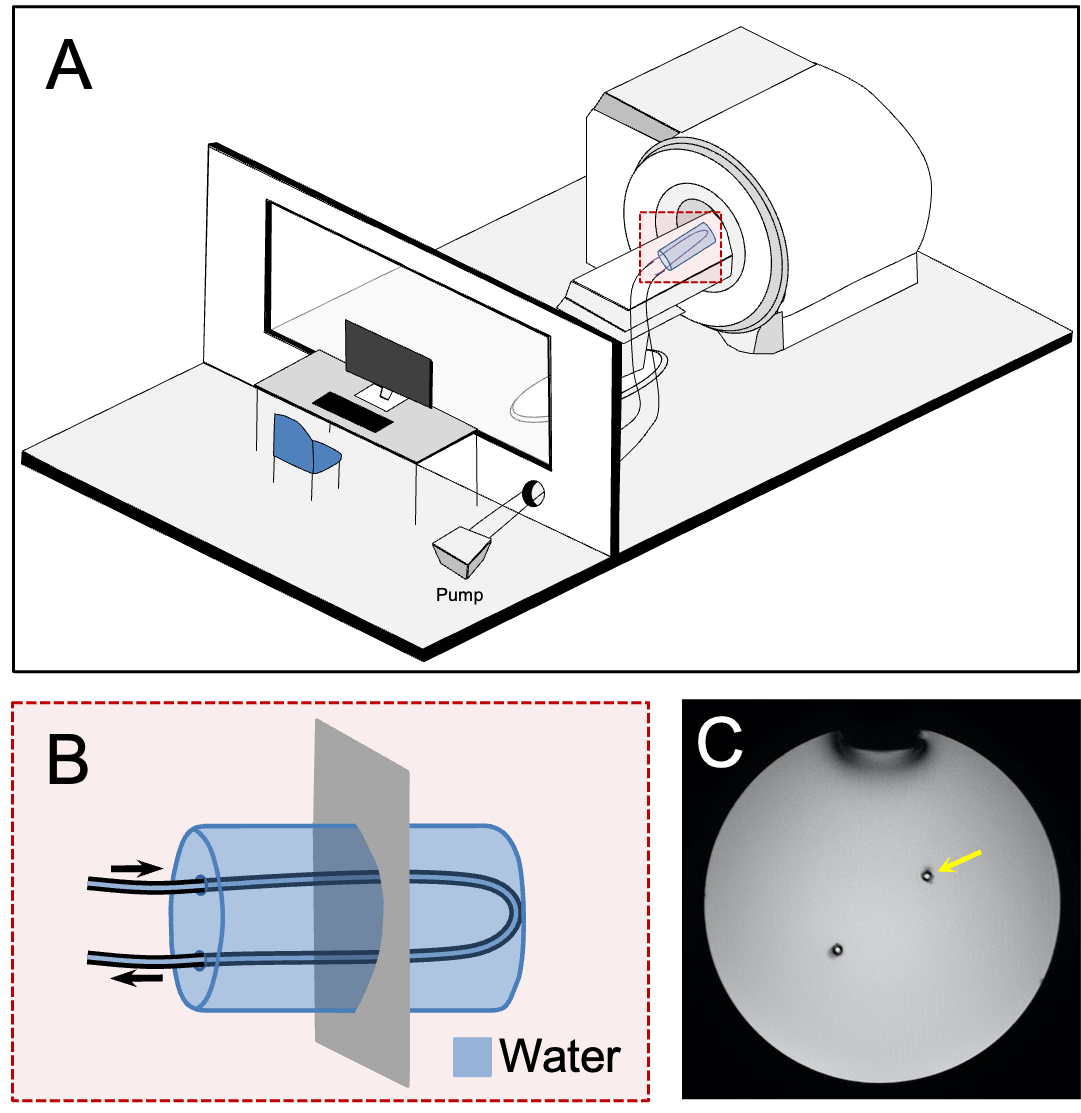
Approach: An MRI phantom was constructed to assess CSF flows between 0-24 cc/hr while in vivo studies measured 21 consecutive patients.
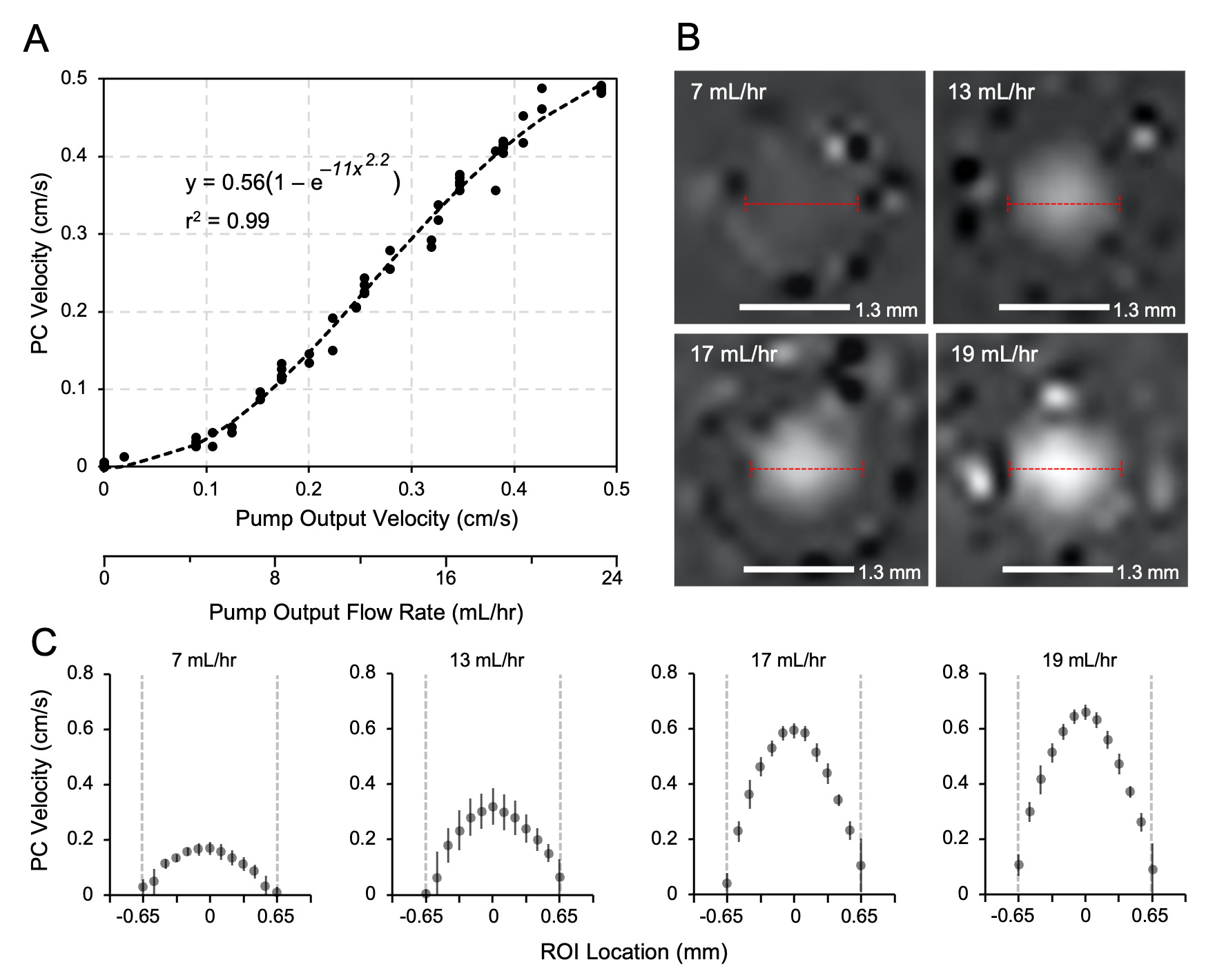
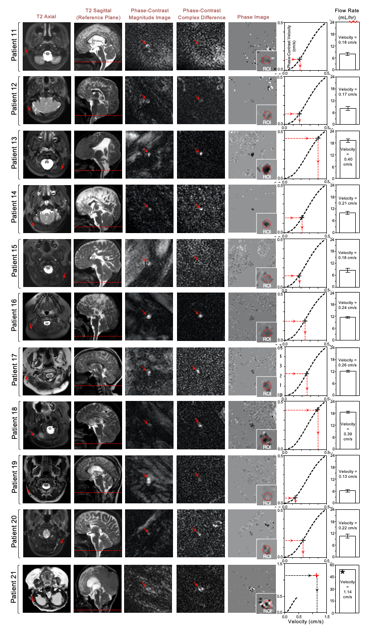
Results: The PC-MRI calibration curve demonstrates a slightly non-linear relationship between flow output by pump and PC-MRI measured velocity. The in vivo patient studies flows ranged between 7 and 54 cc/hr.
Impact: Our work shows that PC-MRI is a non-invasive method for the measurement of CSF flow through the shunt in patients with hydrocephalus. Our work shows that PC-MRI is a promising addition to the clinical setting.
Background
Hydrocephalus is a pathological accumulation of CSF within the brain resulting from a disruption or imbalance of CSF production and absorption.1 The incidence of congenital hydrocephalus is approximately 68 per 100,000 births in the US. Hydrocephalus is the most common condition treated by pediatric neurosurgeons and the most common intervention is the surgical placement of a ventricular shunt, which diverts excess CSF from the ventricles to a distal location in the body where CSF can be resorbed (i.e. the peritoneal space). As hydrocephalus is a chronic condition, patients who receive a shunt require continual clinical follow-up to ensure their shunt is working properly. Shunt malfunction broadly refers to insufficient drainage of CSF due to mechanical failure of the shunt system, resulting in increased intracranial pressure, which can lead to neurological deficit and patient death. Previous studies have found that 30-40% of shunts will fail within the first 2 years of placement.2 A single-institution study found that 84% of patients who receive a shunt required a subsequent operation to revise their malfunctioning shunt at least once in their life,3 and on average, pediatric patients will require 2-3 revision surgeries in their lifetime.4 Existing methods for shunt evaluation are qualitative and some of these methods are invasive.Our work has focused on implementing phase-contrast (PC) MRI, a quantitative sequence, to reliably measure CSF flow through the shunt lumen. Detecting and measuring flow within the shunt lumen can be used to inform clinical decision-making and be applied in future applications to further understand the physiology of patients with CSF disorders. The aim of the work is to demonstrate PC MRI as a valuable adjunct in the clinical monitoring of shunted patients. Our prior work has validated this technique as matching measured output in externalized catheters.5
Methods
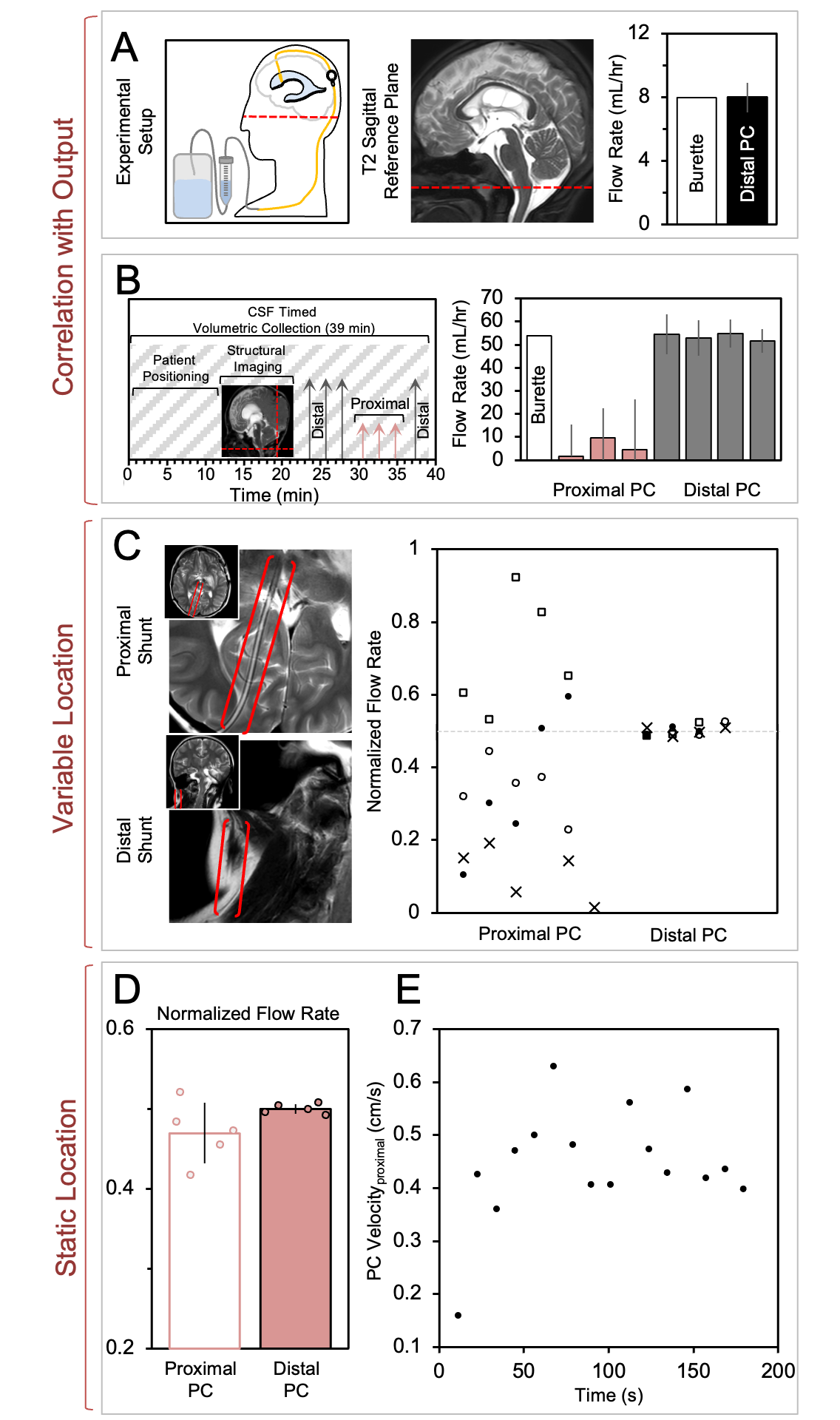
MRI data were collected on two 3T clinical MR scanners (Phillips Achieva) using a 32-channel head coil. The PC-MRI sequence parameters were TR=47 ms, TE=30 ms, field of view 30 × 30 mm, slice thickness=10 mm, NSA=2, matrix 92×91, in-plane resolution 0.20×0.20 mm2, reconstruction x-y voxel dimensions 0.10×0.10 mm2, scan duration=96 s. The PC-MRI sequence was tested using a flow phantom, followed by serial data collection in 21 non-symptomatic patients with a ventricular shunt.5 Slices were prescribed along the catheter orthogonal to the direction of CSF flow, covering either the proximal or distal tubing. Proximal and distal catheter measurements were utilized to successfully identify and eliminate prior sources of error in this technique, and to validate PC-MRI for CSF shunt flow for patients with externalized shunt catheters.Further sequence optimization using compressed SENSE on the Phillips MR software has resulted in a 60-second sequence (38% reduction in scan time). We also present specific cases in which the PC-MRI sequence has been useful in detecting suboptimal or absent flow, leading to a clinical diagnosis of shunt failure.
Results & Discussion
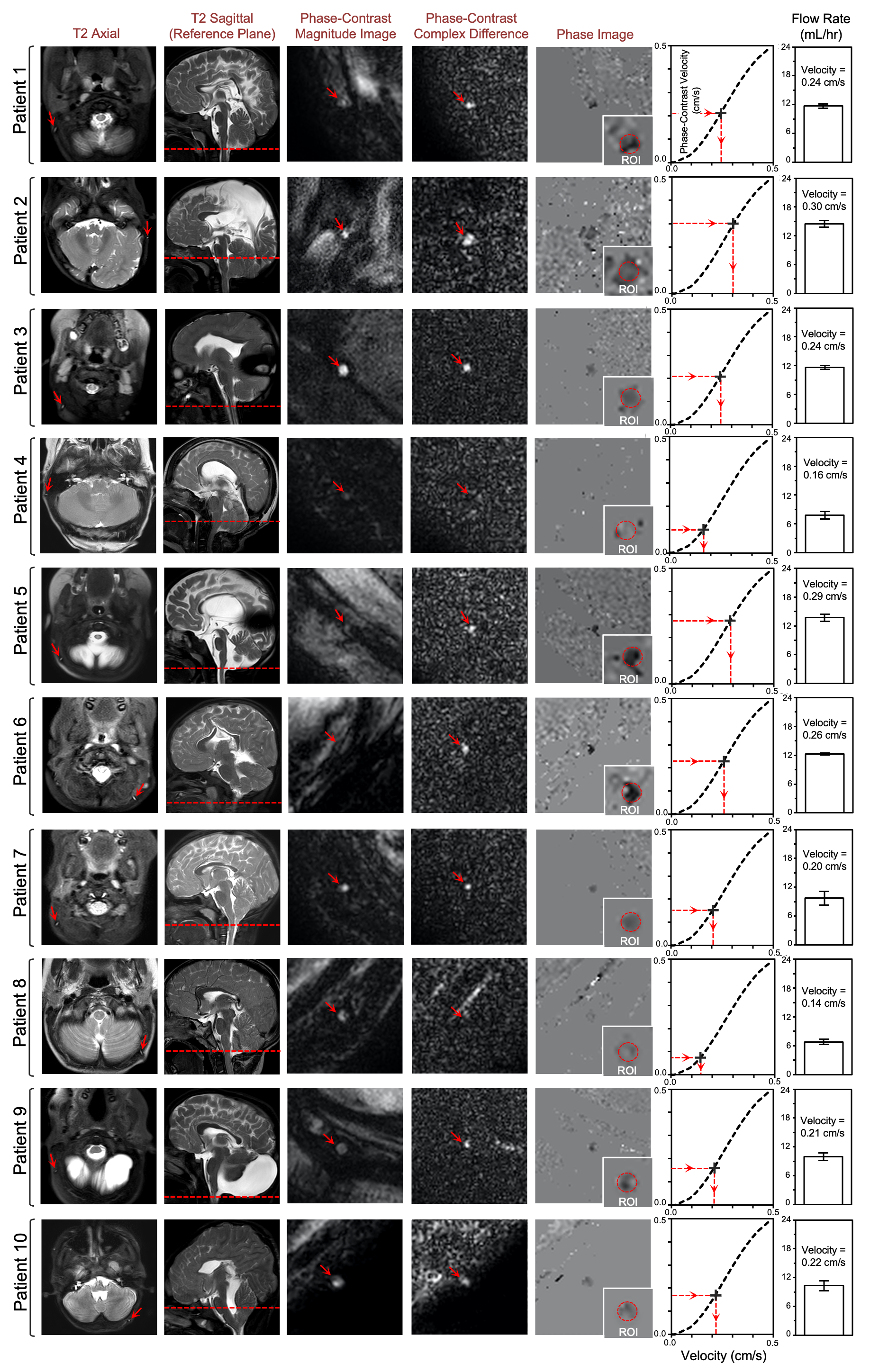
We report results using PC-MRI as an adjunct in the clinical imaging for shunted patients. The current study cohort included 21 patients (10 female, 11 male; age range 11 months to 19 years; median age 6 years). The ranges of measured flow varied from 7-54 mL/hr in patients with functioning shunts. We highlight several examples in which the distal portion of the shunt is determined to be the optimal location for image acquisition, when compared with PC-MRI measurements gathered in the proximal catheter. Furthermore, our study includes the first in vivo validations of PC-MRI for CSF shunt flow by comparing PC-MRI measured flow rate with CSF accumulation in a collection burette obtained in multiple patients with externalized distal shunts. This comparison demonstrates good agreement between flow rate measured by PC-MRI and the burette CSF collection.We highlight the clinical utility of the MR sequence in 8 patients (4 female, 4 male; age range 2 months to 22 years; median age 5 years) whom PC shunt detected absent or suboptimal flow (flow range 0-3 cc/hr) which correlated with an intraoperative finding of proximal catheter shunt obstruction.
Conclusion
The PC-MRI sequence provides simple, accurate, and reproducible clinical measurements of quantitative CSF flow in shunted patients without additional hardware or expense. Our work serves to demonstrate the clinical utility of PC-MRI and its adaptation into the clinical imaging protocols for evaluating shunted patients.Acknowledgements
We thank the Children's Hospital Los Angeles (CHLA) Division of Neurosurgery and Department of Radiology for support. This research was supported through the Rudi Schulte Research Institute.References
1. McAllister JP. Pathophysiology of congenital and neonatal hydrocephalus. Seminars in Fetal and Neonatal Medicine. 2012;17(5):285-294. doi:10.1016/j.siny.2012.06.0042.
2. Drake JM, Kestle JR, Milner R, et al. Randomized trial of cerebrospinal fluid shunt valve design in pediatric hydrocephalus. Neurosurgery. 1998;43(2):294-303; discussion 303-305. doi:10.1097/00006123-199808000-000683.
3. Stone JJ, Walker CT, Jacobson M, Phillips V, Silberstein HJ. Revision rate of pediatric ventriculoperitoneal shunts after 15 years: Clinical article. Journal of Neurosurgery: Pediatrics. 2013;11(1):15-19. doi:10.3171/2012.9.PEDS12984.
4. Reddy GK, Bollam P, Caldito G. Long-Term Outcomes of Ventriculoperitoneal Shunt Surgery in Patients with Hydrocephalus. World Neurosurgery. 2014;81(2):404-410. doi:10.1016/j.wneu.2013.01.0965.
5. Ha JH, Borzage MT, Vanstrum EB, et al. Quantitative noninvasive measurement of cerebrospinal fluid flow in shunted hydrocephalus. Journal of Neurosurgery. 2023;1(aop):1-12. doi:10.3171/2023.7.JNS231326
Figures